Evaluation of Delayed Pedicled TRAM Flap for Breast Reconstruction in High Risk Patients
Background: Breast reconstruction after mastectomy is among the most critical decisions for both the surgeon and the patient. Transverse rectus abdominis musculocutaneous (TRAM) flap has gained increased popularity and has become the standard for autogenous breast reconstruction. Despite the success with TRAM flap, it still has ischemic-related complication in high risk patients. Aims: To evaluate delayed TRAM flap for breast reconstruction in high risk patients. Patients and methods: Between June 2017 to June 2019, 8 female patients with age ranging between 28-55 years were presented to us with history of modified radical mastectomy. Those patients were subjected to two stage operation. The first stage involved delay of the TRAM flap and second stage involved transfer of the contralateral TRAM flap to reconstruct the breast. Results: 7 out of 8 patients had achieved satisfactory result regarding volume and shape of reconstructed breast with no flap necrosis, only in one of our patient had partial flap necrosis which was treated with simple surgical debridement with no further sequelae. Conclusion and recommendation: Delayed TRAM flap showed to be effective in reducing risk of flap necrosis in high risk patients with good and pleasing aesthetic result.
Introduction
Creation of breast mound that resemble preoperative dimension together with nearly normal position and contour that has long lasting are of prime aims and goals of breast reconstruction following mastectomy. TRAM flap remain the mainstay option in any breast reconstruction procedure since its introduction by Holmstrom and Hartramp in 1982 [1, 2].
In the United States, it had being estimated that 15% of mastectomy patient undergo breast reconstruction, any patient who had no local, neither systemic disease can be considered candidate for breast reconstruction after mastectomy. The main objective of breast reconstruction is to improve life quality of patient with breast cancer. Dean et al had reported increasing in psychological well- being with immediate reconstruction, since immediate reconstruction gave better aesthetic result than delayed reconstruction, owing to preservation of both skin envelope and inflammatory fold. In general using of autologous flap is preferable on the implant [3, 4].
Numerous modification had being introduced to TRAM flaps over years to increase its blood supply in high risk patient (overweight, smoker, receive radiotherapy) such as bi-pedicled TRAM flap, turbocharged TRAM, supercharged TRAM, and surgical delay [2].
Taylor study lead to significant improvement of our knowledge about the angiosome of abdominal wall. By his study on cadaver and using intravascular injection, he proved that there are arterial choke vessels of reduced caliber within the deep superior epigastric vessels in the rectus muscle and between vascular territories that located within the flap.
Experimental work had proved that the surgical delay will lead to choke vessels dilatation and so important in circulation of the flap. Also delay mechanism has been shown to improve venous return through improvement of reverse flow across venous valve. And by creation of collateral flow, venous pressure diminished during TRAM in setting in delayed TRAM [5].
The peri-umbilical perforators which arise from the deep inferior epigastric vessels supply the lower transverse abdominal flap, this was noted by Boyed et al. By delay procedure the reduced caliber of choke vessels that connected both the deep inferior and superior epigastric arteries will be dilated which as mentioned above improved the vascularity of the flap [6].
In this study surgical delay of TRAM flap which used for breast reconstruction was evaluated in high risk patients.
Patients and Methods
Between January 2017 and July 2019, 8 patients presented with history of mastectomy and they were subjected to breast reconstruction using 2 stages delayed pedicled TRAM island Flap. All operations were done at specialized burn Hospital and Ghazi Al Hariri Hospital/ Baghdad Medical City. Patients’ ages were ranging between 28 -55 years, and average time of reconstruction started at 1-2 years after mastectomy Patients’ data are shown in table -1- below:
| Age (y) | BMI | Breast side | Time of reconstruction post mastectomy (y) | Associated comorbidity | |
|---|---|---|---|---|---|
| 1 | 55 | 29 | Rt | 5 | Hypertension Radiotherapy |
| 2 | 46 | 30 | Lt | 3 | Overweight Radiotherapy |
| 3 | 28 | 26 | Lt | 2 | Radiotherapy |
| 4 | 39 | 28 | Lt | 4 | Radiotherapy |
| 5 | 52 | 32 | Lt | 1 | Obese Radiotherapy |
| 6 | 48 | 33 | Rt | 2 | Overweight Radiotherapy |
| 7 | 52 | 32 | Lt | 2 | Obese Radiotherapy |
| 8 | 42 | 29 | Lt | 3 | Radiotherapy |
Table 1: Patient’s data.
