Post-Liver Transplantation Diabetes Mellitus: Concise Literature Review and Own Experience
The collective accomplishments of the liver transplant community have resulted in satisfactory 5- and 10-year patient and graft survival. Within the increasing cohort of transplant recipients, metabolic complications are becoming a main reason for non-graft related mortality. Post-liver transplantation diabetes mellitus (PLTDM) is a well-documented disorder, adversely affecting recipient survival, a main risk factor for cardiovascular disease (CVD) and CVD-related mortality. The incidence of PLTDM varies between 9-63%. Calcineurin inhibitors (CINs) and corticosteroids are the principal mediators in the pathogenesis of this disease. We performed a brief review of the literature and retrospectively analyzed our own experience. For immunosuppression we use standard protocol of corticosteroids, tacrolimus and mycophenolate mofetil. The frequency of PLTDM in our series is 20%. We did not find a connection between recipient age, BMI, lipid status, underlying liver disease or acute rejection episode with the development of sustained PLTDM.
Introduction
Liver transplantation is currently a routine procedure, performed in many specialized centers across the world. The surgical technique and immunosuppressive therapy have evolved, as have the intensive care and infection control. Currently the 5-year patient survival, based on Organ Procurement and Transplantation Network data is 75.5% [1] and according to the European Liver Transplant Registry (ELTR), the 5- and 10-year survival rates are 71 % and 61% respectively [2]. Moreover, the advancement of the anti-viral therapy, with the introduction of the direct-acting antiviral agents, targeted against HCV, has led to the reduction of disease recurrence in the grafted liver [3, 4, 5]. Nevertheless, these survival rates have changed insignificantly for the past decade. This plateau signifies a rise of metabolic disorders, leading to an increase of the non-graft related mortality [6]. This turn of events in the past years has understandably shifted the focus to post-LT follow-up and medical care. At the present time, cardio-vascular disease (CVD) is one of the main causes of mortality among liver-transplant patients [6, 7]. Diabetes mellitus (DM) has been recognized as a major risk factor for CVD [6]. According to data from the World Health Organization (WHO), about 422 million people in the world are affected by DM. In 2012 more than 3.7 million deaths were directly related to this condition [8]. Post liver- transplantation diabetes mellitus (PLTDM) is one of the most common metabolic complications [9]. In addition to the well- known adverse effects of DM, it is associated with increased risk of graft loss, acute rejection and worsened patient survival [9].
Methods
For the purpose of this review, we performed a retrospective analysis our liver transplant database. Since the start of our liver-transplant program, for the period of April 2007 - December 2021, 80 liver transplants have been performed, including 2 living – donor liver transplants and 1 re-transplantation. The study includes 63 men and 17 women aged 14-57 years (mean age 42.85 years). Several factors were evaluated: the serum glucose - minimum, maximum and average value within the first 14 postoperative days, on the first, sixth and twelfth postoperative month, the total dose of the applied short-acting insulin (UI), corticosteroid (methylprednisolone, mg, prednisone, mg), mycophenolate mofetil (mg), tacrolimus (mg), serum level of tacrolimus. We examined the dependence of developing post-transplant diabetes mellitus on gender, age, body mass index (BMI), lipid profile, etiology of liver failure, the presence of hepatitis C virus (HCV) and cytomegalovirus (CMV) infection. The onset of impaired carbohydrate tolerance, new onset post- transplant diabetes mellitus (according to diagnostic criteria of the World Health Association) and the dependence on the use of immunosuppressive therapy are recorded. A standard protocol for immunosuppressive therapy has been used:
- Methylprednisolone - Day 1: 5 mg / kg; Day 2 - 2.5 mg / kg; Starting on Day 3 – a gradual reduction in dose to reach the support level of 5-20 mg / day.
- Tacrolimus - 0, 1 mg/kg/24h. With systemic drug monitoring therapeutic levels are reached - 10-15 ng / ml by the end of the first month; 7-15 ng / ml by the end of the third month.
- Mycophenolate mofetil - 1000 mg / day included on the seventh day (on demand).
Results
From a total of 80 liver transplant patients, 14 were diagnosed with DM preoperatively and were excluded from the analysis. Of the remaining 66 patients, 10 were censured due to early post-transplant mortality or early biliary complications, requiring prolonged ICU and hospital stay. A total of 56 patients were included in the analysis. An onset of PLTDM was registered in 25% of patients (n=14). In all the cases, patients were discharged with subcutaneous basal/ bolus insulin regimen. No remission to normoglycemic state has been documented, for a median follow-up of 76 months. Another 5 patients (9%) were diagnosed as having increased fasting plasma glucose levels (IFG) but were successfully managed with lifestyle change and diet.
In the immediate postoperative period, all recipients were intensively monitored, with strict control of plasma glucose levels. Transient hyperglycemia, requiring insulin administration within the first two weeks after LT, was documented in 47 out of 56 patients (84%). Once oral food intake was resumed, a basal/bolus insulin administration scheme was prescribed with day-to-day dose adjustment. With the reduction of the corticosteroid dose, the glucose values in most of the patients normalized.
