Biomechanical Stress Distribution of the Mandibular Condyle in Orthognathic Surgery with Occlusal Plane Counterclockwise Rotation-A Case Report
Purpose: To analyze the changes in stress distribution at the condylar level after maxillomandibular surgery with counterclockwise rotation in a case report. Materials and Methods: A real model of a class III malocclusion patient was obtained and corrected by bimaxillary surgery with counterclockwise rotation. Finite element analysis was performed with the properties of trabecular and cortical bone, articular disc, and teeth assumed and modeled under a continuous homogeneous anisotropic approach. The T-Students test and Pearson's correlation coefficient were performed. Results: The condylar topography showed changes in the distribution of mechanical stress uniformly in the three-dimensional model's post-surgical simulation. The reductions of the various stress areas did not show statistical significance. Conclusion: In our case, bimaxillary orthognathic surgery with a change in the occlusal plane in a counterclockwise rotation did not represent a risk in altering the condylar morphology. Biomechanical stress distribution can be adequately distributed with passive accentuation of the condyle in the mandibular fossa during the procedure in class III patients with an anterior open bite. However the article involves only one case. Therefore, larger studies are recommended and these results should be interpreted with caution.
Introduction
Phillips and Bell, in 1978, were the first to report a case of condylar resorption after mandibular advancement orthognathic surgery, although at the time they could not establish the cause, it is believed that it could be a biomechanical phenomenon with increased muscle tension [1]. Among several causes of condylar alterations, biomechanical stress (including stretching or compression) can cause adaptation in soft and hard tissues that is frequently manifested by condylar elongation or reabsorption [2]. Condylar resorption has a multifactorial etiology, including factors related to the host and biomechanical factors [3]. After mandibular and maxillary orthognathic surgery, the condyle tends to be located in a concentric way within the glenoid cavity. However, it may not necessarily trigger joint symptoms, being the most stable position [4]. Also, bimaxillary orthognathic surgery with counterclockwise rotation has usually been stigmatized due to the increased risk of condylar resorption.
The aim of this article is to show a case that assesses the biomechanical stress of the condyles with a three-dimensional simulation of a class III patient with an anterior open bite in maxillomandibular surgery with counterclockwise rotation.
Materials and Methods
Preoperative and Postoperative Models
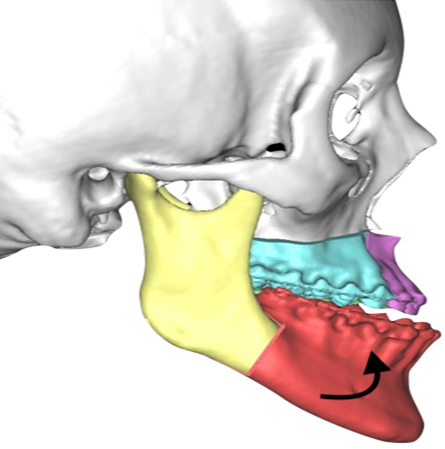
The mathematical model’s geometry was based on the preoperative CT images of a 25 -year-old female patient with dentofacial anomalies class III who assisted at Oral and Maxillofacial Department of the Hospital Universitario La Samaritana. Bogota, Colombia. The patient who underwent BSSO and Lefort I osteotomy with occlusal plane counterclockwise rotation was enrolled in this case approved by the ethical review board of the Institution (Figure 1). The patient provided the written informed consent. No signs or symptoms of Temporomandibular Disorders were found preoperatively and postoperatively at 1 year postoperative follow-up.
The preoperative computed tomography (CT) and postoperative CT were obtained with 1 year of difference under the protocol of helical technique and gantry 0º was made. The head’s scans consisted of 350 images, with a slice thickness of 0,6 mm and using a DICOM format to be exported. The model was reconstructed in a 3D SLICER (© Copyright 2020, Slicer Community BSD-style license) and an equidistant triangular mesh was built (Tetrahedron- Tet4, isosceles 1mm, 170,000 triangles, Jacobian <0.91. (0.91 <1[optimal Jacobian]). Once the model was finished, all digitized anatomical structures were inputted into 8.0 (Swanson Analysis System Co., Houston, TX, USA) in which, for simulation structural analysis, all features were loaded (internal materials properties and boundary conditions).
