Penetrating Injury Neck Sparing Major Vital Structures: A Case Report
Introduction: Penetrating neck injury accounts for only a small incidence of all trauma case. The neck is a compact structure with vascular, neural and aerodigestive tract compacted closely.Trauma to the aerodigestive tract, neural structures, vascular structures can present with increased mortality and morbidity Case Presentation: The authors here report a peculiar case of 24 years old male presenting with Penetrating neck injury by a wooden foreign body. The patient was managed surgically without any related complications. The Foreign Body was found to be missing all the vital structures in the neck after thorough confirmation by imaging modalities and later intra-operative findings. Discussion: Due to the close vicinity of these structures, injury to vital structures is a very real and potentially life threatening complication. Associated vascular, Aerodigestive and neural injuries results in an increase in fatality rate up to 50% in some cases and may be associated with an increased risk of medianitis. Furthermore, wooden foreign body carries an increased risk of infectious, difficulty of detection in different imaging modalities. Foreign body neck is known for secondary displacement during neck movements, hence confirming that an early treatment is strongly recommended. Conclusion: Due to high risk of injury to vital structures and mortality prompt detection and management of penetrating injury neck should a high priority.
Introduction
5–10% of all reported trauma cases are comprised of Penetrating injury to the neck. Timely and appropriate management of such cases is of utmost importance as the mortality rates associated can be as high as 10%. Trauma to the aero digestive tract, neural structures, vascular structures can present with increased mortality and morbidity [1]. The most common etiologies responsible for penetrating injury neck are violent physical attacks, motor vehicle accidents, or suicide attempts. Among this wooden foreign body possess in general a higher tendency to progress to infection due to the characteristic porosity of this organic material, allowing microorganisms to highly proliferate [2]. Here, we present a case of 24 year old male presenting to a tertiary centre with penetrating injury neck with a wooden foreign body and managed surgically.
Case Report
A case of 24 years old male presented to ED in a tertiary care centre with history of Road Traffic Accident approximately 6 hours back. Patient was initially taken to a nearby tertiary centre by early res ponders. On initial examination patient was vitally stable with a penetrating injury to the right side of neck with a wooden Foreign Body (FB) (Figure 1a-B).

Figure1: Foreign Body (Wooden) Injury to the Right Anterior Neck. A- At Presentation. B- Intraoperative.
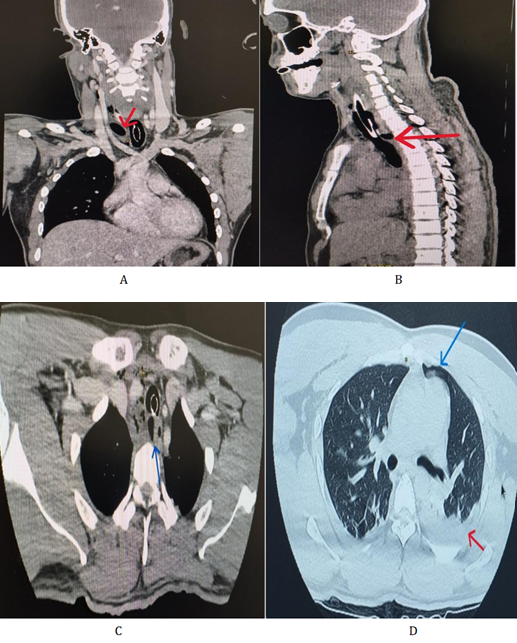
Figure 2: Cect Neck and Chest Showing A- Foreign Body (Red Arrow) Anterior To Right Common Carotid Artery. B- Fb (Red Arrow) Behind Trachea in Superior Mediastinum. C- Fb (Blue Arrow) Located In the Right Para-Oesophageal Region and Compressing Esophagus towards Left. D- Pneumomediastinum (Blue Arrow) With Feature of Hydro pneumothorax (Red Arrow) On the Left Side.
Ultrasonography (USG) Neck was done for evaluation which reported extent of wound approximately 2.5cm and showed no involvement of vital structures, but further imaging advised for confirmation. Patient was planned for exploration in the ENT department and intubated, however the procedure was deferred due to lack of Vascular and Thoracic Surgery back-up in the Centre. Patient was then referred to centre with Cardio-Thoracic Vascular Surgery (CTVS).
Patient presented to our centre intubated and emergency surgical intervetion planned by ENT department with intra- operative CTVS back-up. Pre-operative (Contrast Enhanced Computed Tomography) CECT Neck and chest was done which demonstrated hypo- dense FB approx 15mm*15cm in-situ right side neck anterior to right common carotid artery (Figure 2A), reaching up to D2 level behind trachea in superior mediastinum (Figure 2B) with the tip of the foreign body located in the right para-esophageal region and compressing esophagus towards left (Figure 2C), pneumomediastinum and hydropneumothorax on the left side (Figure 2D).
