Interest of a Three Phase Bone Scintigraphy Protocol in the Diagnosis and Management of Osteoarticular Infections in Children. About 31 Cases
Introduction: Osteoarticular infection is a particularly common pathology in children. The diagnosis is sometimes difficult especially in front of a poor symptomatology and a little disturbed biological assessment. The aim of this work is to assess the contribution of bone scintigraphy in the diagnosis of osteoarticular infections in children. Patients and Method: This is a retrospective study spread out between December 2012 and February 2019, involving children referred to the nuclear medicine department of Hassan II University Hospital Center of Fez for suspected osteoarticular infection. All the children benefited from a bone scan with a triple phase acquisition followed by a study of the entire bone skeleton, after an IV injection of 10 MBq /Kg of MDP-Tc99m. Results: We selected 31 children. The average age was 9.43 years old with a male predominance. The clinical signs mainly found in our patients were fever, bone pain and functional impairment of the affected limb. The main location was the lower limb (74.2%). Bone scan was positive in 70.9% of patients, including 9 cases of septic arthritis, 7 cases of osteomyelitis, 4 cases of sacroiliitis and one case of lumbar spondylodiscitis. Conclusions: Three-phases bone scintigraphy protocole with MDP-Tc99m completed with a whole body bone scan should remain the examination of choice in osteoarticular infections in children. This exam makes it possible to retain an accurate diagnosis in an early stage of OAI while the other medical imaging modalities exams being negative. Thus allowing to prevent severe complications with an affordable financial cost and an acceptable irradiation rate.
Sanae El Mselmi1*, Fabrice Fokoué2, Nadia Abaouz2 and Nadia Ismaili Alaoui2
Introduction
Osteoarticular infection (OAI) is a particularly common pathology in children. It includes osteomyelitis, septic arthritis and osteoarthritis [1]. Its incidence varies between 0.07 and 0.42/1000 children in industrialized countries [2]. This is a diagnostic and therapeutic emergency. Its complications are mainly related to diagnostic delay and / or inappropriate Investigation Paper treatment. Despite progress in imaging, diagnosis at an early stage remains difficult, especially in the face of poor symptomatology and little disturbed biological assessment. Fever and pain are hallmarks of a pediatric osteoarticular infection, although occasionally the signs and symptoms can be more subtile. The use of C-reactive protein to diagnose and validate effective management of treatment has become standard in clinical practice. Above the clinical and Biological
findings, bone scintigraphy with Bisphosphonates labeled with Technetium-99m is a frequently requested examination if a pediatric AOI is suspected. Due to its good sensitivity, the improvement of its specificity and its precocity, it makes it possible to orient the diagnosis while specifying the topography of the infectious process by visualizing the entire bone skeleton without resorting to sedation. This results in faster and more adequate care with a significant reduction in the high cost and duration of treatment. In the Nuclear Medicine Department of CHU HASSAN II in FES, approximately 5% of annual pediatric bone scans are requested for suspected OAI. The aim of this work is to assess the contribution of a triple-phase bone scintigraphy protocol completed by a whole body scan in the early diagnosis of OAI in children.
Patients and Methods
This is a descriptive and retrospective study, carried out over a period of 6 years from December 2012 to February 2019 in the nuclear medicine department of the CHU Hassan II of FEZ. We included children under the age of 16 referred for bone scintigraphy with suspected OAI. We investigated from the files the clinical, biological and radiological data (standard radiography, ultrasound, computed tomography and magnetic resonance imaging).
All the children included in the study underwent a dynamic bone scintigraphy with an acquisition in three phases. Planar images of the vascular inflow were performed immediately after IV injection of the radiotracer, followed by a soft tissue phase 3-10 minutes after. The delayed images were performed 2-3 hours later with static images centered on the suspected area, supplemented by a full-body scan looking for other focus of pathological fixation. The radiotracer used was metastable technetium-99 methylene diphosphonate (99mTc-MDP) injected intravenously, on the examination table, at a dose of 10MBq / Kg. The preparation included sufficient hydration and an empty bladder. An interpretation was made by 02 nuclear medicine physician, supervided by a senior based on the images, considering epidemiological, clinical and paraclinical data of the patients. Images acquisition was performed with a Siemens dual head Gamma Camera, Symbia T6 2010 model. OAI was suspected on pathological fixation relating to the three stages of the examination.
