The Chrysalis Graft: Combination of Diced-Cartilage-Fascia Grafts and PRP in Augmentation Rhinoplasty
Introduction: This dorsal nasal augmentation technique utilizes a combination of the diced-cartilage with Platelet-Rich-Plasma (PRP), Platelet-Poor-Plasma (PPP) and fascia graft in a chrysalis form, which provides a regenerative and moldable technique. Methods: Patients requiring dorsal augmentation underwent rhinoplasty using diced-cartilagein a PRP-clot carrier,wrapped in a sleeve of deep-temporal fascia in achrysalis form. The PRP fraction was extracted after blood centrifugation and used to carry the diced-cartilage graft. The PPP and middle platelet layers were used as fibringlue sprayed over the chrysalis graft avoiding the use of stitches. Results: A total of 31 patients, with a mean age of 42 years old underwent augmentation rhinoplasty with this technique. The mean follow-up was 14 months. Donor sites for cartilage included nasal septum (n=13), concha (n=6), combination of both septum and concha (n=5) and rib (n=7). The surgical approach was open rhinoplasty in 20 cases and closed approach in 11 patients. No major complications requiring surgical revision were observed. No extrusions, no graft displacement and no skin irregularities were observed. Three cases (9.67%) of partial graft resorption were observed. Other complications included one case of local infection and two keloids in ear donor site. Satisfactory nasal dorsal augmentation was achieved in all other cases. Conclusions: This report describes a technique of dorsal augmentation using a mixture of diced-cartilage grafts, PRP, PPP and deep temporal fascia graft in a chrysalis manner. This approach offers a moldable and regenerative construct for nasal augmentation without major complications and minimal graft resorption.
Introduction
We present a modified technique for autologous dorsal nasal augmentation rhinoplasty using diced cartilage and fascia that also incorporates a PRP autologous carrier. This technique is a modification of Daniel and Calvert’s technique [1] that uses diced cartilage and fascia grafts. Diced cartilage in dorsal nasal augmentation was first popularized by Erol [2] in a large series using the named “Turkish delight” technique. Erol’s technique consisted in a combination of diced autologous cartilage wrapped in oxidized regenerated cellulose (Surgicel; Ethicon Inc). Despite very good results demonstrated by Erol some have criticized the technique as not being easily reproducible, and noting higher rates of cartilage resorption using similar techniques [1, 3]. Also, Surgicel has been associated with chronic inflammation and animal studies have shown a lack of proliferation of cartilage grafts wrapped in Surgicel [4]. Another variation of technique was described by Bullocks [5], using diced cartilage in an autologous scaffold created from Platelet- Rich Plasma (PRP) and Platelet-Poor Plasma (PPP). PRP contains growth factors and PPP acts as fibrin glue. In our own clinical experience this technique carries various potential limitations, including visible and palpable skin irregularities along the surface of diced cartilage, limited extend of overall dorsal augmentation, and cartilage graft displacement. To overcome these limitations we have preferred techniques with the combination of diced cartilage and deep temporal fascia grafts, such as first described by Daniel and Calvert [1]. While we have had overall clinical success using Daniel and Calvert techniques, we also have noted graft resorption, which may be due to fascia grafts impeding imbibition of cartilage grafts. In an attempt to minimize the occurrence of graft resorption and skin irregularities, while still achieving good nasal augmentation, we have employed the following technique which combines diced cartilage- fascia grafts with PRP.