Of the patients, who developed PLTDM 8 were male (72%). The indication for liver transplantation was alcoholic liver disease in 6 patients, primary biliary cirrhosis in 1 patient, primary sclerosing cholangitis – 2 patients, HCV – 1 patient, HBV/HDV – 1 patient.
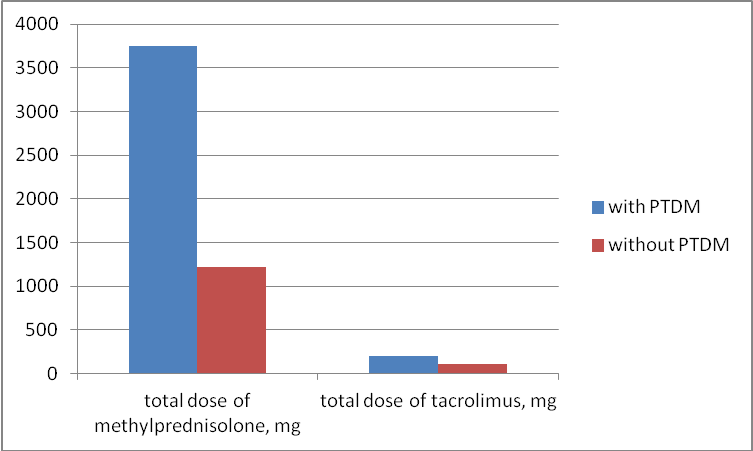
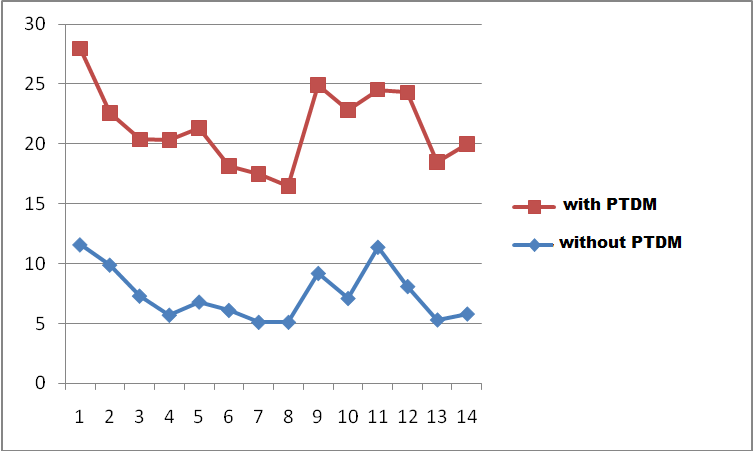
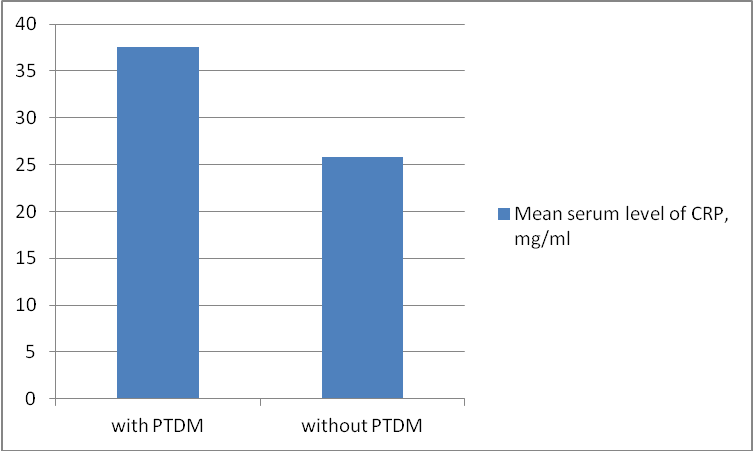
Overall, patients with PLTDM received higher doses (in absolute values) of immunosuppressive agents, which may be attributed to the higher BMI of the group (Figure 1). The mean blood glucose levels were statistically higher (p <0.05) than those in patients with transient impaired glucose tolerance (Figure2). They required higher doses of fast-acting insulin in order an adequate glycemic control to be achieved. The subgroup analysis showed no significant connection between PLTDM and HCV or CMV infection, preoperative lipid status or presence of hypertension. There was no statistically significant increase in acute graft rejections in patients with PTDM or other complications associated with the graft. Elevated values of cholesterol, triglycerides, CRP, as well as higher blood pressure postoperatively were registered in this group (Figure 3).