Properties of Elements
According to related studies, the elements analyzed in this study, the mechanical properties of Young’s modulus (E) (MPa) and Poisson’s ratio (v) of cortical bone were 13.700 and 0.3 respectively, in the case of cancellous bone were 7930 and 0.3, the articular cartilage values were 0.79 and 0.49, and articular disc were 44.1 and 0.4 respectively. All of them were assumed to be homogeneous, isotropic, and linearly modeled according to related studies. Interactions between the interfaces were considered as contact with a frictional coefficient of 0.001 (Table 1).
| Materials Properties of TMJ Components | ||
|---|---|---|
| Young’s Modulus (E) (MPA) | Poisson’s Ratio (V) | |
| Cortical Bone | 13.7 | 0.3 |
| Cancellous Bone | 7930 | 0.3 |
| Articular Cartilage | 0.79 | 0.49 |
| Articular Disc | 44.1 | 0.4 |
| Teeth | 18.6 | 0.31 |
Table 1: Temporomandibular joint properties studied.
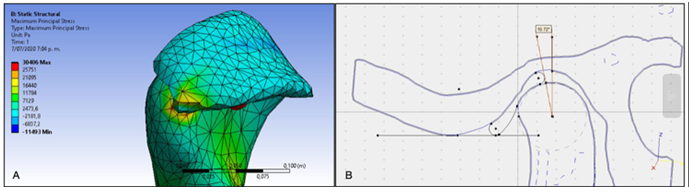
The articular disc was simulated under anatomical maximum occlusal intercuspation similar to the anatomical boundaries in a frontal plane, limiting medial and lateral poles of the mandibular condyle that had a conventional ovoid shape with no signs of bone degeneration or abnormalities in shape. In a sagittal plane, the disc’s posterior limit was located 10º degrees in front of the vertical axis of the center of rotation of the mandibular condyle. Moreover, its volume was determined by the space between the condyle and mandibular fossa (Figure 2).
The Temporomandibular muscles and ligaments were simulated under the strict anatomical relationship. The mean maximum force generated by each masticatory muscles are directly proportional to intrinsic force constant P, by its cross-section A (i) F MAX = pA(I) P is 0.37x 106 N / m squared; these values for each muscle Fmax (i) are then normalized by the Cartesian components of each one from its origin to its insertion (xi, yj, zk).
F muscular=Fmax (i)x (xi,yj,kz)/ IMI
For this study, the biomechanical stress distribution of the left and right mandibular condyles was analyzed. The anterior condyles, medial, central, and lateral areas were studied, and dynamics simulation was made. The statistical analyses were performed using the statistical software package SPSS version 21.0 for Windows (SPSS Inc., Chicago, USA). All effort variables were recollected (Von Mises and shears). The one-sample t-test was used to test the variables group’s significance (Von Mises and shears efforts on condyle areas pre-surgical and post-surgical (p= 0.05)). Pearson’s correlation test was performed to assess the measured linear dependence between the two variables. The significance level was set at 0.05. All analyzes are under the 95% level of statistical significance.