Patients and Methods
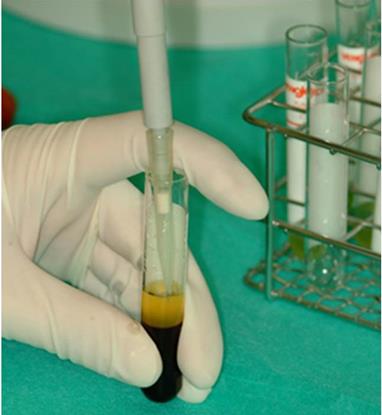
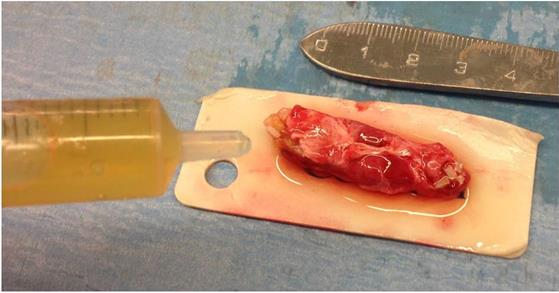
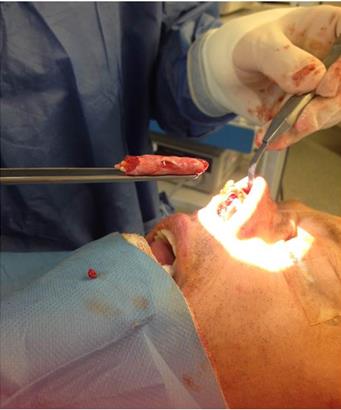
Patients undergoing augmentation rhinoplasty between April 2012 and January 2016 were treated with diced cartilage in a PRP clot carrier, wrapped in a sleeve of deep temporal fascia (Figures 1-4). Diced cartilage was cleanly cut and not crushed. Cartilage donor sites were septum, concha and chondro-costal union. Cartilage was diced into 0.5-1 mm fragments. A rectangular fascia graft (approximately 2x4 cm) was harvested from deep temporal fascia. PRP was obtained by blood centrifugation 1800 rpm 8 minutes. Twenty cc of peripheral blood were extracted in the preoperative area using 4.5 cc sterile vacuum tubes containing 3.8% sodium citrate as an anticoagulant. The anticoagulant effect of sodium citrate and centrifugation at low intensity protect platelet membrane integrity during the process. After centrifugation, three layers were observed in the tube, the lower red layer containing red cells, the middle thin layer containing white cells, and the upper yellow layer containing platelets. The upper layer containing platelets can also be separated in three layers: the upper layer is the layer that contains less platelet growth factors, its content is practically only plasma and is called Platelet- Poor Plasma (PPP); the middle layer presents a very similar platelet proportion of peripheral blood; and the lower layer located immediately above the white series is the fraction corresponding to the major platelet concentration, it is called Platelet-Rich Plasma (PRP) and this is the fraction that interests us and represents approximately 10% of the total volume of blood taken (Figure 5). The upper (PPP) and middle platelet layers were extracted with sterile pipette to be used later as fibrin glue. The PRP fraction was extracted by manual pipetting and is the one used to carry the diced cartilage graft (Figure 6). The PRP fraction was activated with 0.05 cc of 10% calcium chloride for each 0.5 cc of PRP. PRP activation allowed platelets to release growth factors contained in the alpha granules (Figure 7). Diced cartilage and activated PRP were placed over the fascia graft supported over the silicone mold for nasal augmentation. After 7-8 minutes, the activated PRP changed from liquid to a gelatinous consistency, as a clot. This clot contained the diced cartilage grafts. The fascia graft was wrapped around the clot like a chrysalis or Italian cannelloni (Figure 8). Once the cannelloni is rolled, the PPP was sprayed over it to act as fibrin glue (Figure 9). No stitches were needed to close the fascia graft. The pocket dissection was limited to the graft size, to prevent graft displacement. The graft is then inserted into the nasal dorsum (Figures 10 & 11). Manual manipulation allowed adjustments in the graft position and form. Steri-strip and a nasal splint were placed over the nasal dorsum for 7 days. A clinical revision was made on the fourth day after surgery, removing the splint to verify that the graft has not moved and for manual modeling if necessary and the splint was then repositioned until the 7th day. Antibiotic prophylaxis was given for 5 days.