It should be noted that recipients with pre-LT DM needed increased doses of insulin and with some, glycemic control was hard to obtain, requiring in some cases continuous i.v. insulin infusion. Of the 14 patients with pre-existing diabetes, 4 suffered severe post-LT complications, leading to early mortality – 1 patient suffered from intracranial hemorrhage, 1 – early hepatic artery thrombosis, followed by ARDS, sepsis and multi-organ failure, 1 patient had early biliary complications, leading to sepsis and death and 1 patient suffered from early HCV recurrence, developing
fulminant fibro-lamellar hepatitis. In our series, no significant difference in the 6-months post-LT mortality has been found between patients without DM and patients with pre-LT DM, p=0.212.
Discussion
Post – liver transplantation diabetes mellitus (PLTDM) is one of the most common metabolic complications. It is defined as elevation of plasma glucose levels, compliant with the World Health Organization (WHO) [10] or the American Diabetic Association (ADA) criteria [11] (Tables 1& 2), in a patient, who has endured liver transplantation.
| Group | PLTDM¶ |
|---|---|
| Number | 8 |
| Age, mean, years | 43 (32-51) |
| Gender | |
| female | 2 |
| Male | 6 |
| Body mass index (BMI) | 32.56 (30.2-34.9) |
| Cause for transplantation | |
| Alcoholic cirrhosis | 4 |
| Hepatitis В/Hepatitis D | 1 |
| Hepatitis С | 1 |
| Primary biliary cirrhosis | 1 |
| Primary sclerosing cholangitis | 1 |
| Preoperative serum level of cholesterol, mean, mmol/l | 3.785 |
| Preoperative serum level of triglycerides, mean, mmol/l | 0.835 |
Table 1: Demographic and patient characteristics of the liver-transplant recipients with post-liver transplantation diabetes mell
| Condition | 2h – post OGTT | Fasting glucose | HbA1c | |
|---|---|---|---|---|
| Units | mmol/l (mg/dL) | mmol/l (mg/dL) | mmol/mol | DCCT% |
| Normal | < 7.8 (< 140) | < 6.1 (< 110) | < 42 | < 6.0 |
| Increased fasting glucose | < 7.8 ( 140) | ≥ 6.1 (≥110) & ≤ 7.0 (≤126) | 42-46 | 6.0-6.4 |
| Impaired glucose tolerance | ≥ 7.8 (≥140) | < 7.0 (< 126) | 42-46 | 6.0-6.4 |
| Diabetes mellitus | ≥11.1 (≥200) | ≥ 7 (≥ 126) | ≥ 48 | ≥ 6.5 |
Table 2: Diagnosis of diabetes mellitus and pre-diabetic states, according to WHO – criteria.
According to the literature, the frequency of PLTDM varies from 9 to 63% [9, 12, 13, 14, 15]. This significant difference may be explained with discrepancies in the defining criteria for post-transplantation DM. The latest International Consensus Meeting on Post-transplantation Diabetes Mellitus Guidelines [16], from 2014, excluded transient post- transplantation hyperglycemia from the post-transplantation diabetes mellitus (PTDM) diagnosis. Therefore, when consulting older sources, the reported frequency of PTDM may be higher, because of that matter. Moreover, some studies, most of which are retrospective in nature, adhere to the WHO or ADA criteria, as advised by the International Consensus Guidelines, but others use the need for oral anti- diabetic drugs or insulin administration one month post-LT as inclusion criteria [17, 18, 19]. Moreover there is inconsistency, concerning the monitoring tests – fasting or random plasma glucose, HbA1c or oral glucose-tolerance test (OGTT) [9]. Differences in the follow-up period may also play a major role, which may be contributed to the self-resolving nature of PLTDM in some instances, or the longer survival of patients without PTDM [20].
Risk factors for PLTDM can be divided into two groups – general risk factors for diabetes mellitus and risk factors, specific to the transplant recipients. In the first group reside characteristics as age, male sex, obesity, pre-diabetic states as increased fasting glucose (IFG) and impaired glucose tolerance (IGT), non-alcoholic steato-hepatitis (NASH), positive family history for DM and African-American or Hispanic ethnicity [9, 14, 15, 19, 21]. Regarding the liver-transplant population, some of the specific risk factors are HCV [9, 15, 18, 19, 22, 23] or CMV infection [21], immunosuppression with high-dose corticosteroids [14, 21, 24, 25] and the widespread use of calcineurin inhibitors [14, 15, 18]. Grafts, procured from donors, aged > 60 years [14], deceased donors [21], or donors with histologically verified liver steatosis [26], increase the risk of PLTDM.
Risk factors, related to the transplant procedure itself are cold ischemic time longer than 9 hours [21], high-dose corticosteroid induction [14], and early post-transplant episode of acute graft rejection [12, 19]. Recently there has been a discussion, regarding the statin therapy [27], perioperative hypomagnesemia [28], centripetal obesity [29] and hyperglycemia in the first month after LT as possible risk factors for PLTDM [21].
