Comprehensive Surgical Treatment of Breast Cancer by Minimally Invasive Surgery
Introduction
Breast cancer surgery undergoes important modifications due to technological advances and knowledge of tumor biology. Oncospecific locoregional treatment is the cornerstone, but varies by staging. Oncological surgical strategies include prophylactic, diagnostic, conservative, mastectomy, and oncoplastic surgery. All include excision of the tumor and / or breast tissue and glandular reconstruction to achieve a good cosmesis. For two decades, breast oncoplastic surgery has been described. This allows the aesthetic restitution of the posmastectomy breast and in conservative surgery. In addition, it corrects the sequelae of other treatments and includes various surgical techniques such as: mammoplasty, strumoplasties, breast reconstructions and prophylactic surgery. Its two fundamental pillars are the restitution of corporal and aesthetic integrity, as well as the reduction of the risk of Breast Cancer (BC) [1].
Breast reconstruction is a surgical challenge due to two fundamental aspects: the choice of the appropriate technique for each patient and the remodeling of the flap to obtain the most natural breast possible [2]. In the last five years, due to the considerable increase in the worldwide incidence of BC and scientific-technical development, new surgical techniques have been introduced for its prophylactic and / or curative treatment with immediate reconstruction [3, 4]. In Cuba, breast reconstruction began at the Hermanos Ameijeiras Hospital in the 1980s using pedicle flaps and in 1998 at the National Institute of Oncology and Radiobiology. Currently, numerous oncoplastic surgery techniques are described with satisfactory aesthetic results, among which the following stand out: conservative surgery of the areola- nipple complex, skin-sparing surgery and techniques with perforating flaps [3].
A booming variant of mastectomy techniques is the skin saver. The surgical technique consists of the removal of all breast tissue, preserving the skin with or without the Areola- Nipple Complex (ANC). Reconstruction can be performed immediately in the same surgical act or delayed in a second surgical time. Its only initial indication was for the treatment of benign breast lesions. However, due to the high worldwide incidence of BC, its use has been extended to risk-reducing surgery and the already established BC. Hence, in the search to improve surgical options, numerous incisions and increasingly less invasive procedures have been described that increase the quality of life of patients with BC [4, 5].
Knowledge of oncological surgical principles allows the implementation of new minimally invasive surgical techniques for BC [5, 6]. Its purpose is to reduce surgical aggression and scars in visible areas of the breast, preserve its external contour as natural as possible, reduce pain, reduce surgical risk; as well as the expenses of the National Health System and of the patient to accelerate the recovery and reincorporation to the usual activity of her. In addition, it allows large surgeries to be performed through small incisions and combined with high-tech procedures such as laparoscopic and robotic surgery [7, 8]. Minimally invasive surgical techniques have been extended to all fields of surgery to reduce the effects of surgical trauma and its consequences. It is estimated that in the immediate future the experience of surgical teams and technological access will increase to increase the number of surgical interventions using these techniques. The special characteristics of breast cancer surgery make it one of the most benefited by performing the surgical approach through low visibility accesses [7]. This is a new concept in the comprehensive surgical treatment of BC that allows oncological resections and reconstructions through incisions that are imperceptible to the patient’s vision or to the perception of others, with an oncological safety identical to the conventional procedure.
Due to all the above, this research is carried out with the aim of presenting a technical modification through the low visibility surgical approach of the Skin-Sparing Modified Radical Mastectomy with preservation of the NAC and immediate reconstruction with retropectoral silicone cohesive gel breast implants by Minimally Invasive Surgery through a single periareolar incision.
Methods
We present three young patients with left BC operated on for Skin-Sparing Left Modified Radical Mastectomy with preservation of the NAC and immediate reconstruction with placement of retropectoral mid-profile cohesive silicone gel implants by Minimally Invasive Surgery through a single periareolar incision.
Inclusion criteria:
- Ages over 18 and up to 60 years of age.
- Patients diagnosed with breast cancer.
- Patients with breasts with volumes from 200 cc to 300 cc.
