Cerebral Hydatid Cysts: A Case Series
Introduction: Echinococcosis (hydatid disease or hydatidosis) is a cosmopolitan anthropozoonosis common to both humans and herbivorous animals. Cerebral hydatid cyst is very rare accounting for only 0.5 to 3% of all cases. They represent about 1-2% of all intracranial lesions. Fifty to seventy five percent of the patients suffering from echinococcosis are children and young adults. Materials and Methods: This retrospective study included four patients who were treated for intracranial hydatid cysts between 2016 and 2019, in Neurosurgery department, CHU Mohammed VI, Oujda, Morocco. They were three male children and one young female, aged between 3 and 22 years, with an average age of 10, 75. Increased intracranial pressure and seizure represent the most common symptoms. Patients were evaluated with MRI (1.5 T), and underwent a chest X-ray, echocardiography and abdominal CT scan and ultrasound to reveal any other locations. All lesions were surgically removed and received medical treatment. Results: The cysts were successfully removed using the Dowling technique. The postoperative period was uneventful no complications observed, seizures were not seen during follow-up. Conclusion: This report aims to emphasize the clinical, radiological and therapeutic features related to this infectious condition that involves the central nervous system with a literature review.
Introduction
Hydatid disease is a common parasitic disease in the highly endemic countries of North Africa, Middle East and Central Asia. The pathogenic agent is hexacanth embryo of echinococcus granulosus. It is accidentally transmitted to humans either through the ingestion of infected food, or following direct contact with a definitive host, usually a dog. Fifty to 75% of the patients infected with echinoccocus, are children and young adults [1, 2, 3, 4]. The liver is the favored site of hydatid disease (77%) [5, 6]. Intracranial hydatid cysts account for only 0.5 to 3% of all cases of hydatid disease and contribute to 1 to 2% of all intracranial space lesions [3, 4, 5, 6, 7]. This report includes 4 patients suffering from cerebral hydatid cysts operated between 2016 and 2019, three children of 03, 04, and 14 years old, and a young woman of 22 years old. The symptoms and clinical signs have been reviewed. All patients received 1.5 T MRI, and brain CT scan for diagnosis of cerebral cyst. A chest X-ray, an abdominal and cardiac ultrasound was performed to find any other visceral localization. The Dowling technique (improved by Arana-Iniguez and San Julian) has been widely used for the excision. Follow-up and postoperative complications were documented, and the results were assessed in the short and long term.
Cases
Patient 1
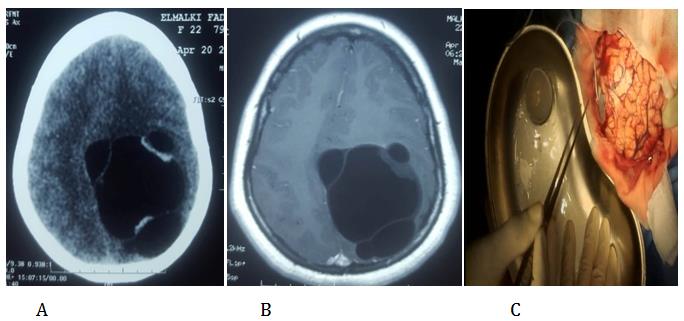
A 14-year-old boy with a history of unlabeled frequent occurrence of headache, nausea and vomiting was admitted to the emergency room for a generalized tonic- clonic seizure. On examination, the main author identified a left hemiparesis with aphasia, bilateral papilledema and vision disorders. No other physical abnormalities were observed. The T1- and T2-weighted Magnetic Resonance Imaging and the CT-scan of his brain showed a well circumscribed spherical cystic lesion of the right parietal area. No calcification or wall enhancements were seen. The development of the cystic lesion was at the origin of a mass effect, consistent with a diagnosis of a hydatid cyst (Figures 1A-C). Chest X-ray and abdominal and pelvic ultrasound and CT-scan were all within normal standards for the patient’s age and sex. The result of the serologic test (ELISA) was negative. The patient received anticonvulsants and the seizures were controlled. The cyst was then completely removed using the technique of hydrodissection as described by Arana-Iniguez. The cyst membrane remained intact (Figure 2). The histopathologic examination of the surgical specimen found a giant cyst with its ectocyst in the shape of lamellated chitinous membrane consistent with a hydatid cyst. Albendazole per os (15 mg/kg twice daily) was prescribed for three months after the surgery. Postoperative CT scan revealed no residual cyst. No recurrence was observed during 2 years of the follow-up.