Surgery performed was exploration and extraction of the foreign body was performed and no evidence of involvement of vessels, aero-digestive tract or neural structures was found. Bilateral chest tube was placed and was removed on 3rd POD. Patient was later discharged and follow-up after 1 week was UN-eventful.
Discussion
Penetrating injury neck presents with multiple complications. While Penetrating neck injuries may present with a simple wounds, up to 80% of patients have been found with damage to major structures of the neck [3]. The most common among these, about 25% are those involving neck vessels with mortality rate of up to 50% [2]. 80 % of these are comprised of Carotid artery involvement and vertebral artery in 43 %. In addition, neurological structures including spinal cord, cranial nerves (VII–XII), sympathetic chain and brachial plexus are also at risk of damage [4]. Aero digestive injury accounting for 23– 30% of patients are also associated with risk of medianitis and a high mortality rate [1, 2]. Pharyngo - oesophageal injuries although more common, but are associated with a higher mortality rate of 20% than laryngotracheal injuries [1]. It is even rarer, however to sustain such an injury with no haemodynamic compromise and follow through with an uneventful clinical course [5].
Generally, wooden foreign bodies possess a greater diagnostic challenge as they are not easily detected by majority of imaging modalities like X-rays and CT Scans and require more advances techniques such as MRI for proper diagnosis and analysis of extent and position [6]. Wooden foreign body possesses in general a higher tendency to progress to infection due to the characteristic porosity of this organic material, allowing microorganisms to highly proliferate. In addition to these a high risk of a secondary displacement of the foreign body during neck movements may occur, hence confirming that an early treatment is strongly recommended [2].
Conclusion
Penetrating neck injury caused due to wooden foreign body has high complications and mortality rate and are refractory to most imaging modalities, thus timely management is of utmost importance. As neck is a compact structure with vital vascular, neural and aero digestive structures trauma to these structures are needed to be ruled out. Our case is a peculiar one as on preoperative imaging and surgical findings ruled out involvements of cny vital structures.
Conflicts of Interest: The authors declare no conflict of interest.
Funding: Self
References
-
Nowicki JL, Stew B, Ooi E (2017) Penetrating neck injuries: a guide to evaluation and management. Ann R Coll Surg Engl 100(1): 6-11.
-
Fama F, Cicciù M, Nastro-Siniscalchi E, Falzea R, Fodale V, et al. (2016) Nonfatal cervical-neck lesion with a wooden foreign body: diagnosis and management. J Craniofac Surg 27(1): 175-176.
-
Babi M, Tarter ZW, Shutt T, Cash E, Jorgensen J (2023) A Throwing Knife Injury to the Neck: Management of a Unique Airway Situation. Ear Nose Throat J 25: 01455613231186018.
-
Lodhia J, Chugulu S, Wampembe E, Chilonga K, Msuya D (2023) Traumatic left common carotid artery thrombosis with ischemic brain injury: A case report. Int J Surg Case Rep 111: 108891.
-
Menon SV, Ponen K, Williams AB (2023) aberrant anatomy angel–a near-miss penetrating neck trauma and a life-saving retropharyngeal right subclavian artery. BJR case reports 9(5): 20220104.
-
Imokawa H, Tazawa T, Sugiura N, Oyake D, Yosino K (2003) Penetrating neck injuries involving wooden foreign bodies: the role of MRI and the misinterpretation of CT images. Auris Nasus Larynx 30: 145-147.
- Management of Chronic Insertional Achilles Tendinopathy Using Flexor Hallucis Longus Tendon Transfer in Patients Over 50 Years of Age: A Four-Case Series Following the CARE Guidelines
- Application of Induced Pluripotent Stem Cells in Bone Tissue Engineering: Current Status and Prospects
- Surgical Management of Upper Thoracic Esophageal Squamous Cell Carcinoma with Concomitant Hypersplenism: Integration of Chai's Supra-Thoracic Apex Technique with Laparoscopic Splenectomy - A Technical Innovation Case Study with Systematic Review
- Evaluation of Masticatory Functional Efficiency of Stomatognathic System in Patients Undergoing Open Reduction Internal Fixation for Treatment of Pan-Facial Trauma: A Prospective Study
- Hepatic Abscess Secondary to Appendiceal Phlegmon an Unusual Complication of Appendiceal Phlegmon
- Report of Lumboperitoneal (LP) Shunt Procedure in Over Decades Experiences, Systematic Narrative Review