Post-liver transplantation diabetes mellitus is multifactorial disorder. One of the most important links of the pathogenic chain of this condition is the widespread use of calcineurin inhibitors (CNIs) [30]. Calcineurin inhibitors are a class of powerful immunosuppressive drugs, including cyclosporine and tacrolimus (FK506), which revolutionized organ transplantation, since their introduction. After they are absorbed, they enter the cell cytoplasm and bind to proteins from the immunofiln family. The formed complex inhibits calcineurin – a calcium dependent serine-threonine phosphatase associated with T-cell function and regulation [31, 32]. Calcineurin is a protein present not only in immune cells, but in many other tissues [33]. In the pancreatic islet cells it is responsible for the transcription of survival factors, leading to beta-cell growth and proliferation [34]. In the adipose and muscle tissue, calcineurin is involved in metabolic signaling pathways [9]. CNIs on the other hand interfere with these processes and lead to beta-cell death and peripheral insulin resistance.
Corticosteroids (CS) are other widely used drugs for immunosuppression with a well-known hyperglycemic effect. They interfere with the insulin signaling pathway, reducing glycogenesis, while stimulating gluconeogenesis and thus inducing fasting hyperglycemia. They reduce tissue insulin sensitivity. Through upregulation of kinase – 1 protein, CS lead to membrane polarization and slow-down of vesicle exocytosis from the pancreatic beta-cells [9].
Inhibitors of mammalian target of rapamycine (mTOR inhibitors): sirolimus and everolimus are less frequently used in the setting of liver transplantation. In the cell they form a complex with the FK-binding protein (FK-BP) – the target of tacrolimus and inhibit the mTOR protein [35]. Their impact on glucose regulation seems to be less pronounced than that of CNIs [36].
The liver takes a central role in the glucose, lipid and protein metabolism in the human body. This would suggest that diseases, affecting the liver parenchyma may lead to DM. This feature differentiates post-liver transplant diabetes mellitus from the onset of DM after other solid organ transplantations [37]. According to Stockmann, et al. [38], the occurrence of PLTDM after LDLT is related to the graft function, rather than the immunosuppressive therapy. Hepatitis C virus (HCV) is a leading cause for liver transplantation and a risk factor for diabetes mellitus. Studies show that chronic HCV infection is positively associated with DM [15]. White, et al. [39] documented that chronic HCV infection increases the risk of DM with a factor of 1.7. Another leading cause for liver transplantation is alcoholic liver disease. According to an analysis by Knott, et al. [40] daily alcohol intake of more than 120 g significantly increases the risk for DM. Non-alcoholic steato-hepatitis is increasingly more prevalent as a cause for LT. It is associated with metabolic disturbances, known to be risk factors of DM [41].
The field of transplantology is relatively recent and quite progressive. To help guide decision-making in this quickly evolving area, extensive databases have been created since its dawn, with detailed information about the recipients and the follow-up period. As a result, we are in dispose of a large retrospective cohort and we can readily assess the effect and outcome of certain conditions. PLTDM has been extensively studied in that matter, with unequivocal evidence of its detrimental effects on clinical outcome [42, 43]. In an analysis of The Scientific Registry of Transplant Recipients (SRTR), Younossi, et al. [43] included 85,194 liver transplant recipients, with a median follow up of 6.5 years, indicating presence of pre-LT or post-LT DM as an independent predictors of patient mortality. In a retrospective review, Moon, et al. [42] showed statistically significant difference of patient and graft survival (p = 0.012 and 0.004 respectively) between the normal group and the sustained PLTDM group. The 10-year patient survival was 78% and 69% respectively.
At the present time, cardio-vascular disease (CVD) is one of the main causes of mortality among liver-transplant patients [6]. A report from Johnston, et al. [44] stated that LT recipients are at 2.6 times greater risk of mortality related to CVD, compared to a matched cohort of non-transplant population. PLTDM is also implicated in higher number of acute rejection episodes [45, 46], postoperative renal insufficiency and infectious complications [9, 47].
Diagnosis of PLTDM relies of the same criteria as DM in the general population – fasting plasma glucose levels (FPG) greater than 7 mmol/L (126 mg/dL) or plasma glucose > 11.1 mmol/L (200 mg/dL) on the second hour of oral glucose-tolerance test (OGTT) [11]. From the immediate post-transplant period until the first post-operative month almost all patients experience hyperglycemia, requiring intravenous or subcutaneous insulin administration. This is due to the high-dose corticosteroid induction therapy, surgical stress and pain [9, 48]. Hyperglycemia can also occur as a consequence of infection and critical conditions. While this transient state is important prognostic factor for future development of PLTDM [16, 49], labeling it as such is inappropriate. Accurate diagnosis of PLTDM can be placed, when transplant recipients are discharged, with reduced dosage of corticosteroids and stable maintenance immunosuppression therapy. Screening for PLTDM in the early follow-up period is paramount. It is important to be noted that with LT-recipients post-prandial hyperglycemia is more pronounced than the fasting state [9]. This is the reason for the OGTT to be the preferred screening tool for PLTDM. Moreover, glycated hemoglobin (HbA1c) is quite an unreliable early marker, due to the supposed blood- loss, hemotransfussions and the impaired renal function in the peri-LT period [49]. The importance of recognition of the pre-diabetic states – impaired glucose tolerance, IGT (2h-post-OGTT plasma glucose levels between 7.7mmol/L – 11.2 mmol/L) and increased fasting glucose, IFG (5.5-6.9 mmol/L) is in the context of their predictive value for future development of PLTDM [16].