All of our patients had more than one year history of mastectomy for invasive ductal carcinoma, those patients were subjected to modified radical mastectomy, followed by chemotherapy, hormonal therapy and radiotherapy. They were selected according to the presence of redundancy and laxity in the abdomen, so that they are amenable to use TRAM flap for breast reconstruction concomitant with abdominoplasty. Those patients who had abdominal wall scar (upper abdominal incision with previous division of rectus abdominis muscle, history of abdominoplasty), patients with no abdominal wall laxity, heavy smoker patients and high BMI (>35) were excluded from our study. Preoperative evaluation was done to assess the amount deficiency at the mastectomy site, status of mastectomy scar (transverse or oblique) which affects the final flap inset, degree of abdominal wall laxity which can be assessed both in supine and erect position and can be confirm by classical diver test while patient in erect position .Before starting our reconstruction, a consultation with general surgeon and oncologist was done to confirm that there is no local recurrence or the presence of secondaries was conducted, and all patients were confirmed that they were tumor free.
Preoperative routine investigations were done for all of our patients and medical consultation for optimization of their condition. All patients sent for C.T. angiography to assess superior epigastric artery (patency, diameter). All patients sent for abdominal U S to exclude hernia and assess abdominal organs condition.
All patients were instructed to stop Tamoxifen treatment 5 days before operation and 5 days postoperatively. Preoperative consent were taken from all patients involved in this study.
1st stage operation (delay) was approximately one hour duration, while time of second stage operation (pedicled TRAM flap for reconstruction ) was about 3.5-4 hours.
Operative Technique
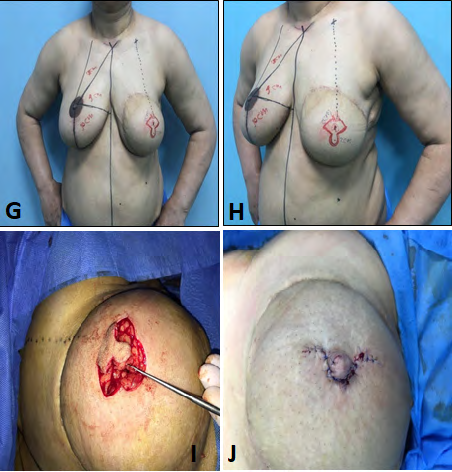
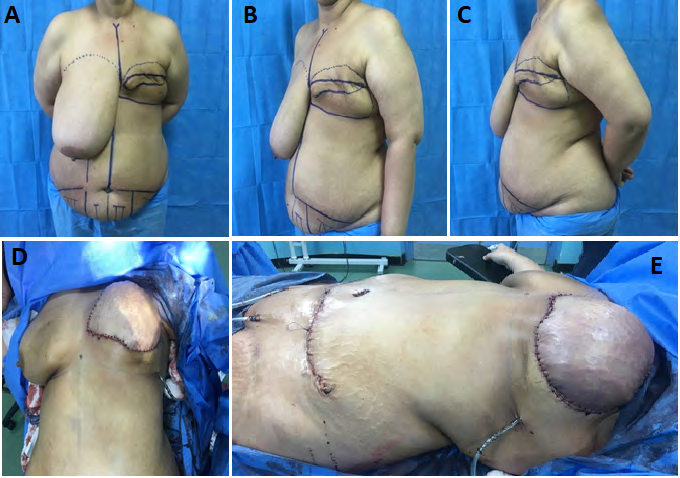
All operation were done under general anesthesia with the patient in supine position. Marking while patient in erect position was performed. The superior margin of abdominal flap is marked as a line that curves 1.5 cm just above the umbilicus and extended toward the anterior superior iliac spines, the lower margin of flap is drawn from the supra- pubic crease along the natural fold line and curving upward toward the anterior superior iliac spines to meet the upper previously marked lines which can be modified according to Case No. 1:
availability and laxity of lower abdominal skin. The distance between the two lines designed so that they meet each other without tension.
The midline is marked from sternum to pubis, then zones of TRAM flap marked as Hartrampf classification as follow; Zone I directly overlying the rectus muscle that will be transfer in second stage. Zone II overlying the contralateral rectus muscle, zone III is ipsilateral to the pedicle, while Zone IV is ipsilateral to zone II.
