Surgical Treatment Options for Augmentation Post-Mastoplasty Breast Ptosis with Silicone Implants
Introduction: Breast ptosis is the descent of the nipple areola complex below its normal position. It can be primary or secondary to the use of implants and the treatment is always surgical. In secondary ptosis, surgical treatment consists of removing excess skin, elevation of the nipple areola complex, fixation of the gland while preserving its function, sensitivity and symmetry, manipulation of implants, capsule and placement plane. Objective: To demonstrate the main deformities that appear in breast ptosis after augmentation mastoplasty with silicone implants and the surgical treatment options for each of them. Method: A descriptive, longitudinal and prospective study was carried out, which included 36 patients who underwent surgery for augmentation mastoplasty with silicone implants who attended the breast surgery department of the Plastic Surgery service of the “Hermanos Ameijeiras†Hospital with breast ptosis, in the Period from October 2016 to March 2019. Results: The age group between 33 and 46 years prevailed 61%. Tissue atrophy 56% was the most frequent cause. Pseudoptosis prevailed 75%. Pexy with an undefined pedicle, periareolar closure and implant change was the most used technique in 44%. The least used technique was inverted T 8% and all of them it was associated with previous scars. The aesthetic result was good in 100% of the cases. Conclusions: Breast ptosis after augmentation mastoplasty with silicone cohesive gel implants has a multifactorial origin, so treatment must be personalized for each patient and more specifically for each breast.
Introduction
The breast is an anatomical region with physical and Conceptual Paper
psychic functions such as breastfeeding, the expression of femininity, beauty and eroticism. It is an important part of female morphology and its development constitutes one of the most important characteristics of sexual difference. Over the years the ideal icons of beauty change and transform, and with them the currents and fashions [1, 2].
The search for trunk harmony is a factor that has contributed to millions of women wearing breast implants and others undergoing reduction mastoplasty. Choosing a surgical procedure that meets the current basic conditions of an “optimal” mastoplasty is difficult due to the innumerable publications of original techniques and their modifications. The condition of a satisfactory result is not only that the technique meets the necessary basic criteria and that the surgeon “feels comfortable in its execution”, but also careful post-operative care. Cosmetic surgery is “artisan work, science and art” [1].
Techniques for breast augmentation began in the 20th century and developed with the evolution of augmentation materials including: autologous transposition of fatty grafts (1895 - 1950), injection of liquid silicone (1950), special sponges (1958), dextran (1965) and saline (1971). Currently silicone gel implants are used worldwide in cosmetic augmentation mastoplasty [3].
Breast ptosis is a morphological condition of the breast characterized by a decrease in the areola-nipple complex (ANC) below its normal position. It occurs primarily or secondary to the use of implants. When ptosis is primary, treatment is aimed at removing excess skin, raising the ANC and fixing the gland with preservation of function, sensitivity, symmetry and lasting results. When ptosis is secondary to surgical treatment, the manipulation of the implants, the capsule and the placement plane are added.
Implant mastopexy was first described by Gonzales - Ulloa in 1960 and by Regnault in 1966, and since then it has been considered a complicated and controversial procedure, with increasing demand in plastic surgery every day. Various technical procedures are recommended to achieve additional stabilization of the gland, which can be classified as mastopexy with suture material, mastopexy with glandular or crossed dermoglandular flaps, stabilization with dermis flaps and pectoral stabilization with dermal strips, among others [4].
In the last 10 years, there has been an increase in women who have undergone augmentation mastoplasty with stents and patients who come to the clinic with late deformities. That is why the motivation of this research arises with the aim of demonstrating the main deformities that appear as an expression of breast ptosis after augmentation mastoplasty with cohesive silicone gel implants and to evaluate surgical treatment options according to the deformity and etiology.
Materials and Methods
A descriptive, longitudinal and prospective study was carried out, which included 36 patients with breast ptosis, who underwent augmentation mastoplasty with implants older than 6 months and less than 10 years in evolution, who consulted for breast dysmorphia at the Plastic Surgery service of the “Hermanos Ameijeiras” Surgical Hospital in the period from October 1st 2016 to March 31st, 2019.
Patients reconstructed for cancer and with decompensated chronic diseases were excluded.