Meticulous glycemic control from the moment of the transplant procedure is extremely important, for ensuring better surgical outcomes. Studies show, that elevated serum glucose values intraoperatively are associated with higher frequency of infectious complications (48% vs 30 % in the group with tight glycemic control, p=0.02) and increased 1-year mortality (21.9% vs. 8.8%, p=0.05) [50]. In another report, Park, et al. [51] stated, that intraoperative hyperglycemia, over 11.1 mmlo/L (>200 md/dL) was independently associated with surgical site infections. Other studies have linked poor glycemic control with longer periods of ICU – stay and longer time to wean off ventilation support [52, 53].
In a recent report, Boerner, et al. [49] have outlined the specifics of hyperglycemia management of the transplanted patients. In general, the aimed glucose values should be no different than for the other patients. Although achieving adequate control is more difficult, due to changing doses of corticosteroids and other immunosuppressive medication, the goals are 7.7 mmol/L-10 mmol/L (140-180 mg/dL) in the ICU, outside the ICU < 7.7 mmol/L ( 140 mg/dL) for fasting and < 10 mmol/L (180 mg/dL) for post-prandial.
Immediately after transplantation, the patients are started on intravenous insulin infusion that should be transitioned to subcutaneous administration as soon as the patient is started on enteral or dietary nutrition. Calculating the initial insulin requirements based on units per kilogram is not sufficiently reliable, because of variations in immunosuppressive medication, renal function, obesity and changing insulin resistance. Therefore, glucose should be measured at bedside on a regular 4- or 6-hour intervals. Synchronizing intermediary or long-acting insulin administration with the timing of corticosteroid administration would allow dose titration in order to cover the increased insulin requirements over that interval.
Overall multidisciplinary management with day-to day titration of the insulin dose, according to changes of caloric intake and immunosuppression is essential for achieving the best results. During hospital stay, the transplant patient should be evaluated for the need of ambulatory insulin therapy, so that education of the patient and relatives for glucose monitoring and insulin administration can be initiated. Concerning the oral anti-diabetic drugs, there are only a few studies, assessing their safety in transplant patients and their use in early onset PLTDM is limited [9]. On the other hand, late onset PLTDM can be managed in a stepwise manner of lifestyle modification, followed by oral anti-diabetic drugs and finally inclusion of insulin therapy [16, 54]. As mentioned earlier, immunosuppressive drugs have a profound influence over the pathogenesis of PLTDM.
Despite the revolution that was the discovery of calcineurin inhibitors, corticosteroids, with their pronounced diabetogenic effects, still remain the most used drugs for induction of immunosuppression [55]. There are several studies assessing the efficacy of non-steroid induction therapy, but still more research is needed [9]. In the literature there are reports evaluating different steroid- withdraw protocols, demonstrating lower frequency of PLTDM at the end of the follow-up period [56, 57]. However, a recent Cochrane Collaboration meta-analysis reported that steroid-avoidance and early steroid-withdraw protocols are associated with increased frequency of acute graft rejection events [58]. Advancing research in this area should be done in caution, as the minimal reduction of the post-transplant DM frequency should not compromise graft survival [16, 59]. Moreover, antirejection therapy itself is a risk factor for PLTDM.
Clinical evidence clearly differentiates the influence of different CNIs on glucose metabolism. Data from two meta-analyses, comparing cyclosporine with tacrolimus demonstrates lower risk of PLTDM with cyclosporine [60, 61]. Nevertheless, tacrolimus demonstrated better survival rates and lower frequency of acute rejection and hypertension among recipients. Clearly the optimal immunosuppression regiment has not been established yet. Now, as 50 years ago, tackling the immune system continues to be the cornerstone of organ transplantation. While a lot has been achieved and a lot of factors, adversely affecting patient and graft survival have been determined, we are limited by the need to fool the body’s defenses.
Conclusion
Post-liver transplantation diabetes mellitus is a frequent metabolic complication, with well documented detrimental effects on patient and graft survival. Patients at risk for developing PLTDM should be identified and advised on lifestyle modification and weight loss. Appropriate evaluation of CVD and actions for reduction of the cardiovascular risk are recommended. In the peri- and post-transplant period, strict monitoring of the blood glucose levels, and management by a multidisciplinary team is advocated in order to reduce the probability of developing PLTDM and related complications.
References
-
(2018) The Organ Procurement and Transplant Network.