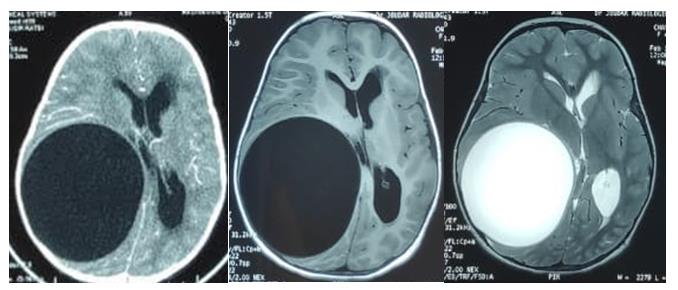
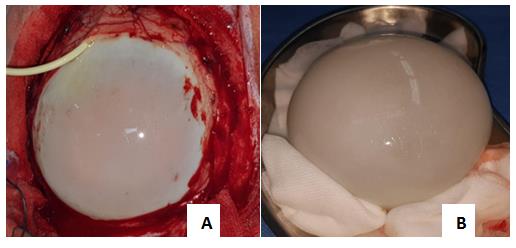
Figure2: Hydrodissection of the cyst (A) macroscopic aspect of intact hydatid cyst after removal (B).
Patient 2
A 4-year-old boy was admitted to the emergency room for an increased intracranial pressure: severe headache and vomiting for three days. Four months earlier, the child was suffering from intermittent headaches and progressive intellectual impairment. On admission, the neurological examination revealed a slight left hemiparesis, with bilateral papilledema. CT-scan and MRI showed a spherical cystic lesion of the right frontoparietal region, measuring 05, 5 mm / 7.5mm / 8.5 mm (Figure 3). The enzyme-linked immune sorbent assay (ELISA) was positive. Radiological imaging including chest and abdominal CT showed no abnormalities. The cyst was then removed surgically without rupture. Medical treatment (Albendazole 15 mg / kg three times a day) was prescribed for 3 months. The postoperative period was an uneventful. A follow-up of 3 years was carried out with no recurrence and with a good clinical evolution.
Patient 3
A 3-year-old boy with no relevant medical history presented to the emergency room with a focal seizure on the left side of the body. This seizure lasted for 5 min and evolved to a generalized tonic-clonic seizure. The child’s parents reported he was suffering from headache and nausea for the last month. On neurological examination, there was no focal deficit and intracranial pressure was within normal range for the age and sex. The examination of the fundus found no abnormalities, and so was the examination of other systems of the body.
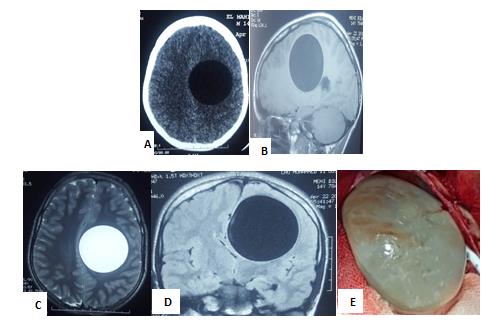
T2-and T1-weighted magnetic resonance imaging and CT-scan showed a well-circumscribed defined, spherical cystic lesion in of the right parietal lobe with no out calcification or and no enhancement of the wall, easily these images and the general context were first pointing towards suggestive of the diagnosis of a hydatid cyst (Figure 4). Chest X-ray and thoracic and abdominal Computed tomography CT-scan, demonstrated found many well defined cavitary lesions in the left lower lobe of the left lung. Abdominal ultrasound and CT-scan, showed several associated to liver cystic lesions in the liver assisted by abdominal ultrasound, which shows several cystic lesions in the liver measuring 25 mm/20, 20 mm/18 mm and 15mm/12 for the biggest. These lesions in the lungs and the liver were highly suggestive of a hydatid disease. The enzyme-linked immune sorbent assay (ELISA) for Echinococcus was positive.