- Absence of breast ptosis.
- Size of the areola greater than 4 cm in diameter.
- Breast / tumor relationship that contraindicates conservative surgery.
- Patients with multicentric tumors and extensive pathological-looking microcalcifications.
- Patients without retraction of the skin or the areola- nipple complex.
- Patients who received neoadjuvant treatment or not with polychemotherapy who had a complete or partial clinical response.
- Satisfied parity.
- Patients who signed the informed consent for surgery.
Exclusion criteria:
- Patients who cannot attend routine posoperative follow- up.
- Paget’s disease with another breast lesion.
- Inflammatory carcinoma of the breast at the time of diagnosis or surgery.
- Smoking patients.
- Pregnant or nursing.
- Previous treatments with anticoagulants and breast filler injections.
- Patients with a personal pathological history of Coagulopathies.
- Bodybuilders.
- Presence of active local, skin or systemic infections.
Preoperative Measures
Paraclinical exams: Hemogram and hemochemistry within normal limits. PCR for Covid - 19 negative, breast ultrasound, mammography and expiratory fine needle cytology or core needle biopsy (trucut). Immediate preoperative period: Assessment by the specialties of Anesthesiology, General Surgery and Plastic Surgery. Preoperative surgical risk assessment and surgical procedure planning. ERAS protocols: All perioperative improved recovery measures were applied for breast cancer surgery following international standards [9]:
- Preoperative education of patients.
- No bowel preparation.
- Ingestion of 400 ml of preoperative carbohydrate solution up to 2 hours before surgery (clear juices without residues, tea or coffee).
- Antithrombotic prophylaxis with low molecular weight heparin (Nadroparin or Enoxiparin 0.6 ml SC) in the immediate preoperative period according to the risk of thromboembolic disease.
- Antibiotic prophylaxis (Cefazolin 1gr EV 30 minutes before surgery and 2 more doses in the immediate postoperative period).
- Balanced intravenous hydration (≤ 1000 ml of fluids in the immediate postoperative period and <150 mmol of sodium).
- Do not place posoperative levine catheter.
- Use of negative suction drains> 24 hours; the patient is discharged in 24 to 48 hours and is removed in the outpatient clinic.
- Application of standard anesthesia according to protocol.
- Multimodal analgesia, avoiding opioids (Diclofenac
75mg EV every 12 hours and then orally when possible Dipyrone 500mg or Paracetamol 500mg every 8 hours). 11. Prevention of posoperative nausea and vomiting (Liquid diet at 6 hours and early mobilization. The use of Ondansetron 8 mg EV or Metoclopramide 10 mg EV) may be necessary. 12. Posoperative oxygen therapy (O2 4 to 6 L / min by mask or nasal catheter). 13. Early restart of the oral route, 4 to 6 hours after surgery (with oral nutritional supplements on the first posoperative day and on the second day start the usual hospital diet). 14. No use of urinary catheter. 15. Extensive mobilization on the first postoperative day (sitting out of bed for at least 4 hours and walking).
Surgical Technique
Patient in supine position, both arms abducted at 90˚, supported by arm boards and secured with gauze. Under general orotracheal anesthesia, the operative field is prepared by asepsis and antisepsis of the mammary and left axillary region and sterile surgical fields are placed. It begins with the periareolar incision of 5 cm from H12 to H6 in the shape of a semicircle surrounding the external edge of the areola, opening by planes, eversion of the NAC and a wedge biopsy of the retroareolar region that is sent to pathological anatomy for ensure the absence of tumor at the edge of the surgical section, respecting 1 cm of tissue close to the areola skin to guarantee vascularization of the areola- nipple complex. Tumor excision and freezing biopsy are then performed to confirm the histological diagnosis of BC if the patient was studied only by preoperative cytology (not necessary if there is a preoperative histological diagnosis of BC), before proceeding to the mastectomy.