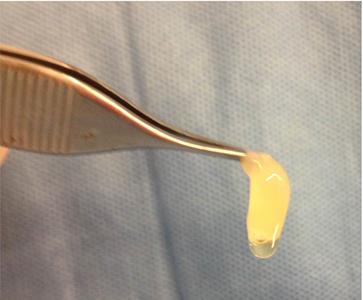

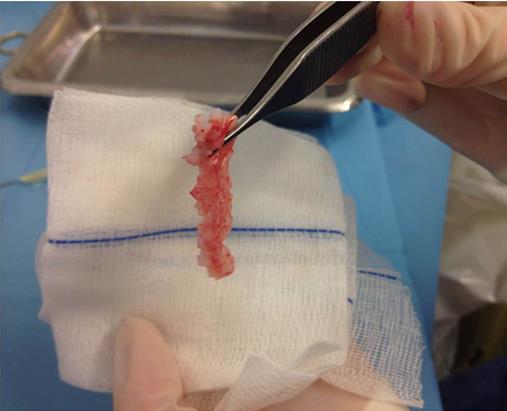
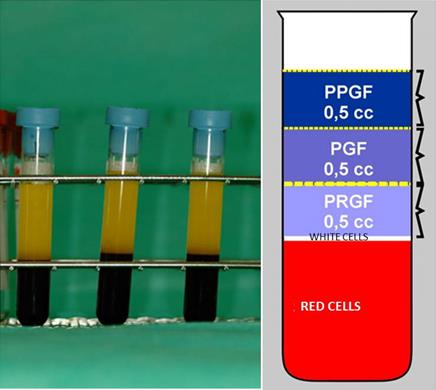
Figure 5: The blood tube after centrifugation shows 3 layers: the lower red layer containing red cells, the middle thin layer containing white cells, and the upper yellow layer containing platelets. The upper layer containing platelets can also be separated in 3 layers: the upper layer is the layer that contains less platelet growth factors and is called Plasma Poor in Growth Factors or Platelet-Poor Plasma (PPGF or PPP); the middle layer presents a very similar platelet proportion of peripheral blood (Plasma with Growth Factors, PGF); and the lower layer located immediately above the white series is the fraction corresponding to the major platelet concentration, it is called Plasma Rich in Growth factors or Platelet-Rich Plasma (PRGF or PRP).




Results
Thirty-one patients (21 women and 10 men) with a mean age of 42 years old (range 24-61) underwent augmentation rhinoplasty with the described technique combining diced cartilage grafts, PRP and deep temporal fascia in a chrysalis manner. The mean follow-up was 14 months (range: 7-25). Donor sites were nasal septum (n=13), concha (n=6), combination of septum and concha (n=5) and chondro-costal union (n=7). The surgical approach was open rhinoplasty in 20 cases and close rhinoplasty in 11 patients.
The results were documented clinically by inspection and palpation, as well as photographically. Patients satisfaction was also assessed. No major complications requiring surgical revision were observed. No extrusions, no graft displacement and no skin irregularities were observed. Three cases (9.67%) of partial graft resorption were observed in ex-cocaine users; however, no additional surgery was performed because the patients refused surgery. One case of local infection presented as a cellulite was resolved with oral antibiotic. Two keloids in ear donor site were observed in African patients and resolved with triamcinolone injections. Good nasal dorsal augmentation was achieved in all other cases (Figures 12- 15, Table 1).



| Patient | A | g | e | Sex | Unaesthetisms cause | Donor site | Graft resorption | Complications | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 43 | Female | Secondary rhinoplasty | Concha | No | No | ||||||||||||||
| 2 | 24 | Female | Congenital | Septum | No | No | ||||||||||||||
| 3 | 36 | Female | Congenital | Septum | No | No | ||||||||||||||
| 4 | 61 | Male | Congenital | Septum, concha | No | No | ||||||||||||||
| 5 | 38 | Female | Ethnic nose | Septum, concha | No | Ear keloid | ||||||||||||||
| 6 | 44 | Female | Congenital | Septum | No | No | ||||||||||||||
| 7 | 26 | Female | Secondary rhinoplasty | Concha | No | No | ||||||||||||||
| 8 | 35 | Female | Ethnic nose | Septum | No | No | ||||||||||||||
| 9 | 51 | Female | Secondary rhinoplasty | Concha | No | No | ||||||||||||||
| 10 | 37 | Female | Secondary rhinoplasty | Concha | No | No | ||||||||||||||
| 11 | 47 | Female | Secondary rhinoplasty | Concha | No | No | ||||||||||||||
| 12 | 45 | Male | Post-traumatic | Chondrocostal | No | Local infection | ||||||||||||||
| 13 | 39 | Female | Secondary rhinoplasty | Septum | No | No | ||||||||||||||
| 14 | 36 | Female | Secondary rhinoplasty | Septum | No | No | ||||||||||||||