First Consultation
They are classified according to the degree of breast ptosis, preoperative and pre-anesthetic checkup is indicated, general data, weight, height, body mass index, pathological history are recorded, physical examination evaluates the quality and quantity of breast tissue, breast volume, grade of ptosis, and preoperative anthropometric analyzes in relation to base, profile and breast projection. In order to determine the possible causes of implant augmentation post-mastoplasty breast ptosis, one cause per patient is selected, which is considered to have the greatest impact on its development [5, 6]. The wishes and expectations of each patient are determined. Different surgical options, benefits and possible complications of each reconstructive procedure are explained, their doubts are clarified and an informed consent is signed. A photographic record is made and hospital admission is indicated.
Preoperative Indications
The day before the surgical procedure, a free diet is indicated until 6:00 p.m. and liquid until 6 hours before surgery, antibiotic prophylaxis with cefazolin 3gr. (1 gr. pre, intra and postoperative) and diazepam 5mg, orally 21:00 hours.
Preoperative Planning Measurements
Planning is done with the patient sitting upright with hands on her thighs and looking straight ahead. The distances between the sternal fork and the ANC, the distance between the nipple and the nipple, the distance between the ANC and the submammary sulcus and ANC to the midline were measured.
Midline is marked from the sternal fork to the navel; The midclavicular line is marked from the clavicle to the submammary sulcus and the new pocket is marked, according to the diameter of the implant base and taking into account: the birth of the patient’s breast (regularly in the
2nd or 3rd rib), the parasternal line, anterior axillary line and submammary sulcus.
With the profile patient it was determined: • Segment 1: From the lower edge of the clavicle to the first breast crest.
• Segment 2: From the first breast crest to the edge of the mamelon.
• Segment 3: From the lower edge of the areola to the submammary sulcus.
• Segment 4: It is the submammary thoracic segment [5, 7].
On the woman seen in profile, 3 elements can be measured: a. Projection anterior to the breast, measured from the sternum to a tangent that passes through the most prominent part. In the normal breast it is equal to 1/3 of the diameter of the breast implantation base.
b. Submammary angle formed by a tangent that goes from the submammary sulcus to the point of greatest decline in segment 3 and a vertical corresponding to segment 4. In the normal breast, this angle must always be greater than 90°.
c. Degree of ptosis, is measured by the distance between a horizontal plane that passes through the lowest point of the submammary sulcus and a horizontal plane tangent to the lowest point of segment 3; normally it must be equal to 0 [5, 7].
Surgical Techniques
Different surgical techniques were performed depending on the type of ptosis. The principles of all techniques were based on excess skin resection, gland fixation, implant replacement in the submuscular plane, and ANC transposition. The approach through the submammary sulcus was performed in patients with light ptosis tributary to the change of implants of greater volume and when the previous approach indicated it. Periareolar closure was performed when the distance from the areola to the new position of the ANC did not exceed 2 cm, as well as cases where the distance between the submammary sulcus and the lower edge of the ANC was less than 8 cm. Vertical closure and combined with horizontal closure was chosen in patients with moderate or severe ptosis and with implants in the subglandular plane.
Intraoperative
The surgical procedure was performed with general anesthesia, asepsis and antisepsis with 10% iodopovidone solution or alcoholic hibitane, incision according to preoperative planning and dissection by planes until reaching the capsule, removal of the implant, sampling of the capsule for biopsy, cavity washing with antiseptic solution, modification or not of the pocket, exhaustive hemostasis is performed, new silicone implants are placed, drains are placed, flat closure to skin without tension and occlusive bandage.
Post-operative Care
In the immediate postoperative period, clinical hospital surveillance, intravenous hydration, antibiotic prophylaxis, analgesia is continued. The first local cure with alcoholic hibitane is performed the next day, a surgical wound is occluded, and a surgical adjuster and a stabilizing band are placed. If the patient recovers optimally and without complications, she is discharged from hospital the day after the surgical procedure.
The postoperative controls of the present study are performed at 6 months and one year.
Processing and Analysis of Results
The information is collected in data collection sheets and is summarized in a database in Microsoft Excel format using the Office 365 statistical package. Descriptive statistical measures are used to analyze the results. Variables are summarized in absolute numbers and percentages.
The aesthetic results of the treatment were classified as good, regular or bad: • Good: Sternal hairpin distance - ANC between 18 and 22 cm, in the breast with angle profile of segment 4 and tangent to segment 3 greater than or equal to 90°, distance between submammary sulcus and tangent to segment 3 is 0, there is symmetry, inconspicuous scar.