The child was immediately put on anticonvulsants to control this seizure. He underwent surgery afterwards to remove the cerebral cyst using the hydropulsion technique. The cyst was removed and checked to be intact. Histopathologic examination of the surgical specimen showed a cyst wall with ectocyst as lamellar chitinous membrane consistent with a hydatid cyst. Postoperative albendazole (15 mg / Kg) twice a day was started Antiepileptic treatment was prescribed for 6 months. The postoperative period was an uneventful.
Hepatic and pulmonary cysts have not been were treated medically. Brain CT-scans were performed in the follow- up. They failed to show any residual cyst in the brain.
Patient 4
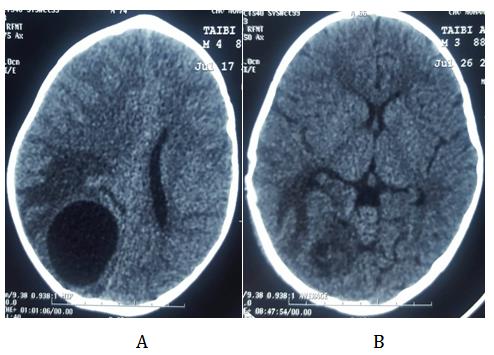
A 22-year-old woman with no medical history presented to the emergency department for a right partial seizure followed by a generalized tonic-clonic seizure. The patient’s family reported that she was suffering from headaches, vomiting and visual disturbances for the last 10 months. When asked, the patient reported a feeling of progressive heaviness in her right upper and lower limbs. This feeling was aggravated after each epileptic seizure. Clinical examination after the seizure was controlled revealed a bilateral papilledema with a right hemiparesis. Brain CT-scan revealed multiple calcified lesions of the left fronto-parietal region. T1-and T2-weighted MRI of the brain showed a large well-defined T2 hyperintense lesion measuring 84x90x60 mm with multiple well defined intra-lesional cysts in the left fronto-parietal lobe causing mass effect. These finds were consistent with multiple hydatid cysts. Thoraco-abdominal ultrasound was normal. The hydatid serology was negative. The diagnosis of hydatid cyst was retained. The patient underwent surgery to remove the brain cyst using the hydropulsion technique. Albendazole 400 mg twice a day and antiepileptic drugs were prescribed for 3 months. No complications were noted postoperatively. No recurrence was observed in the short- and long-term of follow-up (Figure 5).
Discussion
Hydatid disease or hydatidosis is a common anthropozoonosis in the endemic countries of North Africa, Central Asia and the Middle East [6]. Humans can be accidental intermediate hosts by ingesting food contaminated by Echinococcus cestode or by direct contact when petting an infested dog which is the main host of the parasite. The most affected organs are the liver (77%) and the lung (43%) [8]. Cerebral hydatid cysts are rare accounting for only 0.5% of all cases of hydatid disease. They contribute to 1-2% of all intracranial processes in endemic countries. Fifty to 75% of these patients are children and young adults, with a male predominance in most series reported in the literature [2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13]. Most cerebral cysts are located in the supratentorial structures affecting mainly the parietal lobe, in the vascular territory of the middle cerebral artery [9]. In the current series, all patients had a parietal hydatid cyst extending over to the adjacent frontal lobe. These cysts in the brain can occur as solitary lesions, especially in children. They can also present as multiple or multilocular lesions limited to the brain or involving other organs like liver and lungs.