| 15 | 59 | Female | Ethnic nose | Septum, concha | No | Ear keloid | ||||||||||||||
| 16 | 38 | Female | Ethnic nose | Septum, concha | No | No | ||||||||||||||
| 17 | 42 | Female | Congenital | Septum | No | No | ||||||||||||||
| 18 | 27 | Male | Post-traumatic | Chondrocostal | No | No | ||||||||||||||
| 19 | 45 | Male | Cocaine | Chondrocostal | Yes | No | ||||||||||||||
| 20 | 53 | Female | Secondary rhinoplasty | Concha | No | No | ||||||||||||||
| 21 | 49 | Female | Congenital | Septum | No | No | ||||||||||||||
| 22 | 52 | Female | Cocaine | Chondrocostal | Yes | No | ||||||||||||||
| 23 | 33 | Male | Secondary rhinoplasty | Chondrocostal | No | No | ||||||||||||||
| 24 | 38 | Male | Secondary rhinoplasty | Septum | No | No | ||||||||||||||
| 25 | 57 | Male | Post-traumatic | Chondrocostal | No | No | ||||||||||||||
| 26 | 36 | Female | Post-traumatic | Septum | No | No | ||||||||||||||
| 27 | 42 | Female | Ethnic nose | Septum | No | No | ||||||||||||||
| 28 | 53 | Female | Congenital | Septum | No | No | ||||||||||||||
| 29 | 36 | Male | Ethnic nose | Septum, concha | No | No | ||||||||||||||
| 30 | 41 | Male | Cocaine | Chondrocostal | Yes | No | ||||||||||||||
| 31 | 43 | Male | Congenital | Septum | No | No |
Table 1: The table shows distribution of the 31 cases.
Discussion
The advantages of diced cartilage in augmentation rhinoplasty are that they have no visible edges, do not carry risk of warping, can be easily molded to resurface irregularities, and it allows the use of all the cartilage fragments that are usually discarded. Moreover, diced cartilage grafts revascularize faster due to the increased surface area available. Solid costal cartilage grafts have been used extensively for nasal augmentation, but the disadvantages are resorption, stiffness, graft visibility, donor site pain, suboptimal shape and warping.
The advantages of wrapping the diced cartilages in a fascia graft sleeve are that the fascia helps to camouflage skin irregularities, provides a high tensile strength and it is a durable graft material with cell-supportive properties acting like a scaffold for tissue integration [6, 7, 8, 9, 10]. Brenner [11] histologically compared isolated cartilage grafts with dice cartilage grafts wrapped in Surgicel and deep temporal fascia in rats, observing that the cartilages wrapped in Surgicel contained the minimum cartilage cells, whereas those wrapped in fascia showed higher viability. Cerkes [12] described an interesting technique for nasal dorsum augmentation using rectus abdominis fascia in secondary cases requiring costal cartilage grafts, with the advantage of single donor site area. However, the fascia grafts integrates well into tissues but could impede imbibition of cartilage grafts, leading to a cartilage grafts resorption. For that reason, the use of PRP as a regenerative component was included in this technique. Wrapping diced cartilage in hyaluronic acid was also found to improve cartilage survival compared with oxidized regenerated cellulose [13], but hyaluronic acid increases costs. Kim compared histologically the viability of diced cartilage wrapped in autogenous fascia to diced cartilage wrapped in AlloDerm® in a rabbit model, reporting superior results with AlloDerm [14]. One significant disadvantage of AlloDerm is that the increased cost of the procedure.
