Reductive Mastoplasty with Medial Pedicle Flap in Patients with Symptomatic Breast Hypertrophy
Introduction: Breast hypertrophy is the abnormal increase in the volume of the breast associated with local osteomyoarticular and respiratory symptoms. Surgical treatment consists of reducing the size and improving the shape of the breast while preserving the ability to breastfeed. Objective: To evaluate the results of Reductive Mastoplasty with a medial pedicle flap. Method: Descriptive, prospective and longitudinal study in the Plastic Surgery Service of the Ameijeiras Hospital in 35 patients with a diagnosis of symptomatic breast hypertrophy who underwent Reductive Mastoplasty using the monopediculated Strombeck technique from January 2015 to December 2017. Results: Patients under 45 years old predominate with 57%. The most frequent symptoms are shoulder pain in 71% and back pain in 37% associated with very important breast hypertrophy in 55%. Stage E breast ptosis prevails in those less than 45 years with 60%. The median of resected tissue is less than 500g with a range between 300 and 750g without significant differences between both breasts. There is significant variability of anthropometric measurements in the pre and postoperative period with minor complications such as unaesthetic scar in 5.7%, wound dehiscence in 2.9% and sensitivity disorders in 2.9%. The evaluation of satisfaction and quality of life according to the Breast–Q scale reports improvement in all the aspects evaluated. Conclusions: Reductive Mastoplasty with internal monopediculate flap is a technique that offers good aesthetic results and few complications in patients with symptomatic breast hypertrophy.
Introduction
Breast hypertrophy is a medical condition that occurs due to the abnormal increase in volume of the breast Conceptual Paper associated with physical and emotional suffering in women. Symptoms vary from local symptoms such as infectious and inflammatory processes to regional symptoms such as osteomyoarticular pain, thoracic deformity and nerve compression [1, 2, 3].
Treatment is always surgical and favors quality of life. The surgery to reduce the size of the breasts is the Mastoplasty or Reductive Mammoplasty which consists of reducing fat, glandular tissue and skin with the aim of reducing the size, improving the shape, guaranteeing a long-lasting result, preserving the viability of the Nipple- Areola Complex (NAC) and lactation capacity [4]. Reductive Mastoplasty is a plastic surgery technique that constitutes an interface between the aesthetic and the reconstructive. The most recent techniques are based on old publications with additional surgical details that improve the resulting scar, but preserve the vascular pedicles and guarantee the nutrition of the NAC. The modern history of Reductive Mastoplasty begins with Strombeck in 1960 modifying the Wise cast and creating a horizontal bipediculate flap technique. In the 20th century, it became more popular with the advances in anesthesia and changes in the morals of society. Starting in 1960, techniques that respect the glandular cutaneous unit appeared with Strombeck (1960), Pitanguy (1961), Mckissock (1972), Weiner (1973), Robbins (1977), marking an important step in the development and diffusion of the aesthetic and breast surgery [5, 6]. The Strombeck technique revolutionized reduction mastoplasty procedures with the transfer of the areola onto a bipediculated horizontal dermoglandular flap, which is later transformed into an internal pedicle flap. It is performed mainly in large mammary hypertrophy, although it is difficult to perform in breasts with a large fat component [7].
Currently, there are few national publications about the results of Reductive Mastoplasty with medial pedicle flap without applying a satisfaction and quality of life survey using internationally validated questionnaires. The evaluation of the satisfaction of the patients with the aesthetic results is the way to know the effectiveness of the surgical technique. The plastic surgeon must face the challenge of meeting the expectations of the patients by evaluating their satisfaction, because their vision may not coincide with that of the patient [8, 9]. This study is carried out with the objective of evaluating the results of the Reductive Mastoplasty with medial pedicle flap.
Method
A descriptive, prospective and longitudinal study is carried out in the Department of Plastic Surgery and Caumatology of the Hermanos Ameijeiras Clinical Surgical Hospital in 35 patients with a diagnosis of symptomatic breast hypertrophy who underwent Reductive Mastoplasty with a monopediculated Strombeck surgical technique from January 2015 to December 2017.
Inclusion Criteria:
- Age ≤19 years to 60 years.