• Regular: When 3 or 4 of the stated criteria are reached.
• Bad: When less than 3 criteria are reached.
Results
36 patients with an average age of 36 years were evaluated, the age group between 33 and 46 years prevailed 61%, followed 25% for the group between 19 and 32 years and 14% over 47 years of age. Possible situations identified as causing breast ptosis were: tissue atrophy 56% followed by ptosis prior to mastoplasty increased 22%, breastfeeding 14% and weight loss 8%.
For the evaluation of ptosis, the Regnault classification was used [4]. In the series pseudoptosis prevailed in 27 patients, followed by mild ptosis in 8 patients, moderate ptosis in only 1 patient, and none had severe ptosis (Graph 1).
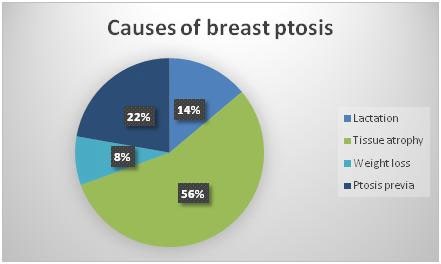
Source: Study database. Graph 1: Distribution of patients according to causes of postimplantation breast ptosis.
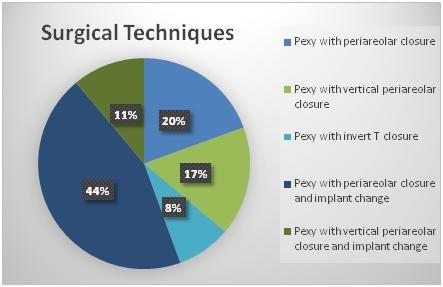
The most commonly used techniques for correction of ptosis secondary to augmentation mastoplasty with implants were pexy with an undefined pedicle, periareolar closure, and implant replacement with 44%, followed by pexy with an undefined pedicle and periareolar closure with 20%. The pexy technique with vertical periareolar closure was used in 17% of the patients; while 11% underwent pexy with an undefined pedicle, vertical periareolar closure and implant change. The least used technique was inverted T 8% of the patients and in all of them it was associated with previous scars (Graph 2).

Source: Study database. Graph 2: Distribution of patients according to surgical techniques.
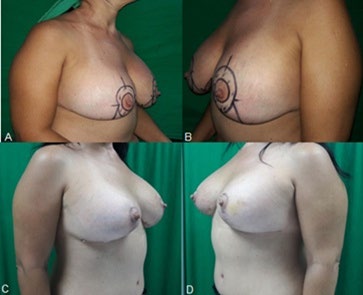
The preoperative measurement of the patients made it possible to aesthetically evaluate the results of the surgical treatment. 94.4% of the patients obtained a distance from the sternal fork to the ANC between 17 and 22 cm, and only 5.6% had 23 cm at that distance. 91.6% presented an intermamillary distance within the established parameter and 8.3% exceeded 1 cm. The desired distance between the ANC and the submammary sulcus and the midline was achieved in 100% of the patients (Figure 1). Regarding the breast seen in profile, the angle of segment 4 and tangent to segment 3 was greater than or equal to 90° in the entire sample and the distance between the submammary sulcus and the tangent to segment 3 was canceled in all cases; Breast symmetry was obtained in 91.6% and it was not reached in 8.3% of the evaluated cases; scars were inconspicuous in all patients (Figure 2). The aesthetic result was evaluated as good in 100% of the patients.
Discussion
In the study, most of the patients were in the age group between 33 and 46 years, with a mean of 36 years, which corresponds to what was found in the literature. Da Silva studies 64 patients with ages between 20 and 54 years, with an average of 34.5 years, Moya had 25 patients with predominance between 28 and 37 years and Zuleta includes 15 patients with an age range between 23 and 58 years, with an average of 37.5 years. This evidences the greater number of patients who undergo augmentation mastoplasties in the second decade or beginning of the third decade of their life; therefore, late complications such as postimplantation ptosis appear between 5 and 10 years after their initial intervention [8, 9, 10].
Mastopexy with silicone implants is one of the most frequent procedures in daily practice in Plastic Surgery. However, the poor quality of breast coverage, related to striated skin, little subcutaneous tissue, loss of the breast parenchyma secondary to prolonged lactation and massive weight loss, produce a progressive increase in unsatisfactory results in the medium and long term. This has been evaluated and discussed by many specialists [11].