The Skin Sparing Mastectomy is performed by elevating the skin flaps above the enveloping fascia of the breast with Farabeuf spacers. The thickness of the skin flap is approximately 5 to 10 mm, although it depends on the location of the tumor in the breast and the patient’s body habit. The flaps are carefully dissected with electrocautery or scissors and the skin is pulled centripetally with fine Deaver retractors to expose the surgical field. The upper flap should be brought to the second intercostal space, the lower to the upper edge of the rectus abdominis muscle, the medial to the sternal edge, and the lateral to the anterior axillary line. All are dissected following the plane of Cooper’s ligaments. All breast tissue is resected, including the aponeurosis of the pectoralis major muscle up to its axillary edge, dissecting parallel to the muscle fibers. The mastectomy is completed preserving the entire skin envelope including the areola- nipple complex. The surgeons’ gloves are changed and all the instruments used for tumor resection are discarded.
The axillary approach is performed by traction of the flaps with fine Deaver retractors and an oblique incision of the clavipectoral fascia is made. The axillary region is exposed with electrocautery and / or scissors from the surface to the depth, looking for the emergence of the axillary vein, the axillary fat and lymph nodes are dissected, ligating the tributaries of the axillary vein coming from the thoracic wall and preserving the intercostobrachial nerves whenever possible. Therefore, axillary lymph node dissection has the axillary vein as its upper limit, the lateral border of the pectoralis major muscle medially, and the latissimus dorsi muscle at the rear. Hence, Berg’s level I, II, and III axillary lymphadenectomy is performed starting from top to bottom and working from the inside out. The mammary gland and lymph nodes are then en bloc removed.
Breast reconstruction begins with the dissection of the lower border of the pectoralis major muscle, a flap from the rectus abdominis muscle and another from the serratus muscle to create a pocket for the breast implant. The mid- profile silicone breast implant is placed in the created pocket and the muscle planes are closed with non-absorbable points that guarantee total muscle coverage. Thorough hemostasis is performed, placement of a negative suction drain (Hemovac) from the axillary region to the submammary groove. Close by planes up to the skin.
Post-operative Care
- Dry cure of the surgical wound with alcohol every other day.
- Drain removal after 48 hours.
- Health education on stabilizing band, surgical adjuster and prosthetic massage.
- Left arm care: No physical effort, limitation of movement and strength of the left upper limb.
Aesthetic results: They were evaluated according to the following criteria:
- Areola-nipple complex in proper position.
- Symmetry in the shape and position of the breasts.
- Resection of the tumor with free margins.
- Absence of complications.
- Little visible scar. a) Good: When all criteria are met. b) Regular: When 4 or 3 of the criteria are met. c) Bad: When less than 2 of the criteria are met.
Degree of satisfaction: The Breast-Related Symptoms Questionnaire (BREAST-Q) [10] was applied as a theoretical basis, since it is the most widely used international instrument to measure patient self-satisfaction with breast surgery. Some modifications were made according to the surgical procedure used and the results obtained [11].
The instrument was applied with modifications 3 months after the patients had been operated on. Questions specific to the abdomen, nipple reconstruction and those related to medical care were eliminated. Thus, the questionnaire was made up of five main modules (Annex 1):
- Satisfaction with the appearance of their breasts.
- Satisfaction with the implant.
- Satisfaction with the surgery.
- Emotional satisfaction.
- Satisfaction with sexuality.
Each module has different questions and a scale of 40 questions was made with 3 possible scores where (3 = 2.5%, 2 = 1.66% and 1 = 0.83%) to achieve 100%, which will be the highest degree of patient satisfaction. From the score obtained, the degree of satisfaction of the patients was considered in: a) Excellent: It was considered when a score greater than 90% was obtained. b) Good: It was considered when a score of 85% to 90% was obtained. c) Regular: It was considered when a score lower than 85% was obtained. Complications: Present or absent. a) Minor: Local complication that requires medical treatment. b) Major: The one that requires a surgical reintervention.
The research was approved by the two participating services, the Scientific Council and the Institution’s Medical Ethics Commission. It was carried out in accordance with the principles of current national and institutional medical ethics and the Declaration of Helsinki.