- Patients who gave their written informed consent for the study.
Exclusion criteria Patients with altered paraclinical examinations, acute or chronic decompensated illnesses, psychiatric disorders, breast cancer, breast scars that could compromise the blood supply of the flap, smokers, pregnant women and those who are lactating.
Preoperative consultation: The patients are classified according to the degree of breast hypertrophy. A preoperative and pre-anesthetic check-up is indicated. The benefit of surgical treatment, possible complications is explained, doubts are clarified and the informed consent is signed. General data, weight, height, body mass index, pathological history, preoperative anthropometric measurements, breast volume, degree of ptosis, reduction wishes; projection and morphology of each patient are recorded. A photographic record is made and hospital admission is indicated.
Preoperative indications: Free diet until 6:00 p.m. and liquid diet until 6 hours before surgery. Antibiotic prophylaxis with cefazolin 3 g (1 g preoperative, intraoperative and postoperative) and diazepam 5 mg 1 tablet orally is indicated at 10:00 p.m. the day before the operation.
Measurements for preoperative planning and evaluation of results: Distance between the sternal fork and the NAC, the distance between nipple and nipple in standing and supine position, the NAC diameter, the breast volume according to the Bowman method, the hypertrophy classification for breast volume according to Roa [10], and the classifications of divergent ptosis and vertical ptosis, according to the Kirwan scale [10].
Monopediculated Strombeck surgical technique: Patient in supine position with arms extended at shoulder level, under general orotracheal anesthesia, asepsis and antisepsis are performed, and sterile drapes are placed in the operative area. The incision is planned according to classical marking with the Wise pattern, starting with a periareolar incision and de-epithelializing the internal monopediculate flap. A mammary cone is excised at the level of the upper pole and incised until reaching the pectoral plane. The medial pedicle is defined and glandular resection is performed from the lower and external pole to the pectoral fascia. The transposition of the NAC is carried out with its movement upwards after releasing its insertion into the deep plane as necessary, until it rotates without tension. The NAC is placed in the area previously created for implantation. The flap is fixed at its upper pole; hemostasis, drainage placement, and plane closure are performed.
Postoperative care: In the immediate posoperative period, rest in the semi-Fowler position, intravenous hydration, antibiotic prophylaxis, analgesia and symptomatic treatment are indicated. The first healing of the surgical wound is performed the next day with an alcohol dry technique, occluded with a sterile dressing and a surgical adjuster. After the cure, if there are no complications and the recovery is satisfactory, the patient is discharged with follow-up in the outpatient clinic until the areola points are removed after 10 days and the rest between 15 and 21 days. Evaluation of the aesthetic results of the surgical treatment: To evaluate the results, volumetric and longitudinal anthropometric measurements are taken after surgery (6 months and 1 year). Photographs are taken in a frontal, profile and oblique position on both sides and the symmetry between the two breasts is measured. Patient satisfaction is evaluated based on the Breast–Q scale and complications (minor and major).
Procedure for the analysis of the information and statistical processing: The data obtained were collected in a database in Microsoft Excel version 3.0 and processed using the statistical package SPSS 17.1. The information is presented in tables and graphs. Descriptive statistical measures are used to summarize the data, for qualitative variables the absolute and relative frequency expressed in percentages is determined; while for the quantitative variables the median, the range and the standard deviation are determined. Two-entry contingency tables are prepared with the descriptive statistics summary measures indicated.
The research is approved by the Scientific Council and the Ethics Commission of the institution. It is carried out in accordance with the principles of medical ethics, current national institutional ethical standards and the principles of the Declaration of Helsinki.
Results
In the study, women under 45 years old predominate with 57%.