In the series, the predominant cause of post-mastoplasty augmentation was tissue atrophy in patients who had undergone surgery for more than 5 years and who did not breastfeed or had significant weight loss after it, followed by poor management of previous ptosis implant placement. This is confirmed by the nonconformity of the patients with the appearance of their breasts due to ptosis shortly after surgery. In other words, the patients already had ptosis before the augmentation mastoplasty that persisted or resolved after surgery for a short period of time (between 3 and 6 months). Until now, tissue atrophy is impossible to avoid.
However, it is possible to modify the management of ptosis prior to implant placement with adequate treatment of ptosis prior to or simultaneously with implant placement. It is very common to use surgical procedures to correct moderate to severe ptosis only with the use of implants, which will inevitably end in persistence of breast ptosis. That is why combined techniques are recommended for the correction of breast ptosis and implant placement when volume increase is desired in a breast with moderate or severe ptosis and not only treat ptosis with the use of breast implants, however large they may be.
The etiology of implant augmentation post-mastoplasty breast ptosis is known to be multifactorial. The main causes are: physiological involution of the tissues, weight loss, breastfeeding and poor management of ptosis prior to implant placement. This study considers only the most important cause of implant augmentation post-mastoplasty breast ptosis. However, there are authors who consider more than one cause per patient such as Moya that mentions 3 causes: pregnancy (83.3%), lactation (79.1%) and weight loss (66%). The sum of all results in 229.1%, which is representative [9].
According to other studies, the management of this deformity becomes difficult as the postoperative period increases due to the atrophy of the tissues generated by the pressure exerted and maintained on them. For this reason the patient comes to consultation to improve the shape of the breast with a minimum of scarring [9].
In recent decades, numerous innovative procedures have been published to correct unsightly defects in breast ptosis. These are associated with loss of breast volume, flattening, and lack of filling of the upper quadrants. To improve the medium and long-term results of mastopexy and breast augmentation techniques, the quality of the breast envelope (skin and subcutaneous cell tissue) and the content (parenchyma, gland) are very important, depending on the characteristics of each [11].
20 patients underwent mastopexy and replacement of larger volume implants without exceeding 400 ml. The implant change was due to the patient’s desire to increase the breast volume or change the retroglandular to retromuscular plane. Only the increase in volume of the prostheses has been shown not to correct breast ptosis. However, the effects of tissue atrophy and relaxation due to the implant’s tissue expander are greater in the retroglandular plane. This is why changing the plane creates a more pronounced retroglandular space than in the retromuscular plane, which contributes to ptosis. By placing a larger volume implant associated with mastopexy, better redistribution of the atrophied or distended tissues is achieved and therefore greater occupation of the retroglandular plane space. That is why it is preferred to increase the volume of the implants when changing from retroglandular to retromuscular planes, as a complement to mastopexy in the correction of post- mastoplasty breast ptosis.
In patients with mammary ptosis with a retroglandular position of the breast implant, they underwent a larger volume prosthesis (up to 100 cc), a change from plane to retromuscular, and most of them periareolar mastopexy. With this technique it was possible to correct the position of the ANC up to 2 cm with a good aesthetic result, according to the measures used in the study methodology. Implant replacements were also made due to age between 5 and 10 years, most with implants of the same volume.
Although it is not the objective of the study, in the previous cases the volume, shape and texture of the initial implants could be verified, since the implants were changed during surgery. The volume ranged from 225 cc to 375 cc, the majority being 325 cc, all round and textured. These findings are in agreement with 3 other studies, ours being the one that found higher volumes in the implants. Ventura placed round, fine textured implants with a volume average of 275 cc (minimum 200 and maximum 400 cc). Berrocal placed round, textured surface silicone implants with average volumes between 200 and 275 cc in all his patients, and Vallarta Rodriguez used round, textured implants of highly cohesive gel from 230 cc to 375 cc [11, 12, 13].
The deformity found in most cases, according to the ptosis classification, was pseudoptosis. This corresponds to the consulted literature, which reports that implant mastopexy is one of the most complex and difficult procedures in breast surgery. The most frequent complications are pseudoptosis, ptosis and the cascade breast (bottoming - out), the latter in the placement of the implants in the submuscular plane [8].