Platelet-rich plasma (PRP) is defined as a portion of the plasma itself with a platelet concentration above the baseline obtained by centrifugation. The plasma fraction contains not only a greater volume of platelets but platelet factors, which exert multiple actions on different aspects of tissue repair. Platelet Derived Growth Factors (PDGFs) are bioactive proteins contained in the alpha granules of platelets that stimulate cellular proliferation and differentiation to promote reparative and regenerative tissue phenomena. Each platelet contains 50 to 80 alpha granules which are formed during megakaryocyte maturation. PDGFs include transforming growth factor beta (TGF β), platelet factor 4 (PF4), interleukin 1 (IL-1), platelet derived angiogenic factor (PDAF), vascular endothelial growth factor (VEGF), epidermal growth factor (EGF), platelet derived endothelial growth factor (PDEGF), epithelial cell growth factor (ECGF), insulin-like growth factor (IGF), osteocalcin, osteonectin, fibrinogen, fibronectin and thrombospondin. These factors are released from the alpha granules in response to platelet activation by platelet aggregation inducers. Platelets start to secrete actively these substances 10 minutes after thrombus formation, releasing more than 95% of the presynthesized growth factors within 1 hour. After this massive protein release, platelets synthesize and secrete proteins additionally for 5 to 10 days. When the influence of platelets begins to subside, the macrophages that have reached the focus thanks to the vascular growth promoted by platelets regulate tissue repair by secreting their own factors. Proteins secreted by platelets exert multiple actions on different aspects of tissue repair. PDGF are chemotactic for macrophages, they exert a chemotactic and mitogenic action on progenitor cells and osteoblasts as well as an angiogenic effect, induce the formation of bone matrix and collagen and contribute in bone mineralization. PRP enhances cartilage repair and stimulates chondrocyte proliferation and the production of cartilage matrix by chondrocytes [15, 16, 17]. Some of the proteins released by platelets are absent in chronic wounds that do not heal properly, which provides further evidence of the role of these substances in tissue repair. PRP contains approximately a concentration of PDGF eight times higher than the basal plasma.
There are numerous growth factors in PRP that stimulate cartilage matrix synthesis and mitigate the effects of catabolic cytokines such as interleukin IL-1 and tumor necrosis factor-α (TNF-α). When tested in combination, growth factors have synergistic effects on cartilage matrix synthesis [18, 19] and they are known to induce further growth factor protein production by neighboring articular chondrocytes [20]. Platelets also store proteins with antibacterial and fungicidal properties, coagulation factors, and membrane glycoproteins that influence inflammation by increasing the synthesis of interleukins and chemokines. PRP has an anti- inflammatory effect via down regulation of known catabolic signaling pathways [21, 22, 23]. All such actions have clinical effects that generally can be summarized in: increase in soft tissue and bone repair processes, and decreased rates of postoperative infection, inflammation, pain and blood loss [24, 25].
The PRP is currently used to improve the integration of bone grafts at the maxillar bone and the obliteration of bone cysts, as well as in orthopaedic surgery to accelerate healing of bone fractures and cartilage-muscle-tendon injuries [26, 27]. It is also used in other fields of surgery to improve the integration of the grafts in the host tissue [21, 28, 29, 30, 31, 32]. The regenerative properties of the PRP added to the diced cartilage allow better integration of the grafts and reduce graft resorption. Güler [33] compared histologically the viability of chondrocytes, the content of collagen fiber in matrix and the peripheral tissue changes in four comparison groups of rabbits (bare diced cartilage/ diced cartilage wrapped in AlloDerm/ diced cartilage wrapped in Surgicel/ diced cartilage wrapped in platelet-rich fibrin matrix). Güler concluded that the viability of chondrocytes, the content of fiber in matrix and the peripheral tissue changes were higher in the cartilage embedded in the platelet-rich fibrin matrix group. Göral [34] demonstrated that platelet-rich fibrin improves the viability of diced cartilage grafts in a rabbit model. Manafi [35] showed that PRP was effective in increasing survival and regeneration capacity of cartilage grafts in rabbit model. Mishra [36] in an in vitro investigation reported that PRP enhanced chondrogenic differentiation. Saito [37] showed that administration of gelatin hydrogel micro-spheres containing PRP has preventive effects against osteoarthritis degeneration in a rabbit model. Tasman [38, 39, 40] described a technique for nasal augmentation using a diced cartilage glue graft with Tisseel (Baxter International Inc.) and without fascia. The
manufacturer of Tisseel cautions that the fibrin sealant may induce hypersensitivity or allergic reactions and carries a risk of transmitting infectious agents because it is derived from pooled human plasma. PRP has advantages over the use of commercial tissue glue. The use of PRP and PPP, in addition to having a biological glue effect, has a regenerative effect and lower cost. Commercial fibrin glues stabilize diced cartilage grafts but do not enclose them. PRP is an autologous material that offers both stabilization and enclosure of diced cartilage without the risks of hypersensitivity or disease transmission.