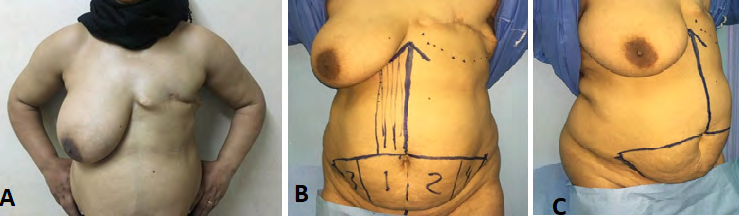
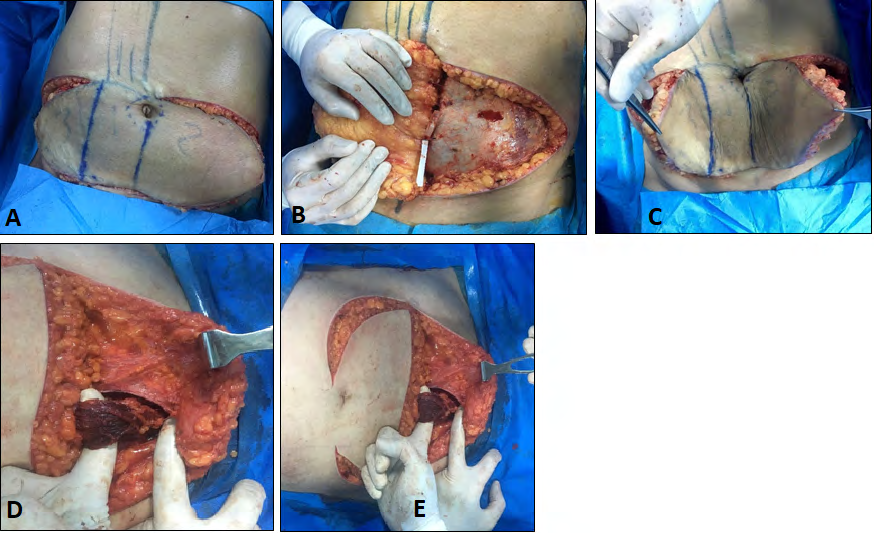
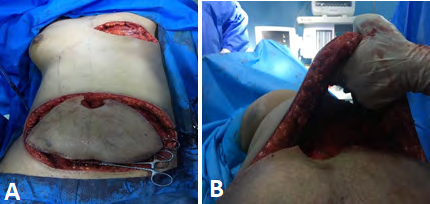
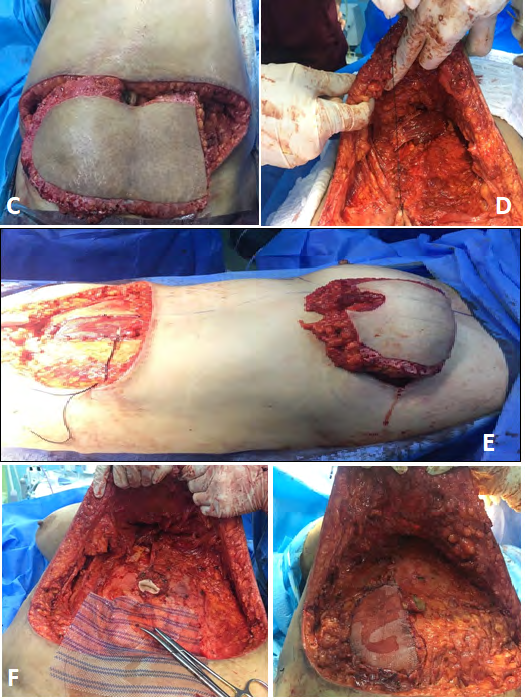
Our design were done so that the contralateral muscle is utilized in the second stage (contralateral to mastectomy site). operation then begins by using No. 24 blade, the skin and subcutaneous tissue is incised along the previously marked lines, then by using electrocautery, the zone II and zone IV and zone III are elevated at the level of the underlying rectus sheath , keeping zone I attached to rectus muscle without elevation (Figure 10).
In order to ligate all branches of deep inferior epigastric artery, we identified the inferior epigastric artery using intra-operatively hand held Doppler, transverse incision was done at the inferior portion of rectus sheath that related to zone I and the most lower part of muscle was exposed, we interrupted the lower portion of transverse rectus muscle near its origin by using 2-0 polyglactine suture to ligate all branches of DIEA. After that the rectus sheath is repaired using 3-0 polyglactine suture.
After we ensured adequate hemostasis, silicon sheath was used beneath the elevated flaps in zone II, IV and III, and is fixed to the underlying fascia by multiple 3/0 polyglactin simple interrupted suture, in order to prevent the adhesion of the elevated skin paddles to the underlying fascia. The skin incision is closed by single layered closure with running fashion using 2/0 proline suture. Two redivac drains size 18 were used, and the patient was discharged in the next day, keeping her on injectable 3rd generation cephalosporin for 3 days post operatively, then continued on oral antibiotics for at least 7 days, the drains were removed after 5 days. Second stage surgery deginitive TRAM flap reconstruction was done 3 weeks later.