The most frequent unsatisfactory results in mastopexy with implants in retromuscular position are the double breast contour, asymmetries and displacement of the implants. Some patients presented post-implant breast ptosis in the form of a double breast contour. This unsightly condition has been mentioned in the literature with many terms such as: double bubble breast, waterfall breast and sign of snoopy dog [11, 14].
Preoperative planning is done according to the type of ptosis, the excess amount of skin, the plication of the gland and the rise of the ANC. However, each patient has its variations, so a rigid pattern was not used. In the sample presented, the options were:
- Pexy with an undefined pedicle with periareolar closure.
- Pexy with an undefined pedicle with vertical periareolar closure.
- Pexy with indefinite pedicle with inverted T-closure.
- Pexy with an undefined pedicle with periareolar closure and implant change.
- Pexy with an undefined pedicle with vertical periareolar closure and implant change.
- Pexy with undefined pedicle with inverted T-closure and implant change.
Critical points when performing a mastopexy with implants, either primary or secondary, are the positioning of the ANC, the definition of a marking of the skin excision, the possible approaches, the possible implantation planes and the choice of implants. Depending on the degree of ptosis, it is important to know the distance from the sternal fork to the nipple to assess the elevation of the ANC over longer distances with more extensive scarring [12].
The most widely used surgical option for the treatment of post-mastoplasty augmentation ptosis was pexy with an undefined pedicle with periareolar closure and implant change, in 16 patients. Similarities and differences were found in the literature reviewed. There are studies where the predominant technique was inverted T, such as Da Silva, who performed a mastopexy with an inverted T closure in 61 of the 64 operated cases.8 Ventura with 60 patients made 2 groups. The first group underwent primary mastopexy with implants and the skin compensations were: 14 periareolar, 6 periareolar vertical and 5 inverted T. The second group underwent secondary mastopexies with implants, and the skin compensations were: 10 periareolar, 11 periareolar vertical and 14 inverted T.12The results of the mastopexies techniques used in the first group correspond to the results of the techniques used in this study, while those in the second group do not correspond. Other studies show that the most widely used technique is mastopexy with periareolar closure. There is no consensus on which technique to “use”, because it depends on multiple factors, such as: the degree of ptosis, previous scars, use of flaps, training and the surgeon’s preference for one or the other technique, etc [8, 12, 15].
The surgical technique used in the study coincides with the algorithm proposed by Cardenas in 2006 that choose the most appropriate procedure according to the degree of ptosis and the distance from the ANC to the submammary sulcus:
- If there is little ptosis of the ANC (<3 cm) and the distance from the ANC to the submammary sulcus is short (<5 cm), the ideal procedure to perform is only the pexy of the ANC.
- If the ptosis is moderate with little excess in the superior and inferior pole of the breast and the distance from the submammary sulcus to the ANC is between 5 and 7 cm and the pexy of the ANC is not greater than 3 cm, the ideal procedure is a pexy periareolar.
- In cases of severe ptosis with large cutaneous excess, a distance from the submammary sulcus to the ANC greater than 7 cm and there is a need to perform a pexy of the ANC greater than 3 cm, the indicated technique is an inverted or vertical T resection [4, 16].
It is difficult to predict whether the degree of elasticity of the skin and the stabilization procedures of the residual gland can counteract the action of gravity, therefore, to evaluate the postoperative results, it should be after 6 months to one year. A significant preoperative ptosis in the postoperative period tends to decrease the breast. The measures taken as a guideline to determine the aesthetic result were chosen from various sources; since these parameters vary according to different authors. For example, in Coiffman’s book the normal distance from the sternal fork to the ANC is 17-18 cm, while for Nelligan this measurement is normal between 19 and 21 cm [5, 17, 18, 19].
It is important to keep in mind that the concept of beauty is very subjective, for this reason it was also decided to use the measures proposed in this study to define the aesthetic results. An example of the subjectivity of beauty is the fact that many patients have the misconception that the nipple must be positioned right in the center of the breast and directed forward, however, the truth is that the nipple must be in the apex of the mammary cone, slightly off-center and towards the external and inferior segment. The study shows that the aesthetic result is good, since the 36 operated patients met at least 4 of the 5 treatment criteria. This was demonstrated in the postoperative controls at 6 and 12 months [5].