Results
Thirty-one patients were collected. The average age was 9.43 years with extremes ranging from 9 months to 15 years old. 74.1% of the patients were male with a sex ratio (M / F) of 2.8. A history of recent infection was found in 12.9% of the children. The notion of trauma was reported in 5 children.
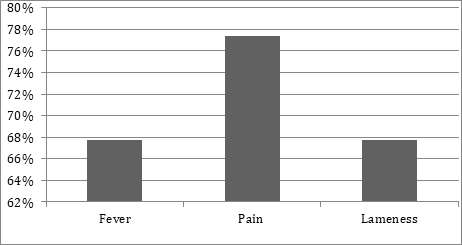
The clinical signs mainly found were bone pain, fever, and lameness (Figure 1). OAI were predominant in the lower limb, 74.2% of cases (Table 1).
| Localisation | Number of cases | Percentage (%) |
|---|---|---|
| Upper limb | 1 | 3,2 |
| Spine | 1 | 3,2 |
| Hip | 6 | 19,4 |
| Lower Limbs | 23 | 74,2 |
| Total | 31 | 100 |
Table 1: Distribution of patients by location.
Among the 19 children who underwent a laboratory assessment, a biological inflammatory syndrome with hyperleukocytosis associated with an elevation of C reactive protein was present in 12 cases (63.1%), 4 children (21 %) had an increase in CRP without leukocytosis while 3 children (15.7%) had a normal biological inflammatory assessment. A standard radiograph of the affected limb was taken in 19 patients, showing radiologic signs suggestive of OAI in 57.14% of cases. The radiological signs identified were bone demineralization and a periosteal reaction. Ultrasound was performed in 12 children, 6 of whom had ultrasound signs suggestive of osteoarticular infection, namely periosteal detachment, joint effusion or infiltration of soft tissue. The tomodensitometry carried out in 5 children, concluded with an OAI in 3 cases.
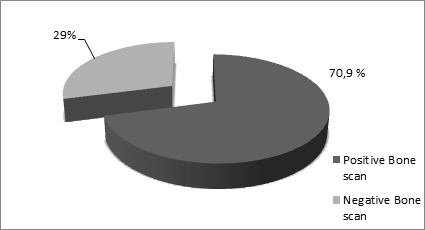
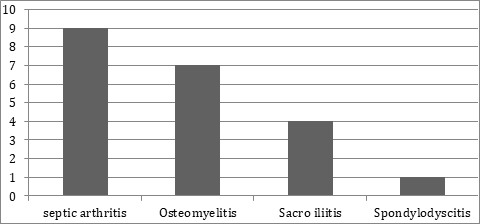
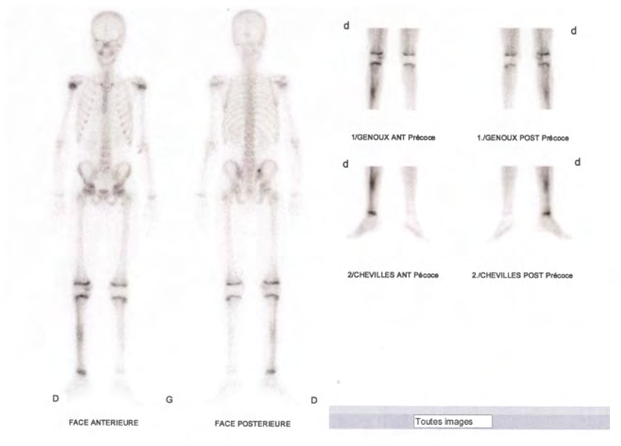
The 99mTc-MDP bone scintigraphy was positive in 22 children (70.9%) (Figure 2), showing a relative hyperactivity of the affected limb at the two stages of the examination (early and late) in favor of an OAI, including 9 cases of septic arthritis, 7 cases of osteomyelitis, 4 cases of sacroiliitis and one case of lumbar spondylodiscitis (Figure 3).