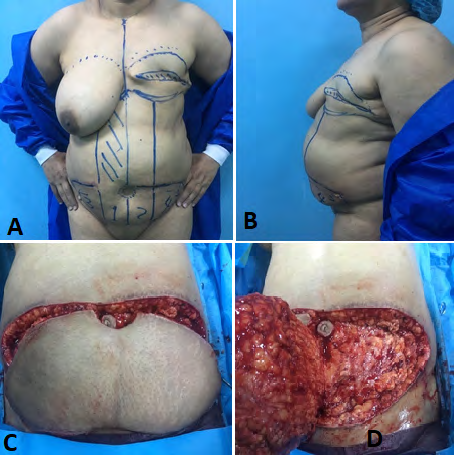
After 3 weeks, patients were subjected to a second stage TRAM flap reconstruction, and preoperative marking done as the same as the 1st stage plus skin marking for designed flap along longitudinal underlying muscle, marking for borders of breast mounds and bilateral infra-mammary folds.
The operation began by circumferentially incising the umbilicus using No.15 blade and keep it attached with a cuff of surrounding fat to Linea alba, so that is maintained its blood supply. Then lower abdominal incision is made, and is carried down to abdominal muscle fascia, after that upper incision which is located about 1.5 cm above the umbilicus, is carried down. When superior incision is made, care should be taken so that the dissection is beveled superiorly in order to preserve superior perforators in the flap. Dissection above the umbilicus is carried supra-fascially to xiphoid process. After finishing the upper and lower incisions, with use of electrocautery, the flap in zone IV and II are raised up to the midline, and then the zone III flap is raised up to the lateral border of ipsilateral rectus sheath of zone I. The previously applied silicon sheath exposed which is fixed to the underlying tissue; the silicon sheath is elevated carefully from its underlying attachment and discarded.
The rectus sheath is incised 2 cm from midline, then complete dissection of the muscle medially and laterally is done in order to utilize the whole bulk of the muscle and ensure the continuity of superior epigastric artery. Tendinous intersections were dissected by blunt scissors in order to avoid injury to vessels and underlying posterior rectus sheath, the inferior portion of rectus muscle is grasped by single long forceps and then by using electrocautery the muscle is horizontally transected, the muscle is elevated easily by using simple finger dissection from caudal to cephalic direction up to 2 cm below the costal margin. During muscle elevation, the superior epigastric artery can be noticed and confirmed by hand held Doppler, which runs longitudinally in the central part of muscle.
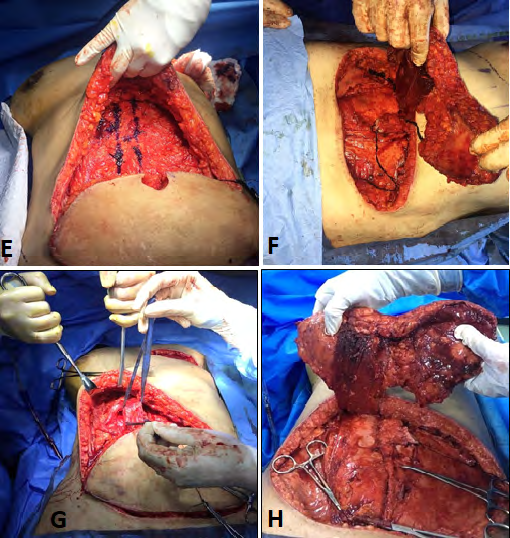
After complete elevation of the flap, the recipient site is prepared. The mastectomy scar is excised and the mastectomy pocket is created, the skin and subcutaneous tissue of the mastectomy site is undermined to create a tunnel for flap passage. We make sure that the tunnel had adequate width so that it will not lead to kinking and compression of the pedicle when it is rotated to inset at the recipient site.
The flap is then rotated in counter-clock wise or clock wise direction according to the position of mastectomy site after discarding zone IV and part of zone II. The flap is inset so that the zone II oriented medially, zone III laterally oriented and zone I is located at center. After that the flap is fixed to the chest wall using anchoring stiches (2/0 polyglactin suture). The proposed infra-mammary fold is created by interrupted sutures that fix the dermis of mastectomy flap into underlying chest wall fascia using interrupted 3/0 polyglactin suture. Then the recipient site is closed with dermal stiches using 2/0 polyglactin interrupted sutures and the skin is closed by 3/0 interrupted prolene suture. Closed suction drain (redivac, size 12) is inserted through separated stab incision on the skin of anterior axillary line and fixed in its position by No. 0 silk suture.