The main symptom that motivates the consultation is shoulder pain in 71%, followed by back pain in 37%, postural change in 17%, erosions and marks with 14%, intertrigo at the level of the submammary groove in 11%, discomfort with the clothes in 11%, feeling short of breath in 6% and difficulty in performing daily activities in 3%. More than one symptom occurs in all patients. Anthropometric variables include measurements and breast volume to determine the degree of breast hypertrophy and the relationship with the patient’s age (Table 1).
| Variable | Category | Less than 45Years | 45 Years or More | P | ||
|---|---|---|---|---|---|---|
| N | N | |||||
| R NAC-Fork (cm) | Median / IR | 20 | 25.0/ 24.0-25.8 | 15 | 24.0/ 23.0-25.0 | 0.082** |
| Range (Min-Max) | 23.0-27.0 | 23.0-27.0 | ||||
| L NAC-Fork | Median / IR | 20 | 25.0/ 25.0-26.0 | 15 | 24.0/ 23.0-25.0 | 0.033** |
| Range (Min-Max) | 23.0-29.0 | 23.0-29.0 | ||||
| R NAC Diameter (cm) | Median / IR | 20 | 6.0/ 5.0-7.0 | 15 | 6.0/ 5.0-7.0 | 0.096** |
| Range (Min-Max) | 5.0-7.0 | 5.0-7.0 | ||||
| L NAC Diameter | Median / IR | 20 | 6.5/ 6.0-7.0 | 15 | 6.0/ 5.0-7.0 | 0.052** |
| Range (Min-Max) | 5.0-7.0 | 5.0-8.0 | ||||
| R NA- Navel (cm) | Median / IR | 20 | 19.5/ 18.0-21.0 | 15 | 19.0/ 18.0-20.2 | 0.464** |
| Range (Min-Max) | 15.0-26.0 | 17.0-21.0 | ||||
| L NAC-Navel | Median / IR | 20 | 18.0/ 18-19.6 | 19.0/ 18.0-20.0 | 0.541** | |
| Range (Min-Max) | 15.0-22.0 | 16.0-23.0 | ||||
| Intermamillary Distance (cm) | Median / IR | 20 | 25.0/ 24.0-26.0 | 15 | 25.0/ 24.0-26.0 | 0.757** |
| Range (Min-Max) | 23.0-26.0 | 23.0-27.0 | ||||
| R Breast Volume (ml) | Median / IR | 20 | 1100.0/ 922.5-1237.0 | 15 | 880.0/ 850.0- 1258.0 | 0.124** |
| Range (Min-Max) | 850.0-1400.0 | 810.0-1480.0 | ||||
| L Breast Volume | Median / IR | 20 | 1150.0/ 932.0-1267.0 | 15 | 890.0/850.0-1300.0 | 0.109** |
| Range (Min-Max) | 850.01450.0 | 830.0-1490.0 | ||||
| R Breast Hypertrophy (%) | Significant Hypertrophy | 9 | 45 | 10 | 66.7 | 0.190*** |
| Very Significant Hypertrophy | 11 | 55 | 5 | 33.3 | ||
| L Breast hypertrophy | Significant Hypertrophy | 9 | 45 | 10 | 66.7 | 0.190*** |
| Very Significant Hypertrophy | 11 | 55 | 5 | 33.3 |
Table 1: Preoperative anthropometric measurements.
In relation to the degree of breast hypertrophy, 19 patients presented with significant breast hypertrophy and 16 patients very important. Of these, 11 women with very significant breast hypertrophy and 9 with significant breast hypertrophy were under 45 years of age. Those over 45 years of age present 5 very significant breast hypertrophy and 10 significant breast hypertrophy (Graph 1).
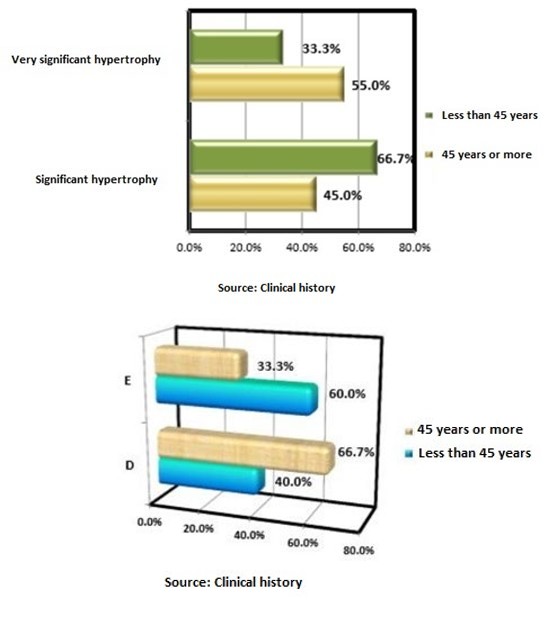
Graph 1: Distribution of patients according to degree of breast hypertrophy and age.