In most cases no resorption of cartilage was observed, and the shape and integrity of the nasal dorsum were maintained. The percentage of patients who suffered partial resorption of the graft (9.67%) was lower compared to our resorption rates using other techniques without PRP (up to 30%).
Not only are the platelet-derived growth factors useful in improving the survival of cartilage grafts. The work of Orbay [41] suggested that adipose-derived stem cells (ADSC) can maintain the viability of diced cartilage. ADSC are autologous and easy to harvest, so they may be useful for improving the long-term outcomes of diced cartilage grafting. However, obtaining PRP is simpler than obtaining ADSC.
The PPP acts as natural fibrin glue. Cyanoacrylate glue has been used as an alternative to sutures for the fixation of rib cartilage slices in a porcine model but was found to induce a strong foreign body reaction, resulting in partial resorption of the graft [42].
Augmentation rhinoplasty with autologous tissue is preferable to the use of synthetic materials, which can give complications in the medium and long-term such as extrusion, migration, foreign body reactions or chronic recurrent infections.
Although studies with longer series and follow-up are needed, this technique can be considered a good surgical option.
Conclusions
This technique combining diced cartilage grafts, PRP, PPP and deep temporal fascia graft in a chrysalis manner allows correct dorsal nasal augmentation with no major complications and minimal graft resorption due to the regenerative properties of the PRP.
Meetings at which the work was presented: - ASAPS Las Vegas Aesthetic Symposium, USA, 2016.
Facial & Rhinoplasty Symposium. - Rhinoplasty Society Meeting. Las Vegas (USA), 2016. - Congress of the Spanish Society of Fat Grafting (SETGRA), Barcelona (Spain), 2016. - IMCAS World Congress, Paris (France), 2018. Video rhinoplasty session. - Congress of the Catalonian Society of Plastic Surgery.
Terrassa, Barcelona (Spain), 2018.
References
-
Daniel RK, Calvert JW (2004) Diced cartilage grafts in rhinoplasty surgery. Plast Reconstr Surg 113(7): 2156-2171.
-
Erol O (2000) The Turkish delight: a pliable graft for rhinoplasty. Plast Reconstr Surg 105(6): 2229-2241.
-
Kelly MH, Bulstrode NW, Waterhouse N (2007) Versatility of diced cartilage-fascia grafts in dorsal nasal augmentation. Plast Reconstr Surg 120(6): 1654-1659.
-
Yilmaz S, Erçöçen AR, Can Z, Yenidünya S, Edali N, et al. (2001) Viability of diced, crushed cartilage grafts and the effects of Surgicel (oxidized regenerated cellulose) on cartilage grafts. Plast Reconstr Surg 108(4): 1054-1060.
-
Bullocks JM, Echo A, Guerra G, Stal S, Yuksel E (2011) A novel autologous scaffold for diced-cartilage grafts in dorsal augmentation rhinoplasty. Aesthetic Plast Surg 35(4): 569-579.
-
Dubay D, Wang X, Kirk S, Adamson B, Robson MC, et al. (2004) Fascial fibroblast kinetic activity is increased during abdominal wall repair compared to dermal fibroblasts. Wound Repair Regen 12(5): 539- 545.
-
Calvert JW, Brenner K, DaCosta-Iyer M, Evans GR, Daniel RK (2006) Histological analysis of human diced cartilage grafts. Plast Reconstr Surg 118(1): 230-236.
-
Guerrerosantos J, Trananino C, Guerrerosantos F (2006) Multifragmented cartilage wrapped with fascia in augmentation rhinoplasty. Plast Reconstr Surg 117(3): 804-812.
-
Daniel RK (2008) Diced cartilage grafts in rhinoplasty surgery: current techniques and applications. Plast Reconstr Surg 122(6): 1883-1891.