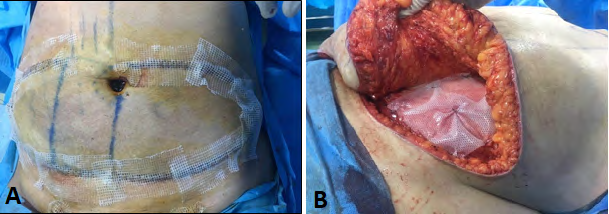
Then the lateral fascial edge approximated to the Linea Alba without tension. In all of our cases prolene mesh was applied over the lower rectus sheath starting at level of Arcuate line at lower abdomen and fixed in its position using 3/0 prolene suture . The abdominal flap then closed using 2 layers closure, first dermal interrupted suture using 2/0 polyglactin suture, skin incision then closed using sub- cuticular 2/0 proline suture. Two drains were applied that exit from the supra-pubic region, fixed by No. 0 silk. Dressing is applied for both donor and recipient site using antibiotic impregnated gauze as first layer, and then Betadine gauze as second layer, then dressing is secured in its position using adhesive plaster.

Patient discharged to the ward keeping them on slowly infusion pump of paracetamol and NSAID analgesia with maintenance I.V. fluid, also patients kept on low molecular weight heparin (4000 I.U. S.C. ) for 5 days post operatively with injectable 3rd generation cephalosporine. The patient is instructed to ambulate in the second day (day 1 post operation), where the foley’s catheter is removed. The flap is inspected after 2 hours from discharging to ward to check color and viability in the 1st 24 hours, and then every 6 hours in next days, until patients were discharged in 4th post- operative day. On discharge, the patients were kept on pentoxyphyline tab for 5 days, also kept on oral antibiotics till the 14th day postoperatively were sutures and all drains are removed.
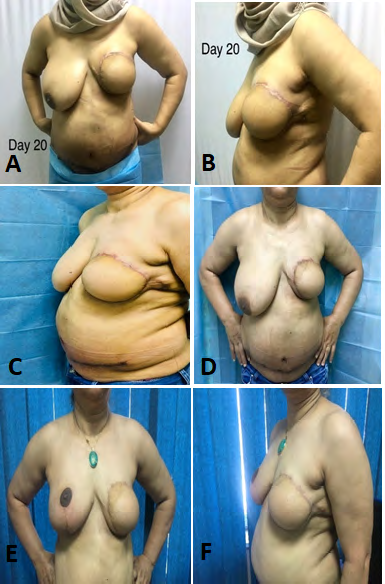
The follow up continues every 2 weeks in the1st month then every 1 month until (12-18) months. In all patients surgical contouring of the contralateral breast was mandatory (which include mastopexy or reduction mammoplasty) and this was done after 4-6 months to match the size of the reconstructed breast, then nipple reconstruction was done 1 month after contouring of the natural contralateral breast by using C.V. flap. Areolar tattooing was done after 3 months from nipple reconstruction. Patients were kept on regular follow up period which was extended up to 12-18 months post operatively.
Results
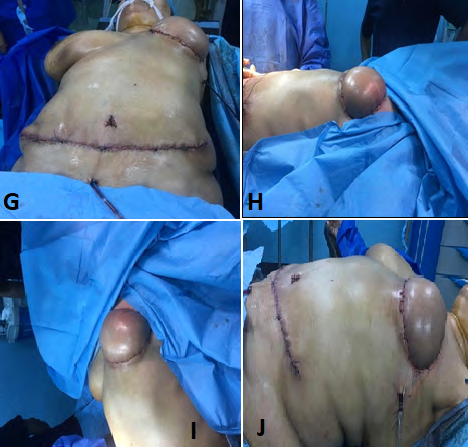
All flaps had been completely survived with 1 reported case of partial flap necrosis at medial side of the reconstructed breast which was treated by surgical debridement and resuturing of the flap.
Patient’s satisfaction was evaluated by directly asking the patient about her satisfaction with postoperative breast appearance and abdominal shape. Seven of our patients were satisfied, one of our patient was not completely satisfied and her main concerned was about breast asymmetry.
Patients were evaluated subjectively, a good breast shape and projection were obtained in all of our patients, with nearly symmetrical in size to the contralateral breast after (reduction mammoplasty or mastopexy) which was done in 6 out of 8 patients as follow: 5 of them had inferiorly based pedicle reduction-mammoplasty and in one patient had vertical pattern mastopexy. One patient was refused operation on contralateral normal breast, and one patient already has symmetry of other side. No reported case of abdominal flap necrosis or wound dehiscence, only one patient had developed seroma which was evacuated using large bore needle successfully without further sequelae. No abdominal wall hernia was noticed in our patients, The resultant scar, whether for donor or recipient site was acceptable, except for one patient which presented with hypertrophic scar at donor and recipient sites.
