Testis Sparing Surgery in Double Testicular Tumor in a Child Report of a Case
Mature teratomas are the most common benign testicular tumour during childhood. Epidermoid cyst are rare benign tumours, being more frequent before adolescence. We report so far the only case of ipsilateral and synchronous mature teratoma and epidermoid cyst in paediatric age.
Case Report
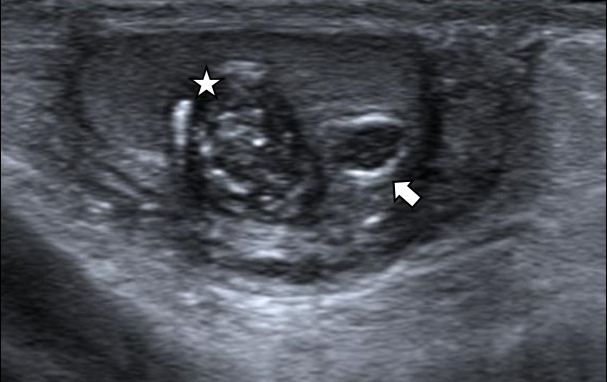
An 11-year-old boy presented with acute left testicular pain of 12 hours, without sweating or vomiting. A torsion of Morgagni hydatid was visualized on emergency ultrasound (US). This test also showed two incidental contiguous lesions in the lower pole of the left testis. They were hypo echoic with well-defined margins and without Colour-Doppler signal. The largest 8 x 6 mm with diffuse micro calcifications inside and the smallest 4 x 3 mm, with peripheral hyper echoic rim (Figure 1).
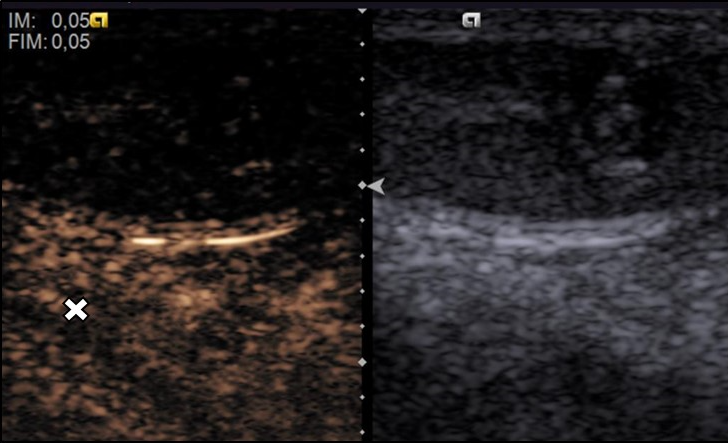
On physical examination we palpated two stony-hard nodules next to each other on distal third of left testis. No signs of pubertal development were found on the patient (Tanner I). Tumor markers of alpha fetoprotein, beta human chorionic gonadotropin and inhibin B were negative and serum levels of testosterone were normal. The contrast enhanced ultrasound (CEUS) confirmed absence of vascularization of the two nodules (Figure 2).
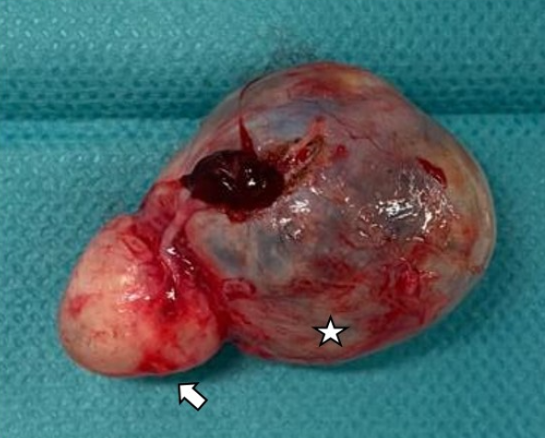
We proceeded to perform testis sparing surgery through scrotal access identifying two lesions next to each other. The biggest was heterogeneous purplish and the other yellowish. Both were encapsulated, non-infiltrating to testis parenchyma and easy to shell out. On histology, the major lesion was diagnosed of mature cystic teratoma. The minor was confirmed as epidermoid cyst (Figure 3).
On 3 years of follow up with routine ultrasound, no recurrence or testicular atrophy were detected.
Discussion
Testicular tumors are infrequent on pediatric age, being only about 1-2% of total solid tumors. Traditionally, they have been treated with radical orchiectomy through inguinal access, extrapolating the data of adults to children [1]. The frequency of benign tumors is highest in children than adults, even more in pre-pubertal. In post-pubertal children, the general incidence of testicular tumor increases ten times, being mostly malignant. Despite testis sparing surgery was described in the 80s, there is no big evidence for benign tumors in the last years. However, it is still controversial when you can apply this technique, because the risk of a final diagnosis of malignant tumor and recurrence [2]. Teratomas are the most frequent testicular tumors in children with an incidence between 8-48%. They are composed of tissues from the three germinal layers. On ultrasound, teratomas varies highly including focal or diffuse micro calcifications, cystic or solid, single or multi-septated. Some can mimic dermoid and Epidermoid cysts [3, 4]. Epidermoid cyst are tumors of keratin producing epithelium, being between 1-11% of total of pediatric testicular tumors. Sonographic findings include well circumscribed hypoechoic mass and hyper-echogenic rim with an onion-ring pattern [4, 5].