Among the 19 children who performed conventional imaging, 14 patients (73.6%) had a positive bone scan. As for imaging, it had found radiological signs in favor of an OAI in only 12 cases (63.1% of cases) (Table 2).
| Normal Bone scan | Positive | Total | |
|---|---|---|---|
| Conventional imaging | |||
| Normal | 1 | 6 | 7 |
| Positive | 4 | 8 | 12 |
| Total | 5 | 14 | 19 |
Table 3: Comparison between the results of conventional imaging and those of bone scan Among the 19 children who underwent an inf
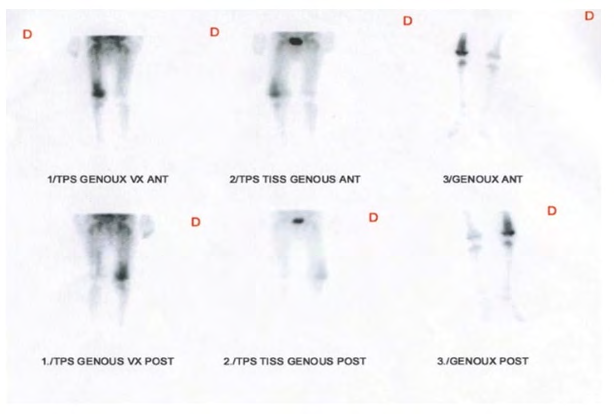
Table 2: Comparison between the results of conventional imaging and those of bone scan Among the 19 children who underwent an inflammatory laboratory assessment, 3 cases had a normal inflammatory assessment with scintigraphic signs in favor of an osteo- articular infection. Also, 3 patients presented a biological inflammatory syndrome while the bone scintigraphy did not show scintigraphic signs in favor of an OAI (Table 3, Figures 4 & 5).
| Normal Bone Scan | Positive | Total | |
|---|---|---|---|
| Disrupted inflammatory assessment | 3 | 13 | 16 |
| Normal inflammatory assessment | 0 | 3 | 3 |
| Total | 3 | 16 | 19 |
Table 2: Comparison between the results of the biological assessment and those of the bone scan.
Discussion
Osteoarticular infection in children is a considerable diagnostic and therapeutic challenge. The consequences of a delayed or missed diagnosis could lead to significant functional complications. This pathology takes on several aspects depending on the clinical presentation and the site of infection. OAI affects children of all ages, from newborns to older children [3] with an average age of onset varying according to the studies [4, 5, 6, 7]. The average age of our sample was 9.43 years old. In OAI, the predominance is male [4, 5, 6] and it was the same for our study with a sex ratio of 2.8.
The classic location of OAI is the lower limb [1, 2, 8, 9]. It was 74.2% in our series. According to the litterature this location can be multifocal in about 13 % of children concerning with OAI [10, 11]. In our study, we found no cases of multifocal involvement. The concept of trauma has been found in 30-40% of cases in most studies [4, 12, 13]. In our study, a history of trauma was reported in approximately 16% of cases.
The diagnosis of OAI is suspected in a child admitted with febrile, helpless, abrupt onset or rapidly progressive osteoarticular pain syndrome. The Fever is an important clinical element pointing to an infectious aetiology. According to the litterature, fever is only present in 60 to 80% of cases [7, 14]. In our study fever was present in 63.6% of OAI cases. Its absence does not exclude the diagnosis of OIA in children.
Biological inflammatory syndrome associating hyperleukocytosis and elevated C-reactive protein (CRP) is inconstant in childhood OAI [13, 15]. However, these markers are not always reliable. Hyperleukocytosis is generally present in only 50% of infected children [16]. Also, elevation of CRP is found in around 80% of cases [1]. In our study, around 63.1% of children with confirmed AOI were having a biological inflammatory syndrome.