Results
Collision analysis of pre and post-surgical images was initially performed; showing a rotation of the mandibular condyle and anterior displacement of the proximal segment of the right mandibular ramus at the level of the neck of the condyle of 2.66 mm and at the level of the anterior border of the ramus 2.86 mm. On the left side, there was evidence of condylar rotation with a displacement of the proximal segment anteriorly of 2.93 mm at the level of the condyle and a displacement of the ramus of 3.2mm anteriorly. The distribution patterns and areas of most significant stress of the mandibular condyles were measured in stress variables:
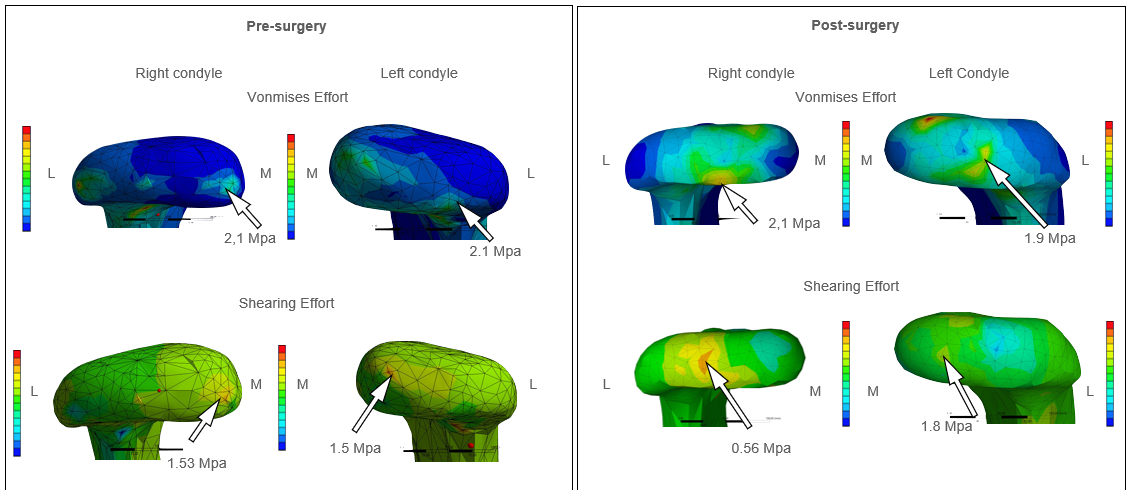
Von Mises and Shear. In the presurgical simulation, the right condyle showed a Vonmises effort of 2.1 Mp in the medial region (MR), and a shear stress of 1.53 Mp reflected also in the MR of the condyle. In the left condyle, the area of most tremendous pre-surgical stress was the lateral region (LR) showing a Von Mises effort of 2.1 Mp and the central region (CR) with a shear stress of 1.5 Mp. The distribution patterns and areas of most significant stress of the mandibular condyles in the post-surgical simulation were: Von Mises effort of 2.1 Mp for the right condyle in the CR and a shear stress of 0.56 Mp also in the CR. For the left condyle, the most significant post-surgical stress area was the CR with 1.9 Mp in Von Mises effort and 1.8 Mp in the MR for shear stress (Figure 3).
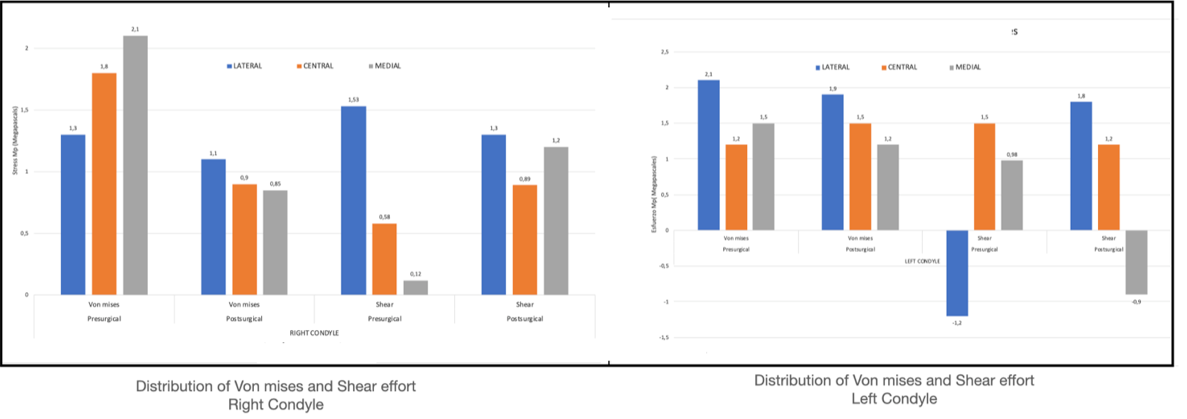
Average Von Mises stress was 1.73 Mpa in the pre- surgery and 1 MPa for the post-surgery in the right condyle (reduction of 42.1%). Shear effort average for the pre was 0.74 Mpa and the post average was 0.15 Mpa (79% decrease). According to T students’ test, it was observed that the results of the right condyle in Von Mises effort before and after surgery had a statistically significant reduction, CI = 95% (p= 0.008), while the Pearson Correlation expresses a perfect correlation linearly negative (-0.96). On the other hand, the pre and post shear stress does not represent a statistically significant reduction for the right condyle, CI = 95% (p= 0.27) and a weak linear positive Pearson correlation (0.41). Regarding the left condyle, the average of Von Mises effort was 1,6 for the preoperative period and 1,53 for the post- surgical period (decrease of 4.4%). The average shear effort showed a slight increase for the left condyle, being 0,42 for the preoperative period and 0,7 for the postoperative period (an increase of 66%). The pre and postsurgical Von mises effort does not represent a statistically significant reduction, CI = 95% (p= 0.75) for the left condyle. On the other hand, the Pearson correlation showed a significantly positive linear (0.71). The pre and post shear stress does not represent a statistically significant reduction either, CI = 95% (p= 0.86), with a moderately linear negative Pearson correlation (-0.52). Finally, preoperative and postoperative X rays were compared to evaluate facial changes and osteosíntesis material was in position without infection signs (Figure 4).