Regarding the degree of breast ptosis, 17 patients were presented with the nipple 2 cm below the submammary groove and 18 patients 1 cm from the submammary groove.
Stage E predominates in women less than 45 years of age with 12 patients, while in women over 45 years stage D predominates with 10 patients (Graph 2).
Graph 2: Distribution of patients according to degree of breast ptosis and age.
Table 2 shows the median and range of the resected tissue in the right and left breast according to age groups.
| Variable | Category | Less than 45Years | 45 Years or More | P | ||
|---|---|---|---|---|---|---|
| N | N | |||||
| R Resected tissue weight (g) | Median /IR | 20 | 400/350.0-465.0 | 15 | 350.0/350.0-400.0 | 0.215* |
| Range(Min-Max) | 300.0-650.0 | 300.0-550.0 | ||||
| L Resected tissue weight (g) | Median / IR | 20 | 410.0/365.0-530.0 | 15 | 370.0/350.0-400.0 | 0.159* |
| Range(Min-Max) | 300.0-750.0 | 300.0-650.0 |
Table 2: Resected breast tissue according to breast and age of the patients.
Tables 3 and 4 show the significant difference in preoperative and postoperative anthropometric measurements at 6 months and 1 year.
| Variable | Category | Preoperative | Postoperative | P1* | P2* | |
|---|---|---|---|---|---|---|
| 6 months | 1 Year | |||||
| NAC-Fork | R Breast | 25.0/23.0-25.0 | 21.0/20.0-22.0 | 21.0/20.0-21.0 | 0.000 | 0.317 |
| L Breast | 25.0/24.0-26.0 | 21.0/20.0-22.0 | 21.0/20.0-21.0 | 0.000 | 0.317 | |
| NAC Diameter | R Breast | 6.0/6.0-7.0 | 5.00 (ct) | 5.00 (ct) | 0.000 | 1.000 |
| L Breast | 6.0/6.0-7.0 | 5.00 (ct) | 5.00 (ct) | 0.000 | 1.000 | |
| NAC- Navel | R Breast | 19.0/18.0-20.0 | 21.0/21.0-22.0 | 21.0/21.0-22.0 | 0.000 | 1.000 |
| L Breast | 19.0/18.0-20.0 | 21.0/21.0-22.0 | 21.0/21.0-22.0 | 0.000 | 1.000 | |
| Intermamillary Distance (cm) | R Breast | 25.0/24.0-26.0 | 22.0/21.0-22.0 | 22.0/21.0-22.0 | 0.000 | 1.000 |
| Volume | R Breast | 950.0/870.0-1250.0 | 600.0/520.0-780.0 | 600.0/540.0-780.0 | 0.000 | 0.008 |
| L Breast | 950.0/880.0-1300.0 | 600/520.2-800.0 | 600.0/540.0-780.0 | 0.000 | 0.008 |
Table 3: Measurements related to the reduction of breast volume.
| Variable | Category | Preoperative | Postoperative | P1* | P2* | |
|---|---|---|---|---|---|---|
| 6month | 1Year | |||||
| RNAC | Median / IR | - | 3.0/3.0-4.0 | 3.0/3.0-4.0 | - | 0.317 |
| NAC-SG Distance | Median / IR | 21.0/18.0-23.0 | 5.0/5.0-6.0 | 5.4/5.0-6.0 | 0.000 | 0.066 |
Table 4: Measurements related to the correction of mammary ptosis.
Minor complications such as unaesthetic scar in 5.7%, wound dehiscence in 2.9% and alteration of the sensitivity of the NCA in 2.9%.
According to the surveys applied by the Breast-Q scale, more than 91% satisfaction is reached in all the aspects evaluated and only in a more than 68% (Graph 3).
As can be seen in Figure 1, there is a great difference between the preoperative anthropometric breast measurements and the 1-year postoperative evolution.− No changes are reported in postoperative anthropometric measurements at 6 months and 1 year, except for the increase in the distance from the submammary groove to the NAC, which is not statistically significant.