Medical Imaging plays an important role in the diagnostic orientation of osteoarticular infections. The choice of the most appropriate imaging modality based on the clinical presentation is very important in making the diagnosis and assessing the extent of the disease. Thus, standard x-rays, ultrasound, bone scintigraphy and MRI are discussed, each with its advantages and limitations. Radiography centered on the affected limb is the first-line, urgent and systematic examination. This is an insensitive examination [17] and frequently normal in the early stage of infection. In the case of acute osteomyelitis, X-rays can show extra osseous signs that appear early during the first 48 to 72 hours of infection [18].
However, these signs are neither sensitive nor specific and therefore of little use in practice [11, 18]. The first bone signs appear late after 7 hours to 10 days of progression, which includes resorption under the periosteum and clarity under cortex, indicating bone demineralization [19]. In septic arthritis, it is most often normal and above all makes it possible to rule out a differential diagnosis (osteomyelitis, bone tumor or fracture). In our series, 57.1% of cases had radiographic abnormalities suggestive of OAI.
Ultrasound is a simple, non-invasive, non-irradiating, inexpensive, sensitive and available examination, but it remains operator-dependent. It may be normal in the early stage of OAI, especially with acute osteomyelitis [18, 20]. Its interest lies in the search for a complication, in particular the subperiosteal abscess, or of the soft tissues in the event of acute osteomyelitis and in demonstrating an intra-articular effusion in the event of septic arthritis. In our series, this examination made it possible to orient the diagnosis in 5 cases of septic arthritis, 16.1% of cases, by showing an intra- articular effusion and in one case of acute osteomyelitis by showing a periosteal detachment.
MRI is a non-irradiating, non-invasive, but expensive means of imaging. This is a very sensitive test, around 97% [17]. However, its specificity varies from one study to another [21, 22]. This examination is reserved for certain indications, especially in spondylodscitis and sacroiliitis, and in the event of failure of antibiotic therapy adapted to the search for a complication (abscess) [11, 12]. In our study, no child did an MRI.
Bone scintigraphy with bisphosphonates labeled with metastable technetium-99 in 3 states is a very useful test in the diagnosis of OAI. It allows early diagnosis of OAI. In fact, the technical diphosphonate derivatives are markers of bone remodeling and bone perfusion [23, 24, 25], which makes it possible to detect bone remodeling anomalies in the first 48- 72 hours of infection before the appearance of radiological anomalies. . Its sensitivity varies according to the studies (84-100%) [18]. A normal bone scintigraphy excludes bone infection with a strong negative predictive value (close to 100%) [12].
In our sample, 99mTc-MDP bone scintigraphy made it possible to diagnose OAI in 22 children (70.9%) including 9 cases of septic arthritis, 7 cases of osteomyelitis, 4 cases of sacroiliitis and one case of lumbar spondylodiscitis. This low-irradiation examination also makes it possible to explore the entire bone skeleton using whole-body imaging, which is useful in the event of double localization of the infection, in around 7% of children, especially in newborns [23].
The examination is performed in three phases, the vascular phase which reflects the blood supply to the area explored, the tissue phase which reflects activity in adjacent tissues and the bone phase which reflects osteoblastic activity [26, 27, 28]. The classic scintigraphic appearance during OAI is early hyperemia in vascular time, associated with hypercaptation in tissue time and late hyperfixation of the radiotracer in bone time due to hypervascularization of the infectious site [10, 28].
Although performing the three-phase bone scintigraphy improves the specificity of the examination (approximately 90%), it does not differentiate an osteoarticular infection from a tumor or traumatic injury [28, 29].
To further improve its specificity, some authors recommend making a 4th acquisition at the 24th hour because the infected bone continues to bind 99mTc diphosphonate until the 24th hour [30, 31], others recommend ‘’ use of certain markers specific to infection, in particular gallium-67 citrate, leukocytes labeled with Indium 111 or with hexamethylpropylene-amine-oxime (99mTc- HMPAO) and anti-granular antibodies labeled with 99mTc (Leukoscan) [28, 30], but these examinations are not possible in our routine [32].