-
Harel M, Margulis A (2013) Dorsal augmentation with diced cartilage enclosed with temporal fascia in secondary endonasal rhinoplasty. Aesthet Surg J 33(6): 809-816.
-
Brenner KA, McConnell MP, Evans GR, Calvert JW (2006) Survival of diced cartilage grafts: an experimental study. Plast Reconstr Surg 117(1): 105- 115.
-
Cerkes N, Basaran K (2016) Diced Cartilage Grafts Wrapped in Rectus Abdominis Fascia for Nasal Dorsum Augmentation. Plast Reconstr Surg 137(1): 43-51.
-
Kazikdas KC, Ergur B, Tugyan K, Guneli E, Kaya D, et al. (2007) Viability of crushed and diced cartilage grafts wrapped in oxidized regenerated cellulose and esterified hyaluronic acid: an experimental study. Laryngoscope 117(10): 1728-1734.
-
Kim HK, Chu LS, Kim JW, Park B, Kim MK, et al. (2011) The viability of diced cartilage grafts wrapped in autogenous fascia and AlloDerm (in a rabbit model). J Plast Reconstr Aesthet Surg 64(8): e193-e200.
-
Akeda K, An HS, Okuma M, Attawia M, Miyamoto K, et al. (2006) Platelet-rich plasma stimulates porcine articular chondrocyte proliferation and matrix biosynthesis. Osteoarthritis Cartilage 14(12): 1272- 1280.
-
Park SI, Lee HR, Kim S, Ahn MW, Do SH (2012) Time- sequential modulation in expression of growth factors from platelet-rich plasma (PRP) on the chondrocyte cultures. Mol Cell Biochem 361(1-2): 9- 17.
-
Gaissmaier C, Fritz J, Krackhardt T, Flesch I, Aicher WK, et al. (2005) Effect of human platelet supernatant on proliferation and matrix synthesis of human articular chondrocytes in monolayer and three- dimensional alginate cultures. Biomaterials 26(14): 1953-1960.
-
Chubinskaya S, Hakimiyan A, Pacione C, Yanke A, Rappoport L, et al. (2007) Synergistic effect of IGF-1 and OP-1 on matrix formation by normal and OA chondrocytes cultured in alginate beads. Osteoarthritis Cartilage 15(4): 421-430.
-
Longobardi L, O’Rear L, Aakula S, Johnstone B, Shimer K, et al. (2006) Effect of IGF-I in the chondrogenesis of bone marrow mesenchymal stem cells in the presence or absence of TGF-beta signaling. J Bone Miner Res 21(4): 626-636.
-
Shi S, Mercer S, Eckert GJ, Trippel SB (2009) Growth factor regulation of growth factors in articular chondrocytes. J Biol Chem 284(11): 6697-6704.
-
Fortier LA, Hackett CH, Cole BJ (2011) The Effects of Platelet-Rich Plasma on Cartilage: Basic Science and Clinical Application. Oper Tech Sports Med 19(3): 154-159.
-
Van Buul GM, Koevoet WL, Kops N, Bos PK, Verhaar JA, et al. (2011) Platelet-rich plasma releasate inhibits inflammatory processes in osteoarthritic chondrocytes. Am J Sports Med 39(11): 2362-2370.
-
Bendinelli P, Matteucci E, Dogliotti G, Corsi MM, Banfi G, et al. (2010) Molecular basis of anti-inflammatory action of platelet-rich plasma on human chondrocytes: mechanisms of NF-(B inhibition via HGF. J Cell Physiol 225(3): 757-766.
-
Eppley BL, Woodell JE, Higgins J (2004) Platelet quantification and growth factor analysis from platelet-rich plasma: implications for wound healing. Plast Reconstr Surg 114(6): 1502-1508.
-
Eppley BL, Pietrzak WS, Blanton M (2006) Platelet- rich plasma: a review of biology and applications in plastic surgery. Plast Reconstr Surg 118(6): 147e- 159e.
-
Kon E, Buda R, Filardo G, Di Martino A, Timoncini A, et al. (2010) Platelet-rich plasma: intra articular knee injections produced favorable results on degenerative cartilage lesions. Knee Surg Sports Traumatol Arthrosc 18(4): 472-479.