There are many surgical options and controversies surrounding the correction of augmentation post- mastoplasty breast ptosis. However, it can be said that no technique is ideal. The method that suits the patient’s needs and is preferred by the surgeon should be chosen. The treatment of post-implant breast ptosis is always surgical and offers good results if the technique is individualized to each patient.
Conclusion
Breast ptosis after augmentation mastoplasty with silicone cohesive gel implants is multifactorial in origin; reason why the treatment must be personalized to each patient and more specifically to each breast.
References
-
Taschen A (2005) Beauty and Plastic Surgery.In A. Taschen, Plastic Surgery. Italy: Taschen, pp: 10-5.
-
Navarro C (2016) Augmentation Mammoplasty. In: Coiffman F (Ed.), Plastic, Reconstructive and Aesthetic Surgery 4th (Edn.), Bogota: Amolca, pp: 1991-2015.
-
Meléndez F, Blejman O, Lamattina M, Villamea V, Sarquis F, et al. (2010) Evaluation of Breast Implants by Magnetic Resonance: Practical utility compared to other methods. Rev Colomb Radiol 21(3): 2967-2973.
-
Kube R, Zapata R (2014) Plastic Surgery of the breast. Venezuela: Amolca.
-
Bohorquez V, Roa TT (2016) Surgical anatomy of the breast. In: Coiffman F (Ed.), Plastic, Reconstructive and Aesthetic Surgery. 4th (Edn.), Bogota: Amolca, pp: 1835- 1850.
-
Maxwell GP, Allen G (2017) Augmentation Mastoplasty. In: Neligan PC (Ed.), Cirugia Plastica. 3rd (Edn.), Venezuela: Amolca, pp: 13.
-
Berrocal M (2014) The Four Seasons of Mama. Bogota. Amolca.
-
Da Silva Junior V, De Sousa Soares F (2017) Mastopexy with single-time implants associated with a non-areolar lower pedicle flap. Cir plast ibero-latinoam 43(2): 117- 28.
-
Moya E, Moya Y (2019) Treatment of breast ptosis using the modified Liacyr Ribeiro type I technique. Rev Arch Camagüey 23(1): 1-10.
-
Alí A, Zuleta C, Vassaro V (2013) Dermoglandular support flap in mastopexy with implants. Hammock technique. Cir plast ibero-latinoam 39(4): 361-368.
-
Berrocal Revueltas M (2013) Mastopexy with prosthesis: triplanar technique with fishtail flap for breasts with poor quality coverage. Cir plast ibero-latinoam 39(4): 414-419.
-
Ventura O (2017) Surgical sequence in augmentation mastopexy with implants. Importance of a neutral and multimodal approach. Cir plast ibero-latinoam 43(1): 3-10.
-
Vallarta RA, Ruiz JJ, Guerrero F (2014) Smart augmentation mastoplasty manipulating tissue vectors. Cir Plast 24(1): 40-49.
-
Mantilla JC (2018) Complications in breast surgery. MED UIS 31(3): 63-65.
-
Ramos L (2015) Surgical treatment of augmentation post-mastoplasty complications. Surgical Clinical Hospital Hermanos Ameijeiras: Havana.
-
Martinez SL (2012) History of breast implants. Your Med.
-
Coiffman F (2008) Plastic, Reconstructive and Aesthetic Surgery. 3rd (Edn.), Bogota: Amolca.
-
Habad JL, Hesiquio R (2014) Aesthetic and reconstructive breast surgery. 1st (Edn.), Bogota, Colombia.
-
De la Torre JI, Davis Michael R (2017) Anatomy for plastic surgery of the breast. In: Neligan PC (Ed.), Plastic Surgery. 3rd (Edn.), .Venezuela: Amolca, pp: 2.
- Reconstruction of Nasal Defect Using a Local Flap Based in the Nanoperforants Concept: A Case Report
- Transplant Tourism in Japan: Insights from Nationwide Surveys and Emerging Ethical Challenges
- The Challenge of Peritoneal Vaginoplasty in Transgender Women: Review Literature and Personal Perspectives
- Algorithmic Paternalism: Autonomy Versus Automation
- Dermatoscopy in Gorlin Syndrome: Avoiding the Disfigurement in Patients
- How Artificial Intelligence is Ushering in a New Era of Innovation in General and Plastic Surgery: A Short Communication