Results
The periareolar approach of a Skin-Sparing Left Modified Radical Mastectomy with Preservation of the NAC was performed in three patients aged between 30 and 34 years with a health history, without toxic habits, with a family history of BC, ovarian and / or prostate with diagnosis of BC that presented tumors between 2 and 4 cm without skin retraction or involvement of the nipple areola complex. Two of them received neoadjuvant treatment with polychemotherapy and presented a partial clinical response. Patients with small breasts and without breast ptosis were selected, so they did not need any additional procedure in the contralateral breast to achieve symmetry. The diameter of the areolas varied between 4 and 6 cm. Silimed medium profile silicone cohesive gel textured retropectoral breast prostheses were placed with volumes between 150 and 280 cc in an average surgical time of 3 hours. ERAS protocols were applied in all cases, which made it possible to accelerate recovery and reduce costs.
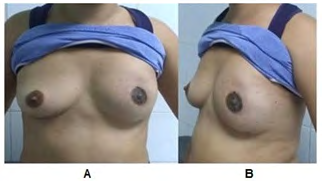
The aesthetic results achieved were good in all patients with a high degree of satisfaction with surgery with 90.76%, 92.45% and 95% respectively, according to the international BREAST-Q questionnaire (Figures 1-3).

Within the first month in the second operated patient, skin folds appeared that disappeared spontaneously.

No patient presented minor or major complications.
Discussion
Every year, BC affects the lives of millions of increasingly young women with high mortality. According to the Statistical Yearbook of the Ministry of Public Health, [12] 2.1 million new cases are diagnosed annually in the world and in Cuba it is the second cause of death for women due to malignant tumors, despite 75% being diagnosed in early stages due to the BC early detection program.
In recent years there has been a worldwide trend towards an increase in BC in increasingly younger women, which represents approximately 23% of cases [13]. In these patients the prognosis is worse due to the presentation of a more aggressive histology (high degree of anaplasia, Her2 overexpression, high rate of positive lymph nodes), late diagnoses and higher recurrence rates.
In the three patients presented, an innovative surgical technique is performed that allows comprehensive surgical treatment of BC by Minimally Invasive Surgery through a single periareolar access. The incision that was used is approximately 5 cm in length and allows total breast excision with tumor-free surgical section edges, axillary emptying, and placement of retropectoral breast prosthesis through the same incision.
At present, multiple surgical techniques for the comprehensive treatment of BC have been described worldwide [1, 2, 3, 4, 5, 9, 12, 14, 15]. The fundamental purpose of improving surgical techniques is to reduce trauma, guaranteeing oncological safety to avoid recurrences and unwanted scars; thus providing better visual acceptance of the patient.
The Skin-Sparing Mastectomy with preservation of the NAC is a technique currently on the rise. It arose for the treatment of benign breast lesions; but with the high worldwide incidence of BC, it is also used in risk-reducing surgery and BC [4, 5]. In this perspective, numerous technical modifications are described for the Minimally Invasive Surgical approach through low visibility accesses in breast cancer surgery, such as the videolaparoscopic approach with the use of flaps, which shows greater satisfaction in relation to scars and reduction of the postoperative complications; although it requires longer surgical time and training in laparoscopic surgery [8].
Skin-Sparing Mastectomy or subcutaneous mastectomy can be combined with oncoplastic techniques for the comprehensive surgical treatment of BC [16, 17]. The selection of the surgical technique and the preservation or not of the NAC depends on the anatomical characteristics of the breasts, the size of the tumor, its location, the involvement of the skin and the tumor involvement of the NAC. Numerous incisions for Skin-Sparing Mastectomy are described, among which the following stand out: the Round- block type periareolar incision, the upper outer racket incision, lower pedicle mammoplasty - upper central, omega -central mammoplasty, lateral-upper external mammoplasty, medial mammoplasty - upper lower, J plasty - lower outer, vertical mammoplasty - lower inner, L plasty - lower outer, lower breast fold mammoplasty - lower central Inverted T mammoplasty - central).