During follow up period, we kept contact with patient’s oncologist to exclude any recurrence of tumor, and all of our patients were free from recurrence during follow up period which was extended up to 12-18 months postoperatively. All patients were instructed to starting exercises for abdominal wall muscles strengthening after 1 month post-operatively.
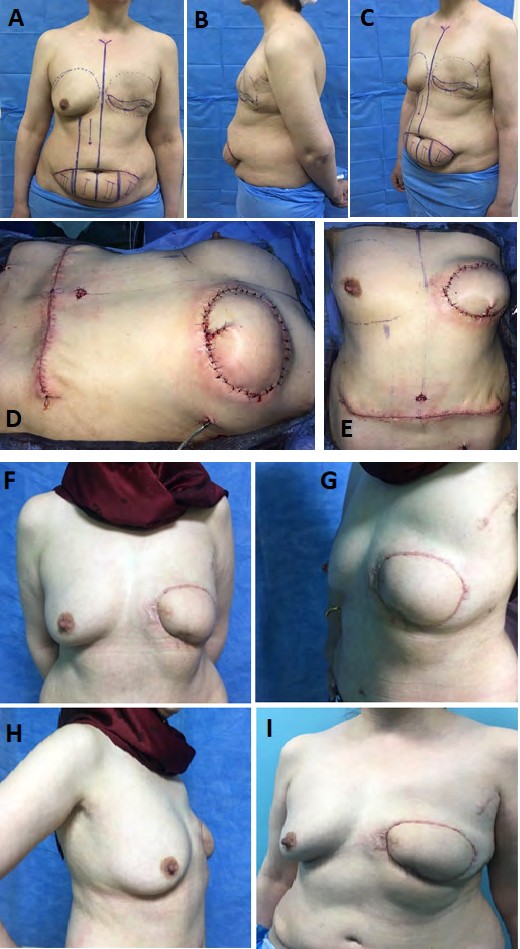
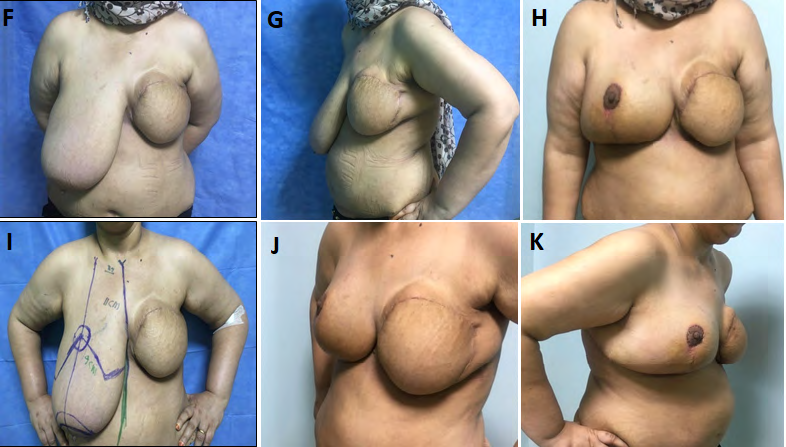
Case No. 2
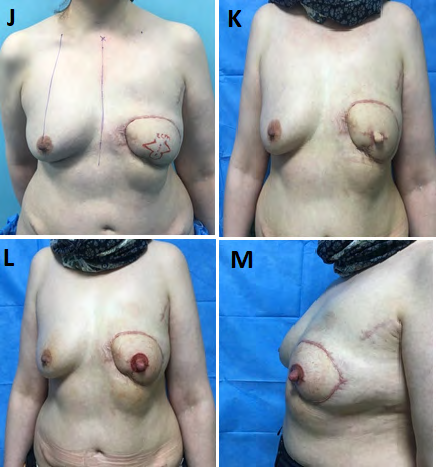
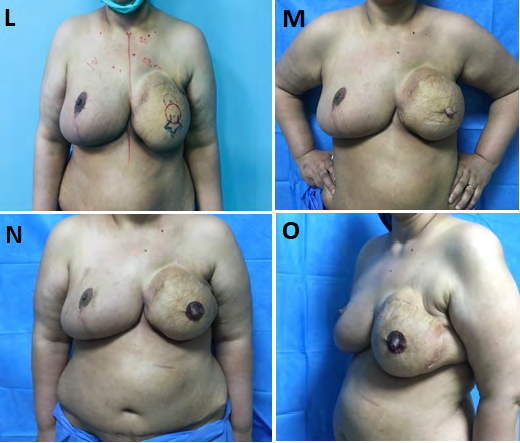
Case No. 3
Discussion
One of the most devastating problems with using of TRAM flap for breast reconstruction is ischemia and fat necrosis which may occur in 5 to 28% of cases. In large series, breast reconstruction with TRAM flap was done in 729 patients between 1981 to 1991, it was associated with high rate of flap ischemia (12%) which was noticed especially in those patients who had risk factors , for example obesity, smoking, abdominal scar and radiation [7].