These cysts can be single solitary lesion which is common in children or multiple, or primary or secondary. Primary hydatid cysts occur because of the direct invasion of the brain, after the liver and the lung fail to filter ecchinococcus larvae. They are usually solitary and fertile. Secondary hydatid cysts occur as a result of the disruption of one or more primary cysts in others organs. The embryos pass through the liver and reach various organs including the central nervous system, cranium and vertebrae by systemic circulation [7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23]. Multiple cerebral hydatid cysts are rare. Most of them are due to spontaneous or traumatic/surgical rupture of a viable primary lesion with spreading of the scolices inside the cerebral parenchyma [11, 12]. The cysts require several years of evolution to become large enough to cause symptoms. Symptomatic hydatid cysts present with symptoms and signs related to increased intracranial pressure [10]. The most common symptoms are headache and vomiting [5]. Other signs include: seizures, focal deficit, papilledema, ataxia, visual deficit, hemi-paresis and disturbed conscious level. Hydrocephalus may occur if the ventricular system is blocked in the latter stages.
The diagnosis of cerebral hydatid cyst is established by neuroimaging. MRI is considered superior to CT in the diagnosis and the localization of hydatid cysts. MRI and CT-scan show a well-defined, usually solitary, cystic lesion with cerebrospinal fluid like density, with no or minimal enhancement, rarely calcified, present in the middle cerebral artery territory. The lesion, when large, may cause mass effect and parenchymal distortion [11, 12, 13, 14, 15]. Old cystic lesions with different ages that are reported mainly in adults are often secondary and result often from spontaneous, traumatic or surgical disruption of a solitary primary cyst [16, 17]. The diagnosis can be supported by serological tests (ELISA) which has a sensitivity of 85%. Definitive diagnosis of a hydatid disease is based on histopathological findings. [13] Differential diagnosis includes other infectious cystic lesions of the central nervous system, such as: neurocysticercosis; brain abscesses; porencephalic cysts; arachnoid cysts and cystic tumors of the brain [18, 19]. Cerebral hydatid cyst is associated with cysts in the liver and/or the lungs in 20% of cases [20, 21]. Ciurea, et al. [22] reported 29.6% of extracerebral localization. Coman, et al. [22] reported that the spleen, the liver and the lungs were affected in 17.4% of the patients who have a cerebral hydatid cyst. In the current study only one patient had a hepatic and pulmonary hydatidosis.
Surgical enucleation without disrupting the cyst wall is the treatment of choice. Reaching this goal is not always easy because the cyst membrane is often fragile. The preferred method is by using hydrodissection following the Dowling technique. Recurrence is directly related to the disruption of the cyst. The extent of the bony flap and the cortical incision should then be proportionate to the diameter of the cyst. The rate of successful removal of an intact hydatid cyst is around 60–70% [23]. Albendazole and praziquantel are the medical treatment of choice. In recurrent cases or cases with rupture during surgery, medical therapy has been reported to be effective. Preoperative and postoperative albendazole may be considered to sterilize the cyst, decrease the chance of anaphylaxis, lower the tension in the cyst wall, and reduce the recurrence.
In the current series, the patients underwent surgery for cyst removal using hydrodissection. All cysts were completely removed with their membrane intact (intraoperative fig: 1-2-3-4). No postoperative complications were observed. Oral albendazole (10– 15 mg/kg/day for 3–6 months) and antiepileptic drugs were systematically administered to all patients. There were no side effects related to albendazole. The histopathologic examinations of the surgical specimens were all consistent with the diagnosis of hydatid cyst. The clinical follow up and a series of CT- scans showed no residual cyst in the brain of any of the patients during the follow- up.
Conclusion
Intracranial hydatid cyst remains a common condition in endemic locations. They should be evoked in the differential diagnosis of any intracranial cyst, especially in children having close contact with dogs. Surgery and chemotherapy aim for a recurrence free outcome. Postoperative follow-up is mandatory, however, giving those recurrences and complications may occur later. In our series we obtained good results through proper care. However extensive health awareness-raising campaigns are needed to reduce the occurrence of this disease.
References
-
Yasar B, Serdar K, Hasan N, Umit O, Adnan C, et al. (2004) cerebral hydatid disease: CT and MR imaging findings. Swiss Med WKLY 134(31-32): 459-467.
-
Trivedi A, Shukla S, Singh K, Sharma V (2007) Giant intracranial hydatid cyst. J Pediatr Neurosci 2(2): 72- 74.