-
Lee HR, Park KM, Joung YK, Park KD, Do SH (2012) Platelet-rich plasma loaded hydrogel scaffold enhances chondrogenic differentiation and maturation with up-regulation of CB1 and CB2. J Control Release 159(3): 332-337.
-
Marx RE (2004) Platelet-rich plasma: evidence to support its use. J Oral Maxillofac Surg 62(4): 489-496.
-
Marx RE, Carlson ER, Eichstaedt RM, Schimmele SR, Strauss JE, et al. (1998) Platelet-rich plasma: Growth factor enhancement for bone grafts. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 85(6): 638-646.
-
Anitua E (1999) Plasma rich in growth factors: preliminary results of use in the preparation of future sites for implants. Int J Oral Maxillofac Implants 14(4): 529-535.
-
Hee HT, Majd ME, Holt RT, Myers L (2003) Do autologous growth factors enhance transforaminal lumbar interbody fusion? Eur Spine J 12(4): 400-407.
-
Cerza F, Carni S, Carcangiu A, Di Vavo I, Schiavilla V, et al. (2012) Comparison between hyaluronic acid and platelet-rich plasma, intra-articular infiltration in the treatment of gonarthrosis. Am J Sports Med 40(12): 2822-2827.
-
Güler I, Billur D, Aydin S, Kocatürk S (2015) Efficacy of platelet-rich fibrin matrix on viability of diced cartilage grafts in a rabbit model. Laryngoscope 125(3): E104-11.
-
Göral A, Aslan C, Bolat Küçükzeybek B, Işık D, Hoşnuter M, et al. (2016) Platelet-Rich Fibrin Improves the Viability of Diced Cartilage Grafts in a Rabbit Model. Aesthet Surg J 36(4): NP153-62.
-
Manafi A, Kaviani Far K, Moradi M, Amir Manafi, Farzad Manafi (2012) Effects of platelet-rich plasma on cartilage grafts in rabbits as an animal model. World J Plast Surg 1(2): 91-98.
-
Mishra A, Tummala P, King A, Lee B, Kraus M, et al. (2009) Buffered platelet-rich plasma enhances mesenchymal stem cell proliferation and chondrogenic differentiation. Tissue Eng Part C Methods 15(3): 431-435.
-
Saito M, Takahashi KA, Arai Y, Inoue A, Sakao K, et al. (2009) Intraarticular administration of platelet-rich plasma with biodegradable gelatin hydrogel microspheres prevents osteoarthritis progression in the rabbit knee. Clin Exp Rheumatol 27(2): 201-207.
-
Tasman AJ, Diener PA, Litschel R (2013) The diced cartilage glue graft for nasal augmentation. Morphometric evidence of longevity. JAMA Facial Plast Surg 15(2): 86-94.
-
Baker SR (2012) Diced cartilage augmentation: early experience with the Tasman technique. Arch Facial Plast Surg 14(6): 451-455.
-
Tasman AJ (2013) Advances in nasal dorsal augmentation with diced cartilage. Curr Opin Otolaryngol Head Neck Surg 21(4): 365-371.
-
Orbay H, Tobita M, Hyakusoku H, Mizuno H (2012) Effects of adipose-derived stem cells on improving the viability of diced cartilage grafts. Plast Reconstr Surg 129(2): 369-377.
-
Lopez MA, Shah AR, Westine JG, O'Grady K, Toriumi DM (2007) Analysis of the physical properties of costal cartilage in a porcine model. Arch Facial Plast Surg 9(1): 35-39.
- Reconstruction of Nasal Defect Using a Local Flap Based in the Nanoperforants Concept: A Case Report
- Transplant Tourism in Japan: Insights from Nationwide Surveys and Emerging Ethical Challenges
- The Challenge of Peritoneal Vaginoplasty in Transgender Women: Review Literature and Personal Perspectives
- Algorithmic Paternalism: Autonomy Versus Automation
- Dermatoscopy in Gorlin Syndrome: Avoiding the Disfigurement in Patients
- How Artificial Intelligence is Ushering in a New Era of Innovation in General and Plastic Surgery: A Short Communication