The classic approaches for breast implant placement [18] include perioareolar, submammary, and axillary to achieve less visible scars and a good cosmetic result. The advantages of the periareolar approach are due to the fact that, as the areola is a looser tissue, it allows greater exposure of the surgical field, with an inconspicuous scar and a low tendency to keloid. This anatomical condition makes it a site of choice for low visibility breast incisions, even in the cases of patients with a keloid tendency as in the second patient presented who had keloids in the presternal region and even so it was decided to perform the periareolar incision obtaining good aesthetic results. However, its disadvantage is the increased risk of Staphylococcal epidermidis infections because it is very close to the milk ducts and there is communication with the outside. The literature Bright CJ, et al. [19] suggests that the most frequent location of mammary tumors is in the upper quadrants with 70%, with a predominance of the upper external quadrant with 50%. For this reason, the most commonly used incisions are periareolar with or without axillary extension or oblique incision, although the selection of the incision depends on the type of breast, the breast / tumor relationship and the location of the tumor. In the present study of technological innovation, a Minimally Invasive Surgery was performed through a single periareolar incision that allowed performing a mastectomy, axillary emptying and immediate reconstruction with a retropectoral implant, obtaining good oncological and aesthetic results.
ERAS protocols or also called “Surgical Multimodal Rehabilitation Programs” applied in breast surgery safely improve posoperative recovery of patients. The current scientific evidence of several key actions of posoperative recovery has been incorporated into medical practice to guarantee early recovery, reduce hospital stay, costs and the rate of complications [9].
In the three cases presented, good cosmetic results are reported, a high degree of satisfaction according to the international Breast Q scale and the absence of complications, similar to the literature consulted [10, 11]. This result agrees with the literature consulted, [4, 16, 17] which reports a low incidence of complications with similar surgical techniques.
However, when they occur, minor complications such as exposure of the suture, delayed healing and epidermolysis predominate, depending on the incisions and the type of mastectomy performed. These complications resolve spontaneously or require medical treatment, as opposed to major complications that require surgical treatment. The most frequent major complications reported are implant extrusion, capsular contracture, skin necrosis, infection, hematoma and seroma, with an incidence of 2% in each of them [16, 17].
Successful surgical treatment consists of performing a refined surgical technique; as well as early diagnosis and timely treatment of complications.
Comments
Although the priority of cancer patients is to live, the improvement and implementation of new surgical techniques to improve the cosmetic result and improve the quality of life of patients constitute real challenges for mastologist surgeons.
Conclusion
Minimally Invasive Surgery with single periareolar access is safe and effective for Skin-Sparing Modified Radical Mastectomy with preservation of the nipple areola complex, as well as the armpit approach and immediate reconstruction with the placement of retropectoral breast implants.
Recommendations: Include all women in the Breast Cancer Early Detection Program to perform more conservative surgeries; as well as immediate reconstructions in patients who meet the selection criteria.
Limitations of the Study: During the follow-up time (1 year), no patient presented capsular contracture, local or distant recurrence, but to effectively assess the presence of BC recurrences, at least 5 years after surgery are needed.
References
-
Albadalejo VC (2016) Breast cancer surgery. Treatment surgical techniques and reconstruction, recovery time and time. Med Segur Trab 62: 116-124.
-
Cruz Benitez L, Morales Hernandez E (2014) History and current status of the types of surgical procedures performed in breast cancer. Gac mex oncol 13(2): 124- 133.
-
Sanchez L, Alfonso L, Sanchez I, Ramos M, Ropero R (2020) Immediate breast reconstruction the National Institute of Oncology and Radiology of Cuba. Rev Cub Cir 59(4).
-
Alarcon Iranzo M, Buch Villa E, Ibanez Arias A, Zorraquillo E, Ramirez Sabio J, et al. (2018) Skin-sparing mastectomy and nipple-areola complex with immediate reconstruction: a growing technique in the treatment of breast cancer. Rev Senol Patol Mamar 31(3): 94-101.