-
Adam R, Karam V, Delvart V, O’Grady J, Mirza D, et al. (2012) Evolution of indications and results of liver transplantation in Europe. A report from the European Liver Transplant Registry (ELTR). J Hepatol 57(3): 675- 688.
-
Rupp C, Hippchen T, Neuberger M, Sauer P, Pfeiffenberger J et al. (2018) Successful combination of direct antiviral agents in liver-transplanted patients with recurrent hepatitis C virus. World J Gastroenterol 24(12): 1353- 1360.
-
Nogueras Lopez F, López Garrido A, Ortega Suazo EJ, Vadillo Calles F, Valverde López F, et al. (2018) Therapy With Direct-Acting Antiviral Agents for Hepatitis C in Liver Transplant Recipients. Transplant Proc 50(2): 631- 633.
-
Ciesek, S, Otto B, Pischke S, Costa R, Lüthgehetmann M, et al. (2016) Efficacy and safety of sofosbuvir/ledipasvir for the treatment of patients with hepatitis C virus re- infection after liver transplantation. Transpl Infect Dis 18(3): 326-332.
-
Roccaro GA, Goldberg DS, Hwang WT, Judy R, Thomasson A, et al. (2018) Sustained Posttransplantation Diabetes Is Associated With Long-Term Major Cardiovascular Events Following Liver Transplantation. Am J Transplant 18(1): 207-215.
-
Khurmi NS, Chang YH, Eric Steidley D, Singer AL, Hewitt WR, et al. (2018) Hospitalizations for cardiovascular disease after liver transplantation in the United States. Liver Transpl 24(10): 1398-1410.
-
Atlas D (2015) International Diabetes Federation (IDF) Diabetes Atlas. 7th (Edn.), Brussels, Belgium: International Diabetes Federation.
-
Pelaez Jaramillo MJ, Cárdenas Mojica AA, Gaete PV, Mendivil CO (2018) Post-Liver Transplantation Diabetes Mellitus: A Review of Relevance and Approach to Treatment. Diabetes Ther 9(2): 521-543.
-
WHO (2006) Definition and diagnosis of diabetes mellitus and intermediate hyperglycemia: report of a WHO/IDF consultation.
-
Inzucchi SE, Bergenstal RM, Buse JB, Diamant M, Ferrannini E, et al. (2015) Management of hyperglycemia in type 2 diabetes, 2015: a patient-centered approach: update to a position statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care 38(1): 140-149.
-
Linder KE, Baker WL, Rochon C, May ST, Sheiner PA, et al. (2016) Evaluation of Posttransplantation Diabetes Mellitus After Liver Transplantation: Assessment of Insulin Administration as a Risk Factor. Ann Pharmacother 50(5): 369-375.
-
Mirabella S, Brunati A, Ricchiuti A, Pierini A, Franchello A, et al. (2005) New-onset diabetes after liver transplantation. Transplant Proc 37(6): 2636-2637.
-
Kuo HT, Sampaio MS, Ye X, Reddy P, Martin P, et al. (2010) Risk factors for new-onset diabetes mellitus in adult liver transplant recipients, an analysis of the Organ Procurement and Transplant Network/United Network for Organ Sharing database. Transplantation 89(9): 1134-1140.
-
Li DW, Lu TF, Hua XW, Dai HJ, Cui XL, et al. (2015) Risk factors for new onset diabetes mellitus after liver transplantation: A meta-analysis. World J Gastroenterol 21(20): 6329-6340.
-
Sharif A, Hecking M, de Vries AP, Porrini E, Hornum M, et al. (2014) Proceedings from an international consensus meeting on posttransplantation diabetes mellitus: recommendations and future directions. Am J Transplant 14(9): 1992-2000.
-
Baid S, Cosimi AB, Farrell ML, Schoenfeld DA, Feng S, et al. (2001) Posttransplant diabetes mellitus in liver transplant recipients: risk factors, temporal relationship with hepatitis C virus allograft hepatitis, and impact on mortality. Transplantation 72(6): 1066-1072.
-
Khalili M, Lim JW, Bass N, Ascher NL, Roberts JP, et al. (2004) New onset diabetes mellitus after liver transplantation: the critical role of hepatitis C infection. Liver Transpl 10(3): 349-355.
-
Yadav AD, Chang YH, Aqel BA, Byrne TJ, Chakkera HA, et al. (2013) New Onset Diabetes Mellitus in Living Donor versus Deceased Donor Liver Transplant Recipients: Analysis of the UNOS/OPTN Database. J Transplant 2013: 269096.
-
Lv C, Zhang Y, Chen X, Huang X, Xue M, et al. (2015) New- onset diabetes after liver transplantation and its impact on complications and patient survival. J Diabetes 7(6): 881-890.
-
Ling, Q, Xu X, Xie H, Wang K, Xiang P, et al. (2016) New- onset diabetes after liver transplantation: a national report from China Liver Transplant Registry. Liver Int 36(5): 705-712.