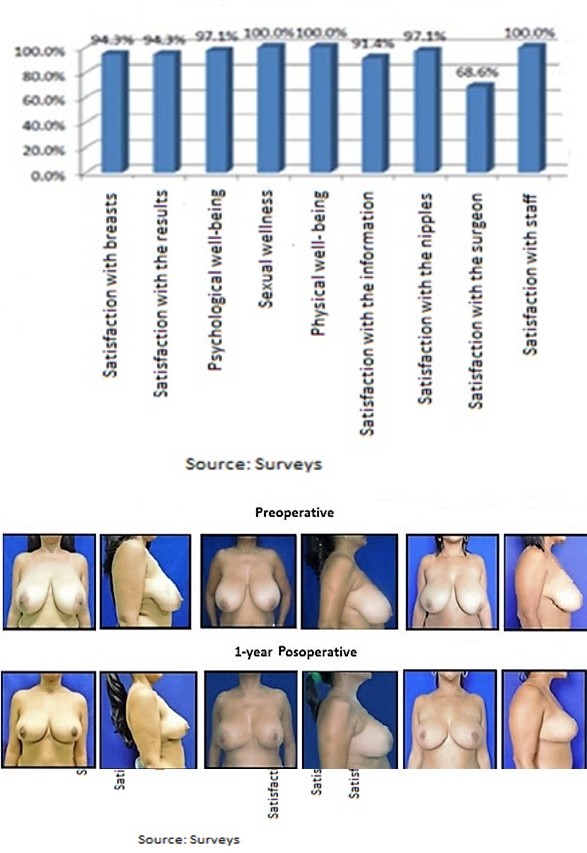
Graph 3: Breast-Q scale results.
Discussion
Breast hypertrophy is a frequent affectation in the female population. The ablation of the glandular surplus must respect the vascularization of the tissue and the remaining areolar plaque with the creation of a residual tissue mass that is flexible enough to be remodeled and sufficiently vascularized to avoid necrotic complications. When the predominant mammary surplus is located in the lower and external pole of the breast, the surgical proposal of choice for emptying or en bloc resection is the monopediculate Strombeck technique. Most of the operated patients are in their fourth decade of life and the most frequent reason for consultation is shoulder and back pain associated with the diagnosis of very important breast hypertrophy. The age group of patients that predominates and the mean age behaves similar to the 10-year study carried out by Güemes [11] that the mean is 38 years with a range of 15 to 56 and with that of Aldaz12 that is 44 years. These results are explained by the fact that younger women come to the clinic for surgical treatment, mainly when the hypertrophy is significant; while smaller volume hypertrophy persists longer and are a reason for consultation when breast ptosis predominates.
The magnitude of the resected weight was greater in the patients of the younger age group associated with larger breasts. However, the average of excised breast tissue is lower than that reported by Aldaz [12] with an average of 608 gr. Guemes [11] reports an average of 650 grams, with a range of 450 to 1500 grams, and the mean coincides with the upper limit of the range of resected tissue in this study. No disease was evidenced in the histological examination of the excised pieces, nor was surgical reoperations performed.
Breast dimensions vary with biotype, age, lactation, number of children, pregnancies, amount of parenchyma and fat, which is considered the most common factor for breast enlargement [13]. Anthropometric measurements of the breast at 6 months and 1 year of the Surgical intervention differ significantly from preoperative measures. This demonstrates volume reduction, correction of breast ptosis, macroareola, and breast divergence. Multiple studies use pre and postoperative measures as an objective for the evaluation of results. Of these, the most used is the distance from the sternal fork to the center of the nipple, as it is the one with the greatest scientific evidence in the literature [13]. In the 1-year postoperative evolution, no changes are observed in relation to the anthropometric measurements of the 6 months, except for the increase in the distance from the submammary groove to the NAC, which is not statistically significant.