-
Onal C, Unal F, Barlas O, Izgi N, Hepgul K, et al. (2001) Long-term follow-up and results of thirty pediatric intracranial hydatid cysts: half a century of experience in the Department of Neurosurgery of the School of Medicine at the University of Istanbul (1952-2001). Pediatr Neurosurg 35(2): 72-81.
-
Cavusoglu H, Tuncer C, Ozdilmaç A, Aydin Y (2009) Multiple intracranial hydatid cysts in a boy. Turk Neurosurg. 19(2): 203-207.
-
Mala R, Ananth ML, Nagaraju BN, Rao CV ( 2014) Intracranial hydatid cysts-some rare presentations of cases. J NTR Univ Health Sci 3(4): 263-266.
-
Shivani Randev, Vipin K Gupta, Pankaj Kumar, Vidushi Mahajan, Suresh K. Angurana, et al. (2018) Brain Hydatid in a Child: the journal of pediatrics 199: 280.
-
Altınörs N, Bavbek M, Caner HH, Erdogan B (2000) Central nervous system hydatidosis in Turkey: a cooperative study and literature survey analysis of 458 cases. J Neurosurg 93(1): 1-8.
-
Erşahin Y, Mutluer S, Güzelbag E (1993) Intracranial hydatid cysts in children. Neurosurgery 33(2): 219- 224.
-
Arora SK, Aggarwal A, Datta V (2014) Giant primary cerebral hydatid cyst: a rare cause of childhood seizure. J Pediatr Neurosci 9(1): 73-75.
-
Shih RY, Koeller KK (2015) Bacterial, fungal, and parasitic infections of the central nervous system: radiologic-pathologic correlation and historical perspectives. Radiographics 35(4): 1141-1169.
-
Banzo J, Diaz FJ, Pina JI, Abós MD, Rios G, et al. (1984) Multiple cerebral hydatid cysts. Eur J Nucl Med 9(12): 561-563.
-
Boles DM (1981) Cerebral echinococciasis. Surg Neurol 16(4): 280-282.
-
Binesh F, Mehrabanian M, Navabii H (2011) Primary brain hydatosis. BMJ Case Rep.
-
Tuzun Y, Kadioglu HH, Izci Y, Suma S, Keles M, et al. (2004). The clinical, radiological and surgical aspects of cerebral hydatid cysts in children. Pediatr Neurosurg 40(4): 155-160.
-
Pasaoglu A, Orhon C, Akdemir H (1989) Multiple primary hydatid cysts of the brain. Turk J Pediatr 31(1): 57-61.
-
Sharma A, Abraham J (1982) Multiple giant hydatid cysts of the brain.Case report. J Neurosurg 57(3): 413-415.
-
Osborn AG, Preece MT (2006) Intracranial cysts: radiologic- pathologic correlation and imaging approach. Radiology 239: 650-664.
-
Oprisan A, Popescu BO (2013) intracranial cysts: an imagery diagnostic challenge. Sci World J 172154.
-
Huseyin Per, Sefer Komendas, Gu¨mu¨s H, Ali Kurtsoy (2009) Primary solitary and multiple intracranial cyst hydatid disease: Report of five cases. Brain & Development 31 (3): 228- 233.
-
Ciurea AV, Vasilescu G, Nuteanu L, Carp N(1995) Cerebral hydatid cyst in children. Experience of 27 cases. Child’s Nerv Syst 11(12): 679–685.
-
Mingde Q, Zheshang H (1981)Echinococcosis of the central nervous system. Eur Neurol 20(2): 125–131.
-
Ciurea AV, Fountas KN, Coman TC, Machinis TG, Kapsalaki EZ, et al. (2006) Long-term surgical outcome in patients with intracranial hydatid cyst. Acta Neurochir (Wien) 148(4): 421–426.
-
Lunardi P, Missori P, Di-Lorenzo N (1991) Cerebral hydatidosis in childhood: a retrospective survey with emphasis on long-term follow-up. Neurosurgery 29(4): 515-518.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review