-
Hartog H, May CJ, Corbett C, Phillips A, Tomlinson JW, et al. (2015) Early occurrence of new-onset diabetes after transplantation is related to type of liver graft and warm ischaemic injury. Liver Int 35(6): 1739-1747.
-
Soule JL, Olyaei AJ, Boslaugh TA, Busch AM, Schwartz JM, et al. (2005) Hepatitis C infection increases the risk of new-onset diabetes after transplantation in liver allograft recipients. Am J Surg 189(5): 552-557.
-
Honda M, Asonuma K, Hayashida S, Suda H, Ohya Y, et al. (2013) Incidence and risk factors for new-onset diabetes in living-donor liver transplant recipients. Clin Transplant 27(3): 426-435.
-
Pirsch JD, Henning AK, First MR, Fitzsimmons W, Gaber AO, et al. (2015) New-Onset Diabetes After Transplantation: Results From a Double-Blind Early Corticosteroid Withdrawal Trial. Am J Transplant 15(7): 1982-1990.
-
Xue M, Lv C, Chen X, Liang J, Zhao C, et al. (2017) Donor liver steatosis: A risk factor for early new-onset diabetes after liver transplantation. J Diabetes Investig 8(2): 181- 187.
-
Cho Y, Lee MJ, Choe EY, Jung CH, Joo DJ, et al. (2014) Statin therapy is associated with the development of new- onset diabetes after transplantation in liver recipients with high fasting plasma glucose levels. Liver Transpl 20(5): 557-563.
-
Van Laecke S, Desideri F, Geerts A, Van Vlierberghe H, Berrevoet F, et al. (2010) Hypomagnesemia and the risk of new-onset diabetes after liver transplantation. Liver Transpl 16(11): 1278-1287.
-
Vaughn VM, Cron DC, Terjimanian MN, Gala ZS, Wang SC, et al. (2015) Analytic morphomics identifies predictors of new-onset diabetes after liver transplantation. Clin Transplant 29(5): 458-464.
-
Heisel O, Heisel R, Balshaw R, Keown P (2004) New onset diabetes mellitus in patients receiving calcineurin inhibitors: a systematic review and meta-analysis. Am J Transplant 4(4): 583-595.
-
Jain J, McCaffrey PG, Miner Z, Kerppola TK, Lambert JN, et al. (1993) The T-cell transcription factor NFATp is a substrate for calcineurin and interacts with Fos and Jun. Nature 365(6444): 352-355.
-
Clipstone NA, Crabtree GR (1992) Identification of calcineurin as a key signalling enzyme in T-lymphocyte activation. Nature 357(6380): 695-697.
-
Kung L, Batiuk TD, Palomo-Pinon S, Noujaim J, Helms LM, et al. (2001) Tissue distribution of calcineurin and its sensitivity to inhibition by cyclosporine. Am J Transplant 1(4): 325-333.
-
Soleimanpour SA, Crutchlow MF, Ferrari AM, Raum JC, Groff DN, et al. (2010) Calcineurin signaling regulates human islet {beta}-cell survival. J Biol Chem 285(51): 40050-40059.
-
Waldner M, Fantus D, Solari M, Thomson AW (2016) New perspectives on mTOR inhibitors (rapamycin, rapalogs and TORKinibs) in transplantation. Br J Clin Pharmacol 82(5): 1158-1170.
-
Ju WQ, Guo ZY, Liang WH, Wu LW, Tai Q, et al. (2012) Sirolimus conversion in liver transplant recipients with calcineurin inhibitor-induced complications: efficacy and safety. Exp Clin Transplant 10(2): 132-135.
-
Ling Q, Xu X, Wang B, Li L, Zheng S (2016) The Origin of New-Onset Diabetes After Liver Transplantation: Liver, Islets, or Gut? Transplantation 100(4): 808-813.
-
Stockmann M, Konrad T, Nolting S, Hünerbein D, Wernecke KD, et al. (2006) Major influence of liver function itself but not of immunosuppression determines glucose tolerance after living-donor liver transplantation. Liver Transpl 12(4): 535-543.
-
White DL, Ratziu V, El Serag HB (2008) Hepatitis C infection and risk of diabetes: a systematic review and meta-analysis. J Hepatol 49(5): 831-844.
-
Knott C, Bell S, Britton A (2015) Alcohol Consumption and the Risk of Type 2 Diabetes: A Systematic Review and Dose-Response Meta-analysis of More Than 1.9 Million Individuals From 38 Observational Studies. Diabetes Care 38(9): 1804-1812.
-
Jakobsen MU, Berentzen T, Sørensen TI, Overvad K (2007) Abdominal obesity and fatty liver. Epidemiol Rev 29: 77-87.
-
Moon JI, Barbeito R, Faradji RN, Gaynor JJ, Tzakis AG (2006) Negative impact of new-onset diabetes mellitus on patient and graft survival after liver transplantation: Long-term follow up. Transplantation 82(12): 1625- 1628.