The complications that are observed are infrequent and minor, such as: unsightly scar, wound dehiscence and alteration of the sensitivity of the NAC. Regarding the insensitivity of the NAC, it is only reported in one patient, although the disadvantage of this technique is that the percentage is large. Schlenz [7] carried out a study comparing 5 reduction mammoplasty techniques to evaluate which one most affected the sensitivity of the NAC and showed that this depends on the surgical technique used. Superior pedicle techniques, which require tissue resections at the base of the breast, are associated with an increased risk of injury to the nerve branches that innervate the NAC [12, 14].
Other studies report higher complication rates ranging from 19.1% Grajeda [14], 13.6% Bolger [15] and 50% Dabbah [16]. All agree that the most frequent early complications are hematoma, necrosis of the NAC and dehiscence of the wound of onset early; while the most common late complications are hypertrophic scars, loss of sensation, fat necrosis, dermoid cysts, and pseudoptosis. To prevent them, we insist on exhaustive hemostasis, not leaving the flaps under tension, adequate de-epithelialization, placement of drains, closure by planes so as not to leave the weight attached to the dermis, and posoperative dressings that allow monitoring the vitality of the NAC.
Stevens, et al. conducted one of the largest studies in terms of reduction mammoplasty results with a total of 884 surgeries [12]. They describe that possible minor complications include seroma, hematoma, soft tissue infection, dog ears requiring revision and small incisional injuries or delayed healing of less than 2 cm; whereas the major complications are due to incision problems or delayed healing of more than 2 cm, necrosis of the NAC, need for blood transfusion, deep vein thrombosis, pulmonary embolism, myocardial infarction and death.
The safety of mammoplasty surgery is evaluated by Ghareeb, et al. [17], who point out in their retrospective study in the period 2008-2014, that these surgeries performed with a careful technique are safe, effective and reliable.
The levels of satisfaction and quality of life are evaluated as high because the expectations of the patients are achieved. There are several instruments designed to evaluate the results obtained after breast surgery from the subjective evaluation of the patients themselves. The purpose of these questionnaires is to evaluate two predominant domains: patient satisfaction after breast surgery and quality of life in relation to her health [18, 19].
Among them is the Breast Reconstruction Satisfaction Questionnaire (Breast-Q), which is made up of several modules and scales that measure subjective results after breast surgery intervention [20, 21]. This instrument is useful in patients undergoing breast reconstruction due to cancer [18, 22, 23]. However, it is not used in cases of reduction mastoplasty, which prevents us from comparing our results. In the survey applied in the present investigation, the parameters of physical and sexual well-being reached 100% satisfaction, which responds to the improvement of the patients’ symptoms. Although the symptom complex that these women present is variegated and difficult to classify within the common pathology of a syndrome, the efficacy of breast reduction in relieving symptoms is indisputable [11]. Even if this relief was psychological or related to their body image reduction mastoplasty is helpful.
Breast hypertrophy or macromastia can cause a wide range of symptoms (physical, psychosomatic or behavioral) that affect the quality of life of patients. Breast reduction in most cases can solve the problem. However, there are factors that can have a negative effect on the outcome of the surgery. In a prospective and longitudinal study of 121 patients undergoing breast reduction performed by Perez [24] to assess the quality of life after reduction mammoplasty, an improvement in symptoms (p <0.001) and quality of life (p <0.001 for p = 0.002) were observed at month and one year after surgery, compared to the preoperative situation. One year after surgery, the majority of the patients (96.6%) were satisfied with the result, 96.6% would recommend it to others, and 95.8% would undergo a second operation if necessary. The effects of breast reduction on the quality of life of patients with macromastia were evaluated by Kececi [25, 26], which shows a significant improvement in the posoperative period in relation to self-esteem Rosenberg Self-Esteem Scale; P <0.001) and in all the domains of the Breast Reduction Assessed Severity Scale (BRASS) (P <0.001). Post-operatively, the 5 mean scores improved significantly, but the body pain score remained lower than that of a normative population. Valtonen [25] carried out a multicenter, prospective study that analyzed the symptoms related to the breast of 98 women, measured before the operation with the BRSQ scale (Breast Related Symptoms Questionnaire) and the Health Related Quality of Life (HRQL). The women were middle-aged (mean age 44 years) and most of them were overweight (body mass index at 29). All patients had frequent physical symptoms and disability due to their breast hypertrophy with a low score of symptoms reported by the severity of the breast (range 13-38). After the operation, symptoms associated with breast hypertrophy are considerably relieved in terms of discomfort, usual activities and breathing. All the aforementioned studies correspond to the results of the present investigation.