Conclusion
The three-phase bone scintigraphy protocol with metastable technetium-99 methylene diphosphonate (99mTc-MDP) completed by a whole body scan should remain the gold standard exam if an OAI is suspected in children. It makes it possible to diagnose OAI in an early stage when the morphological assessment may still be negative and thus improve the initial management and eventually the follow up of children affected by this condition in order to avoid severe complications with an affordable financial cost and an acceptable irradiation rate.
Declaration of Patient Consent
The authors certify that they have obtained the appropriate patient consent.
Financial Support
Nil
Conflicts of Interest
The authors declare no conflict of interest.
References
-
Timsit S, Pannier S, Glorion C, Chéron G (2005) Bacterial osteoarticular infections in infants and children: one year experience acute osteomyelitis and septic arthritis in children: one year experience. Arch Pediatr 12(1): 16- 22.
-
Grimprel E, Cohen R (2007) Epidemiology and physiopathology of osteoarticular infections in children (newborns except). Arch Pediatr 14(2): 81- 85.
-
Teklali Y, Ettayebi F, Benhammou M, Alami ZF El, Madhi EL T, et al. (2002) Septic arthritis in infants and children about 554 cases. Journal of Pediatrics and Childcare 15(3): 137-141.
-
Cadilhac C, Clavier F, Pannier S, Chéron G, Glorionet CH, et al. (2007) Osteoarticular infections in children. Emergency Medicine 1-10.
-
Trifa M, Bouchoucha S, Smaoui H, Frikha M, Marzouk SB, et al. (2011) Microbiological profile of haematogenous osteoarticular infections in children. Orthop Traumatol Surg Res 97(2): 186-190.
-
Arias MG, Balsa A, Mola EM (2011) Septic arthritis. Best Pract Res Clin Rheumatol 25(3): 407-421.
-
Lemoine A, Baudin F, Vialle R, Grimprel E (2016) Treatment and evolution of community acute musculoskeletal infections in healthy children: single- center retrospective study of 64 cases. Pediatrics Archives 23(11): 1124-1133.
-
Vial J, Gandois HC (2012) Limb infections in children and adults. Diagn Interv Imaging 93(6): 530-546.
-
Bouchoucha S, Drissi G, Trifa M, Saied W, Ammar C, et al. (2012) Epidémiologie des ostéomyélites aigües hématogènes communautaires de l’enfant : Etude Prospective sur 32 mois. La Tunisie Médicale 90(0607): 473-478.
-
Bonhoeffer J, Haeberle B, Schaad B, Heininger U (2001) Diagnosis of acute haematogenous osteomyelitis and septic arthritis: 20 years’ experience at the University Children’s Hospital Basel. Swiss Med Wkly 131(39-40): 575-581.
-
Jaramillo D, Treves ST, Kasser JR, Harper M, Sundel R, et al. (1995) Osteomyelitis and Septic Arthritis in Children: Appropriate Use of Imaging to Guide Treatment. Am JR Roentgenol 165(2): 399-403.
-
Connolly LP, Connolly SA, Drubach LA, Jaramillo D, Treveset ST (2002) Acute Hematogenous Osteomyelitis of Children: Assessment of Skeletal Scintigraphy–Based Diagnosis in the Era of MRI. J Nucl Med 43(10): 1310- 1316.
-
Ghachem MB (2008) Quoi de neuf dans les infections ostéoarticulaires hématogènes aigues de l’enfant ?. In: Conférences d’enseignements. Paris: Elsevier Masson SAS: 219-238.
-
Wagner N, Ceroni D, Niederer A, Ritz N, Relly C, et al. (2017) Prise en charge des infections ostéo-articulaires aigües de l’enfant. Paediatrica 28(1): 8-12.