-
Stepanova M, Wai H, Saab S, Mishra A, Venkatesan C, et al. (2015) The outcomes of adult liver transplants in the United States from 1987 to 2013. Liver Int 35(8): 2036- 2041.
-
Johnston SD, Morris JK, Cramb R, Gunson BK, Neuberger J (2002) Cardiovascular morbidity and mortality after orthotopic liver transplantation. Transplantation 73(6): 901-916.
-
John PR, Thuluvath PJ (2002) Outcome of patients with new-onset diabetes mellitus after liver transplantation compared with those without diabetes mellitus. Liver Transpl 8(8): 708-713.
-
Wallia A, Parikh ND, Molitch ME, Mahler E, Tian L, et al. (2010) Posttransplant hyperglycemia is associated with increased risk of liver allograft rejection. Transplantation 89(2): 222-226.
-
Wallia A, Schmidt K, Oakes DJ, Pollack T, Welsh N, et al. (2017) Glycemic Control Reduces Infections in Post- Liver Transplant Patients: Results of a Prospective, Randomized Study. J Clin Endocrinol Metab 102(2): 451- 459.
-
Pei D, Chen TW, Kuo YL, Hung YJ, Hsieh CH, et al. (2003) The effect of surgical stress on insulin sensitivity, glucose effectiveness and acute insulin response to glucose load. J Endocrinol Invest 26(5): 397-402.
-
Boerner B, Shivaswamy V, Goldner W, Larsen J (2015) Management of the hospitalized transplant patient. Curr Diab Rep 15(4): 19.
-
Ammori JB, Sigakis M, Englesbe MJ, O’Reilly M, Pelletier SJ (2007) Effect of intraoperative hyperglycemia during liver transplantation. J Surg Res 140(2): 227-233.
-
Park C, Hsu C, Neelakanta G, Nourmand H, Braunfeld M, et al. (2009) Severe intraoperative hyperglycemia is independently associated with surgical site infection after liver transplantation. Transplantation 87(7): 1031- 1036.
-
Foxton MR, Quaglia A, Muiesan P, Heneghan MA, Portmann B, et al. (2006) The impact of diabetes mellitus on fibrosis progression in patients transplanted for hepatitis C. Am J Transplant 6(8): 1922-1929.
-
Wallia A, Parikh ND, O Shea Mahler E, Schmidt K, DeSantis AJ, et al. (2011) Glycemic control by a glucose management service and infection rates after liver transplantation. Endocr Pract 17(4): 546-551.
-
Sharif A, Moore R, Baboolal K (2008) Influence of lifestyle modification in renal transplant recipients with postprandial hyperglycemia. Transplantation 85(3): 353-358.
-
Dhanasekaran R (2017) Management of Immunosuppression in Liver Transplantation. Clin Liver Dis 21(2): 337-353.
-
Ju WQ, Guo ZY, Ling X, He XS, Wu LW, et al. (2012) Twenty- four hour steroid avoidance immunosuppressive regimen in liver transplant recipients. Exp Clin Transplant 10(3): 258-262.
-
Kim YK, Lee KW, Kim SH, Cho SY, Han SS, et al. (2012) Early steroid withdrawal regimen prevents new-onset diabetes mellitus in old-age recipients after living donor liver transplantation. World J Surg 36(10): 2443-2448.
-
Fairfield C, Penninga L, Powell J, Harrison EM, Wigmore SJ, et al. (2014) Glucocorticosteroid-free versus glucocorticosteroid-containing immunosuppression for liver transplanted patients. Cochrane Database Syst Rev 15(12): CD007606.
-
Woodle ES, First MR, Pirsch J, Shihab F, Gaber AO, et al. (2008) A prospective, randomized, double-blind, placebo-controlled multicenter trial comparing early (7 day) corticosteroid cessation versus long-term, low- dose corticosteroid therapy. Ann Surg 248(4): 564-577.
-
Haddad EM, McAlister VC, Renouf E, Malthaner R, Kjaer MS, et al. (2006) Cyclosporin versus tacrolimus for liver transplanted patients. Cochrane Database Syst Rev (4): Cd005161.
-
Muduma G, Saunders R Systematic, Odeyemi I, Pollock RF (2016) Review and Meta-Analysis of Tacrolimus versus Ciclosporin as Primary Immunosuppression After Liver Transplant 11(11): e0160421.
- Reconstruction of Nasal Defect Using a Local Flap Based in the Nanoperforants Concept: A Case Report
- Transplant Tourism in Japan: Insights from Nationwide Surveys and Emerging Ethical Challenges
- The Challenge of Peritoneal Vaginoplasty in Transgender Women: Review Literature and Personal Perspectives
- Algorithmic Paternalism: Autonomy Versus Automation
- Dermatoscopy in Gorlin Syndrome: Avoiding the Disfigurement in Patients
- How Artificial Intelligence is Ushering in a New Era of Innovation in General and Plastic Surgery: A Short Communication