In both cases, there are no reports of their malignant variety in pre-pubertal patients [6]. The benign nature of these tumors favours testis sparing surgery [2, 6, 7, 8, 9, 10]. In adults, teratomas are malignant in 90-95% of cases. Avoiding unnecessary orchiectomy, prevents possible psychological problems and potential loss of fertility and hormonal function [6, 11]. Colour-Doppler ultrasound traditionally has been considered not sufficient to discard or confirm vascularization, and therefore malignancy. Ma W, et al. found avascular ultrasound lesions can be malignant in up to 39.7% of adult cases [12]. CEUS has already proved their efficacy to assess vascularization in intratesticular lesions. Two thirds of benign lesions showed no enhancement and one third had homogeneous enhancement. Heterogeneous enhancement was present in all malignant lesions [13, 14, 15].
Conclusion
In this case, all sonographic findings (both US and CEUS), pre-pubertal age and negative tumors markers were highly compatible with benign lesions. Consequently, access through inguinotomy to control spermatic vessels to deliver the testis and performing frozen section was not necessary, minimizing morbidity of surgery. So far, this is the only case reported of synchronous and ipsilateral mature teratoma and epidermoid cyst in pediatric age.
Availability of Data
The data of this case report are located at Consortium Corporation Sanitaria Parc Tauli, Sabadell, Spain.
Authors’ Contributions
GJR participated in data acquisition, drafting the manuscript and performed the surgery and follow-up of the patient. BJ, SMS, JJ, EC and AN participated in figure preparation, revising and editing and helped with translation for English language. JP assisted at the surgery. SB, SVB, GM and BN helped in revising and editing the manuscript. All authors read and approved the final manuscript.
References
-
Neumann DP, Abrams GS, Hight DW (1997) Testicular epidermoid cysts in prepubertal children: case report and review of the world literature. J Pediatr Surg 32(12): 1786-1789
-
Miao X, Li Y, Zhou T, Lv M (2021) Testis-sparing surgery in children with testicular tumors: A systematic review and meta-analysis. Asian J Surg 44(12): 1503-1509.
-
Epifanio M, Baldissera M, Esteban FG, Baldisserotto M (2014) Mature testicular teratoma in children: multifaceted tumors on ultrasound. Urology 83(1): 195- 197.
-
Maizlin ZV, Belenky A, Baniel J, Gottlieb P, Sandbank J, et al. (2005) Epidermoid cyst and teratoma of the testis: sonographic and histologic similarities. J Ultrasound Med 24(10): 1403-1409.
-
Eustace S, Graham D, Behan M, Smith JM (1994) Ultrasonographic diagnosis and surgical enucleation of an epidermoid cyst of the testis. Br J Urol 74(4): 518-519.
-
de Campos VAS, Chui CH, Cox S, Abdelhafeez AH, Fernandez PI, et al. (2022) International Society of Paediatric Surgical Oncology (IPSO) Surgical Practice Guidelines. Ecancermedicalscience 16: 1356.
-
Ross JH, Kay R, Elder J (1993) Testis sparing surgery for pediatric epidermoid cysts of the testis. J Urol 149(2): 353-356.
-
Rushton HG, Belman AB, Sesterhenn I, Patterson K, Mostofi FK (1990) Testicular sparing surgery for prepubertal teratoma of the testis: a clinical and pathological study. J Urol 144(3): 726-730.
-
O’Shea K, Tong A, Farrelly P, Craigie R, Cheesman E, et al. (2021) Management and outcome of paediatric testicular tumours - A 20 year experience. J Pediatr Surg 56(11): 2032-2036.
-
Ross JH, Rybicki L, Kay R (2002) Clinical behavior and a contemporary management algorithm for prepubertal testis tumors: a summary of the Prepubertal Testis Tumor Registry. J Urol 168(4 Pt 2): 1675-1678.
-
Skoogh J, Steineck G, Cavallin SE, Wilderang U, Hakansson UK, et al. (2011) Feelings of loss and uneasiness or shame after removal of a testicle by orchidectomy: a population- based long-term follow-up of testicular cancer survivors. Int J Androl 34(2): 183-192.
-
Ma W, Sarasohn D, Zheng J, Vargas HA, Bach A (2017) Causes of Avascular Hypoechoic Testicular Lesions Detected at Scrotal Ultrasound: Can They Be Considered Benign?. AJR Am J Roentgenol 209(1): 110-115.
-
Lung PFC, Fang C, Jaffer OS, Deganello A, Shah A, et al. (2020) Vascularity of Intra-Testicular Lesions: Inter- observer Variation in the Assessment of Non-neoplastic Versus Neoplastic Abnormalities After Vascular Enhancement with Contrast-Enhanced Ultrasound. Ultrasound Med Biol 46: 2956-2964.
-
Patel K, Sellars ME, Clarke JL, Sidhu PS (2012) Features of testicular epidermoid cysts on contrast-enhanced sonography and real-time tissue elastography. J Ultrasound Med 31(1): 115-122.
-
Isidori AM, Pozza C, Gianfrilli D, Giannetta E, Lemma A, et al. (2014) Differential diagnosis of nonpalpable testicular lesions: qualitative and quantitative contrast- enhanced US of benign and malignant testicular tumors. Radiology 273(2): 606-618.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review