To date, it has been shown that there is no suitable technique for all types of breast, nor a specific technique that achieves the best aesthetic results and that can be applied to all types of patients. The most commonly used techniques during the 1960s were Strombeck, Biesenberger and Toreck [27, 28], for cases of macromastia and severe ptosis. Its selective use at present shows the validity of the use of horizontal and vertical dermal pedicles [29]. The high levels of satisfaction achieved in this study demonstrate the effectiveness of reduction mastoplasty techniques with medial pedicle.
Conclusions
The Reductive Mastoplasty with an internal monopediculate flap is a technique that offers good aesthetic results and few complications in patients with symptomatic breast hypertrophy.
References
-
Fonseca CC, Veiga DF, Garcia EDS, Cabral IV, de Carvalho MM, et al. (2018) Breast Hypertrophy, Reduction Mammaplasty and Body Image. Aesthetic Surgery Journal 38(9): 972-979.
-
Perez Panzano E, Gascon-Catalan A, Sousa-Dominguez R, Carrera Lasfuentes P, Garcia Campayo J, et al. (2017) Reduction mammaplasty improves levels of anxiety, depression and body image satisfaction in patients with symptomatic macromastia in the short and long term. Psychosom Obstet Gynaecol 38(4): 268-275.
-
Sharma K, Nigam S, Khurana N, Chaturvedi K (2004) Unilateral gestational macromastia--a rare disorder. Malays J Pathol 26(2): 125-128.
-
Calderon Ortega W, Lombardi Azocar JJ, Calderon D, Poblete Saavedra A, Camacho-Martino JP (2016) Periareolar reduction mammoplasty: anatomy and clinic of the central pedicle. Cir Plast Iberolatinoam 42(1): 21- 28.
-
Fisher J, Kent K (2013) Reduction mammoplasty history. In: Neligan PC (Ed.), Plast Reconstr Surg. Elsevier, USA, pp: 153-162.
-
Jimenez Reyes W, Rodriguez Gil E (2017) Reductive mastoplasty using the modified McKissock technique, with a small incision, L closure. Rev Inf Cient 96(3): 424- 434.
-
Bellini Ditta L (2018) Breast ptosis and its surgical resolution. Argentine Journal of Plastic Surgery 24(2): 95-104.
-
Kim MK, Kim T, Moon HG, Jin US, Kim K, et al. (2015) Effect of cosmetic outcome on quality of life after breast cancer surgery. Eur J Surg Oncol 41(3): 426-432.
-
McKevitt L. Kuusk U, Dingee C, Warburton R, Pao J, et al. (2019) Immediate Reconstruction Swing Room Scheduling Reduces Wait Times to Surgery and Increases Breast Reconstruction Rates. Annals of Surgical Oncology 26: 1276-1283.
-
Tamayo Carbon AM, Orozco Jaramillo MA, Rendon Oliva IE, Posada Ruiz DA, Valdivia Llanes J (2020) Outcomes of Reduction Mastoplasty by McKissock’s Modified Technique in Moderate Breast Hypertrophy. Rev Acta Med 21(1).
-
Guemes Sanchez A, Souza Dominguez R, Salinas Payer JC, Torcal Aznar J, Burdio Pinilla F, et al. (2000) Reduction mammaplasty. Indications and technical considerations. Cir Esp 68(1): 30-34.
-
Aldaz Lozada A (2016) Reduction mammoplasty in breast hypertrophy with use of an internal lateral flap attended at the Teodoro Maldonado Carbo Hospital during the period January 2013 - January 2015. Doctoral thesis. Samborondon.
-
De Barros Fernandez C (2012) Reductive L-shaped mastoplasty for large volumes. Autonomous University of Barcelona (AUB).
-
Grajeda Lopez P, Corzo Sosa A, Valdes Galicia J (1999) Reduction mammoplasty. Complications. Research work. Plastic surgery 9(1): 5-8.