One of the methods which have been used to enhance blood flow to TRAM flap and decrease the incidence of flap necrosis especially for those patients who had risk factors, is using of surgical delay whether by ligation of deep inferior and superficial inferior epigastric vessels or by extensive flap undermining or both as it was adopted in our study [1].
Surgical delay of TRAM flap by undermining of lower abdominal skin paddles (except for zone I) and ligation of inferior epigastric artery was used successfully in 8 patients who were presented to us with history of mastectomy (modified radical mastectomy). All flaps had shown excellent viability except one case had developed partial necrosis medially which was managed by surgical debridement. Although an ipsilateral pedicled TRAM flap transfer reduces epigastric bulging after flap inset, in our study all pedicled TRAM flap were chosen to be contralateral to mastectomy site, since using contralateral TRAM flap result in less twisting of pedicle during tunneling, also it provides natural breast fullness. Delay procedure which was used in this study showed it’s a reliable method for those patients who had risk factors (obese, received radiotherapy) where no patients were needed to return back to operating room for re-exploration. The aesthetic outcome was quite satisfactory for both the surgeon and patients (except in one patient), the constructed breast had pleasing volume and projection in comparison with the contralateral breast. No donor site morbidity were encountered in all of our patients, e.g. abdominal wall hernia, and the scar whether for recipient or donor site was accepted, except for 1 patient who had developed hypertrophic scar at donor and recipient sites. In our procedure we used silicon sheath as a barrier between the undermined flaps and the underlying tissues, so that we ensure adequate and effective delay of TRAM flap with no blood vessels connection that might occurred between the flap and its underlying bed. In all of our cases we informed our patients to stop taking Tamoxifen at least 5 days before operation in order to reduce the risk of flap necrosis, since in a study which was conducted by Kelley et al had shown that Tamoxifen may increase the risk of microvascular flap complications in patients undergoing microvascular breast reconstruction [8].
Restifo, et al. proved that after delay procedure for TRAM flap, there will be increase in both diameter and blood flow of superior epigastric artery. They found that the mean diameter of superior epigastric artery, it increased after delay from1.3+0.2 to1.8+0.3(p value < 0.001), also they found that the flow in superior epigastric artery increased from 7.25 +o.8 to 18.2+0.3 ml /min (p value < 0.001) after delay of TRAM flap. Another study which was conducted by Mark A Codner, et al. had shown that TRAM perfusion pressure was increased from 13.3 mm Hg (control ) to 40.3 mm (delayed ) in mid rectus perforator region (p value < 0.05) [9, 10].
Extended skin paddle delay of uni-pedicle TRAM flap was done in 35 patients by J-Arthur Jensen, et al. [11]. Those patients were active smoker (11 patients), 16 of them had radiation therapy, and 14 of them had undergone chemotherapy. Their results showed that all flaps survived with no reported case of flap necrosis, only 10% of their patients had partial fat necrosis which was attributed to medial stiches that used to inset the flap to pectoral fascia, in order to decrease this complication, they minimize the number of medial stiches and they notice complete absence of fat necrosis in subsequent cases. The results of the above mentioned study is in general consistence with our study.
Detlev Erdman et al. performed surgical delay of TRAM flap by ligation of deep inferior epigastric vessels through incision at inferior border of the flap down to the fascia. In his series 76 cases were subjected to delay, those patients showed no flap necrosis. In 5.6 % of cases, partial fat necrosis occurs. This percent according to Detlev Erdman, et al. is nearly comparable to partial fat necrosis that occur after free TRAM flap (which is range between 0- 7 %) [2]. We believe that delay augment blood supply even in patient with no risk factor, to make the flap more tolerable for ischemia, also it enable us to easily manipulate the flap during insetting, thus we achieve better breast mound and projection. Although delay procedure is two stage operation and had associated with risk of the anesthesia and postoperative deep venous thrombosis, the benefit of delay is out weighting the disadvantage of single procedure, we did not encounter postoperative case of DVT, as we instruct the patient for early ambulation and the use of prophylactic dose of low molecular weight heparin.
One of the method that had been used to improve blood supply to TRAM flap in patient with risk factors is using double – muscle pedicle TRAM flap, were the flap is transfer on both rectus muscle to increase its blood supply. However, bipedicle TRAM flap had major disadvantage, it will sacrifice both recti muscles which is associated with abdominal wall morbidity and loss of abdominal wall musculature and increase the risk of hernia.