-
Carlson GW, Bostwick J, Styblo TM, Moore B, Bried JT, et al. (1997) Skin-sparing mastectomy. Oncologic and reconstructive considerations. Ann Surg 225(5): 570- 575.
-
Soler Vaillant R, Mederos Curbelo ON (2018) Surgery. Havana (Eds.), Ecimed, Chapters: 8-9, Vol 1.
-
Guemes A, Sousa R, Cachon R, Valcarreres P, Rufas M, et al. (2008) Minimally invasive breast surgery: breast reconstruction using a pure muscle flap of the great dorsalis. Cir Esp 83(2): 85-88.
-
Houvenaeghel G, El Hajj H, Schmitt A, Cohen M, Rua S, et al. (2020) Robotic-assisted skin sparing mastectomy and immediate reconstruction using latissimus dorsi flap a new effective and safe technique: A comparative study. Surg Oncol 35: 406-411.
-
Temple Oberle C, Shea Budgell MA, Tan M, Semple JL, Schrag Ch, et al. (2017) Consensus Review of Optimal Perioperative Care in Breast Reconstruction: Enhanced Recovery after Surgery (ERAS) Society Recommendations. Plast Reconstr Surg 139(5): 1056- 1071.
-
Jara R, Albornoz C, Valdes M, Andrades P, Erazo C, et al. (2020) Translation and cross-cultural adaptation into Spanish (Castilian) of the Breast Q ® instrument, breast reconstruction module. Rev Cir 72(2): 126-129.
-
Payne RM, Siotos C, Manahan MA, Rosson GD, Cooney CM (2018) Breast cancer and reconstruction: Normative data for interpreting the BREAST-Q. Plast Reconstr Surg 141(1): 180-181.
-
Statistical Yearbook of Health 2019.
-
Stover ACL, Viamontes NM, Fernandez JLL, Vila Garcia E (2018) Results of surgical treatment of breast cancer in women up to 40 years of age. Rev Cub Cir 57(2).
-
Tamayo Carbon AM, Vila Garcia E, Cedillo Lopez RM (2019) Postmastectomy Mammary Reconstruction with Musculocutaneous Flap of Latissimus Dorsi and Placement of Definitive Endoprosthesis. Int J Transplant & Plastic Surg 3(1): 000130.
-
Potter S, Trickey A, Rattay T, O Connell RL, Dave R, et al. (2020) Therapeutic mammaplasty is a safe and effective alternative to mastectomy with or without immediate breast reconstruction. Br J Surg 107(7): 832-844.
-
Nahabedian M, Neligan P (2021) Plastic Surgery. Chapter 13, 4th (Edn.), Washington DC, USA, MedStar Georgetown University Hospital: Elsevier, Vol 5.
-
Nahabedian M, Neligan P, Plastic Surgery. Chapter 16, 4th (Edn.), Washington DC, USA, MedStar Georgetown University Hospital: Elsevier.
-
Castillo Delgado P, Prado Scott A, Troncoso Rigotti A, Villaman Gonzalez J, Fuentes Freire P (2007) Areolar approach in mammoplasty. Cir Plast Iberoatinoam 33(2): 91-96.
-
Bright CJ, Rea DW, Francis A, Feltbower RG (2016) Comparison of quadrant-specific breast cancer incidence trends in the United States and England between 1975 and 2013. Cancer Epidemiol 44: 186-194.
- Reconstruction of Nasal Defect Using a Local Flap Based in the Nanoperforants Concept: A Case Report
- Transplant Tourism in Japan: Insights from Nationwide Surveys and Emerging Ethical Challenges
- The Challenge of Peritoneal Vaginoplasty in Transgender Women: Review Literature and Personal Perspectives
- Algorithmic Paternalism: Autonomy Versus Automation
- Dermatoscopy in Gorlin Syndrome: Avoiding the Disfigurement in Patients
- How Artificial Intelligence is Ushering in a New Era of Innovation in General and Plastic Surgery: A Short Communication