-
Bolger WE, Seyfer AE, Stanley J (1987) Reduction Mammaplasty Using the Inferior Glandular “Pyramid” Pedicle Experiences with 300 Patients. Plastic and Reconstructive Surgery 80(1): 75-84.
-
Dabbah A, Lehman JA, Parker MG, Tantri D, Wagner DS (1995) Reduction mammaplasty: an outcome analysis. Ann Plast Surg 35(4): 337-341.
-
Allue Cabanuz M, Arribas del Amo M, Guemes Sanchez A (2020) Risk reducing mastectomy: reflections and evidences. Author’s reply. Journal of Senology and Breast Pathology - Journal of Breast Science 33(3): 127-128.
-
Sanchez WalsJuan L, Lence J, Villegas Valverde C (2020) Satisfaction with the aesthetic results of post-mastectomy breast reconstruction at the Cuban Institute of Oncology (INOR) by using the BREAST-Q questionnaire. Revista de Senología y Patología Mamaria.
-
Jara R, Albornoz C, Valdes M, Andrades P, Erazo C, et al. (2020) Translation and cross-cultural adaptation into Spanish (Castilian) of the Breast-Q instrument, breast reconstruction module. Rev Cir 72(2): 126-129.
-
Mundy L, Homa K, Klassen A, Pusic A, Kerrigan C (2017) Breast Cancer and Reconstruction: Normative Data for Interpreting the BREAST-Q. Plast Reconstr Surg 139(5): 1046-1055.
-
Begic A, Stark B (2016) The Telemark Breast Score: A Reliable Method for the Evaluation of Results after Breast Surgery. Plast Reconstr Surg 138(3): 390-400.
-
Cha R, Barnes E, Locke M (2013) Patient-reported outcomes following breast reconstruction surgery in a public hospital: use of the Breast-Q questionnaire. N Z Med 126(1386): 43-55.
-
Toyserkani NM, Jørgensen MG, Tabatabaeifar S, Damsgaard T, Ahm Sørensen J (2020) Autologous versus implant-based breast reconstruction: A systematic review and meta-analysis of Breast-Q patient-reported outcomes. J Plast Reconstr Aesthet Surg 73(2): 278-285.
-
Perez Hera F, Castillo Calderon G, Rivera Companioni L, Pina Morales E (2012) Breast reduction surgery with infiltrative local anesthesia. Electronic Med Rev of Ciego de 18(1).
-
Kececi Y, Sir E, Gungor M (2015) Patient-reported quality-of-life outcomes of breast reduction evaluated with generic questionnaires and the breast reduction assessed severity scale. Aesthet Surg J 35(1): 48-54.
-
Danilla S, Troncoso E, Ríos M, Dominguez C (2016) What factors influence the satisfaction of patients undergoing breast reduction? Analysis of a cohort study using the Breast-Q instrument. Rev Chil Cir 69(1).
-
Jimenez Reyes M, Jimenez Reyes W, Rodriguez Gil E (2018) Reductive mastoplasty by modified Thorek technique in giant breasts. 97(1).
-
Avellaneda Oviedo M, Garcia Novoa A, Palacios Garcia P, Pacheco Compana J, Acea Nebril B, et al.(2019) Reductive risk surgery with prosthetic reconstruction by using type IV skin sparrow mastectomy with free nipple- areola graft. Cir Plast Iberolatinoam 45(2): 139-150.
-
Mangelsdorff G, Deichler FV, Garcia Huidobro MA, Enriquez E, Israel G, et al. (2013) Validation of an instrument to assess quality of life associated with breast hypertrophy in Chilean women. Rev Med Chile 141(9): 1143-1149.
- Reconstruction of Nasal Defect Using a Local Flap Based in the Nanoperforants Concept: A Case Report
- Transplant Tourism in Japan: Insights from Nationwide Surveys and Emerging Ethical Challenges
- The Challenge of Peritoneal Vaginoplasty in Transgender Women: Review Literature and Personal Perspectives
- Algorithmic Paternalism: Autonomy Versus Automation
- Dermatoscopy in Gorlin Syndrome: Avoiding the Disfigurement in Patients
- How Artificial Intelligence is Ushering in a New Era of Innovation in General and Plastic Surgery: A Short Communication