Using of free – TRAM flap for breast reconstruction for patient with high risk factor remain optimum option, but its time consuming operation, needs high skill and practice. Free TRAM flap carry risk of complete flap necrosis with frequencies up to 10% [5, 10].
TRAM can be supercharged by microvascular anastamosis of inferior epigastric vessels to thoracodorsal vessels. However, still this procedure also needs experience in microvascular surgery. In study which was conducted by El-Mrakby HH, he found that the incidence of vascular complication in supercharged pedicle to be as twice as that associated with free flap (36% vs 18%) [12].
Preoperative selection deep inferior epigastric embolization that proceed ipsilateral unipedicle TRAM flap operation is another option for TRAM delay, it is not invasive procedure and can be carried out under local anesthesia as an outpatient, this procedure enhance the reliability of pedicled TRAM flap, however this procedure needs expert radiologist and special facilities, so that it is regarded as more complex and expensive when we compare it with our procedure [13].
Conclusion and Recommendation
Delay procedure for TRAM flap provides simple method that augmented its blood supply that can be used for high risk patients and even in not high risk patients. It reduced the incidence of flap necrosis in high risk patients. Though it two stages operation, the average time is much less than of free- flap and in contrast to free flap, it required no microvascular experience and it cost less-effective.
References
-
Sheina AM, Esta SB, Edward WB, Peter AL (2017) Evidence- Based Medicine, Autologous Breast Reconstruction. Plastic reconstructive Surgery 139(1): p204e-229e.
-
Detlev E, Burton M Sundin, Kenneth J Moquin, Henry Young, Gregory S Georgiade (2002) Delayed in Unipedicle TRAM flap reconstruction of the breast, A review of 76 consecutive cases. Plast Reconstr Surg 110(3): 762-767.
-
Stephan J Mathes (2006) Mathe’s Plastic Surgery. 2nd (Edn), Saunders Elsevier, Philadelphia, pp: 687, 673, 674, 761, 762, 752.
-
Urban C, Reitjens M (2013) Oncoplastic and Reconstructive breast surgery. 1st (Edn.), Springer-Verlag Italia, pp: 3, 77, 29, 298, 299, 300, 301, 302.
-
Taylor GI, Corlett RJ, Caddy CM, Zelt RG (1992) An anatomic review of the delay phenomena II: clinical applications. Plast Reconstr Surg 89(3): 408-416.
-
Boyd JB, Taylor GI, Corlett R (1984) The vascular territories of the superior epigastric and the deep inferior epigastric systems. Plast Reconstr Surg 73(1): 1-16.
-
Thaller S, Panthaki ZJ (2012) Aethetic and Reconstructive breast surgery, solving complications and avoiding unfavorable results. Informa healthcare, UK, pp: 102.
-
Kelley BP, Valero V, Yi M, Kronowitz SJ (2012) Tamoxifen increases the risk of microvascular flap complications in patients undergoing microvascular breast reconstruction. Plast Reconstr Surg 129(2): 305-314.
-
Restifo RJ, Ward BA, Scoutt LM, Brown JM, Taylor KJ (1997) Timing, magnitude, and utility of surgical delay in the TRAM flap: II. Clinical studies. Plast Reconstr Surg 99(5): 1217-1223.
-
Codner MA, Bostwick J, Nahai F, Bried JT, Eaves FF (1995) TRAM flap vascular delay for high-risk breast reconstruction. Plast Reconstr Surg 96(7): 1615-1622.
-
Jensen JA, Handel N, Silverstein MJ, Waisman J, Gierson ED (1995) Extended skin island delay of the unipedicle TRAM flap: experience in 35 patients. Plast Reconstr Surg 96(6): 1341-1345.
-
El-Mrakby HH, Milner RH, McLean NR (2002) Supercharged pedicled TRAM flap in breast reconstruction: is it a worthwhile procedure. Ann Plast Surg 49(3): 252-257.
-
Serletti JM, Taub PJ, Wa LC, Slutsky DJ (2013) Current reconstructive surgery. 1st (Edn.), McGraw Hill Medical, New York, pp: 503, 504.
- Reconstruction of Nasal Defect Using a Local Flap Based in the Nanoperforants Concept: A Case Report
- Transplant Tourism in Japan: Insights from Nationwide Surveys and Emerging Ethical Challenges
- The Challenge of Peritoneal Vaginoplasty in Transgender Women: Review Literature and Personal Perspectives
- Algorithmic Paternalism: Autonomy Versus Automation
- Dermatoscopy in Gorlin Syndrome: Avoiding the Disfigurement in Patients
- How Artificial Intelligence is Ushering in a New Era of Innovation in General and Plastic Surgery: A Short Communication