-
Gras G, Druon J, Floch S, Bernard L (2014) Infection ostéoarticulaire. Encycl Med Chir (Traité de medecine) AKOS. Paris: Elsevier Masson SAS: 1-11.
-
Dartnell J, Ramachandran M, Katchburian M (2012) Haematogenous acute and subacute osteomyelitis: a systematic review of the literature. J Bone Joint Surg Br 94(5): 584-595.
-
Dutronc H, Bocquentin F, Dupont M (2004) Contribution of imaging to the diagnosis of osteoarticular infection. Medicine and Infectious Diseases 34(6): 257-263.
-
Azouz E (2003) Infections in bone. In: Kuhn JP, Slovis TL, Hailer JO (Eds). Caffey’s Pediatric Diagnosis Imaging, 10th (Edn.), Vol. II, Philadelphia: Mosby, pp: 2343-2373.
-
Blickman JG, de Rooy JW (2004) Current imaging concepts in pediatric osteomyelitis. Eur Radiol 14(4): 55-64.
-
Riebel TW, Nasir R, Nazarenko O (1996) The value of sonography in the detection of osteomyelitis. Pediatr Radiol 26(4): 291-297.
-
Azoulay R, Alison M, Sekkal A, Sebag G, Adamsbaum C (2007) Imaging of bone and joint infections in childrenImaging of child osteoarticular infections. Arch Pediatr 14(Suppl 2): 113-121.
-
Vittorini E, Del Guidice E, Pizzoli A, Caudana R (2005) MRI versus scintigraphy with 99mTc-HMPAO labbeled granulocytes in the diagnosis of bone infection. Radiol Med 109(4): 395-403.
-
Goergens ED, McEnvoy A, Watson M, Barrett IR (2005) Acute osteomyelitis and septic athritis in children. J Paediatr Child Health 41(1-2): 59-62.
-
Alison M, Tanase A, Rega A, Gabor F, Tilea B, et al. (2014) Imaging of osteo-articular infections in children. Arch Pediatr 21: 174-175.
-
Rouy JC, Tafani M, Guillet J (2012) Nuclear medicine and paediatrics: Radiopharmaceutical the point of view. Med Nucl 36(3): 124-127.
-
(2012) Guidelines for writing protocols for bone scintigraphy. Med Nucl 36(11): 687-697.
-
Brenner AI, Koshy J, Morey J, Lin C, DiPoce J (2012) The Bone Scan. Semin Nucl Med 42(1): 11-26.
-
Love C, Din AS, Tomas MB, Kalapparambath TP, Palestro CJ (2003) Radionuclide bone imaging: an illustrative review. Radiographics 23(2): 341-358.
-
Palestro CJ, Torres MA (1997) Radionuclide imaging of orthopedic infections. Semin Nucl Med 27(4): 334-345.
-
Maurer AH, Chen DC, Camargo EE, Wong DF, Wagner HN, et al. (1981) Utility of Three-Phase Skeletal Scintigraphy in Suspected Osteomyelitis: Concise Communication. J Nucl Med 22(11): 941-949.
-
Goldsmith SJ, Vallabhajosula S (2009) Clinically Proven Radiopharmaceuticals for Infection Imaging: Mechanisms and Applications. Semin Nucl Med 39(1): 2-10.
-
Demopulos GA, Bleck EE, McDougall IR (1988) Role of radionuclide imaging in the diagnosis of acute osteomyelitis. J Pediatr Orthop 8(5): 558-565.
- Contribution of 18FDG PET in Atypical HORTON Disease
- Living Conditions, Healthy Practice and State of Households of a Town Rural in Colombia
- Background to the Health and Safety Regulation at Work in Colombia
- Risk Factors Psychology Workers Sena (Center for the Petrochemical Industry) Regional Bolívar, Colombia
- Diffuse Intense Pleural FDG Uptake with Smooth Thickening: A MARKER of Tuberculosis in Isolated Pleural Effusion
- Hypermetabolic Splenomegaly with Infarct in FDG PET/CT: A Clue to Scrub Typhus in PUO