Discussion
Orthognathic surgery can trigger some changes at the condylar level. These changes can be divided into condylar remodeling or condylar resorption. In the second situation, the condyle exceeds the adaptive capacity, becoming a pathological process due to load and position changes in the condyle. The systematic review by Vandeput, et al. [5] found condylar remodeling in class III patients due to mandibular setback. However, the literature was not conclusive due to the heterogeneity of the studies and the level of evidence [5].
Regarding condylar position changes Kim, et al. [6] conducted a study in 33 subjects with class III malocclusion. Bimaxillary orthognathic surgery was performed with a 1-year tomographic follow-up. Condylar movements in different directions were observed up to six months, which influenced a relapse of surgery. However, they note that these movements stabilize after one year suggesting condylar remodeling not condylar resorption [6]. On the other hand, Park, et al. [7], 22 patients with class III malocclusion who underwent Le Fort I osteotomy and mandibular setback by sagittal osteotomy were studied to observe changes in height and condylar shape in those who observed remodeling and loss of height after surgery. The anterior and superior visualization remodeling changes, and the superior and lateral visualization resorption changes [7]. This suggests the importance of assessing the intraoperative condylar position in whichever procedure to be performed.
Regarding changes in the occlusal plane, Kor, et al. [8] conducted a study in 29 patients with class III malocclusion and anterior open bite divided into two groups. One group consisted of patients with a clockwise occlusion change and the other group in a counterclockwise direction. Changes occurred in both groups; however, in the group with counterclockwise rotation, more remarkable changes occurred at the level of point B, pogonion, and chin. Despite these results, both groups were relatively stable techniques [8]. This could destigmatize the counterclockwise rotation, showing that when it is not carried out there may also be a remodeling; however in both cases it can be stable.
Regarding the differences between a jaw or bimaxillary surgery, a study was carried out by Kim, et al. [9] where they evaluated the condylar changes in class III patients managed with sagittal osteotomy mandible or bimaxillary surgery. The results observed in the 43 patients analyzed did not show statistically significant differences in condylar displacements in the frontal, sagittal and axial planes. In addition, the remodeling variation was less than 2 mm, which lacked clinical relevance [9]. However, the possibility of condylar resorption in forward or mandibular setback by sagittal osteotomy with and without Le Fort I osteotomy is in a percentage lower than 4.2%, according to a systematic review and meta-analysis [10]. In our case of bimaxillary surgery, an excessive overload was not observed in the finite element analysis. This may suggest that the risk of presenting condylar changes is lower with bimaxillary surgery with counterclockwise rotation, but studies with a larger number of patients should be carried out.
Additionally, Al-Moraissi and Wolford conducted a systematic review and meta-analysis in which they observed the stability of the counterclockwise rotation of the maxillomandibular complex in orthognathic surgery with or without treatment of coexisting temporomandibular joint pathology. Three hundred forty-five patients were included from a total of 12 studies where they performed the fixed- point evaluation, linear measurements, and evaluation of the occlusal plane. They concluded that the maxillomandibular complex’s counterclockwise rotation was a stable procedure in healthy patients or those who had joint pathology previously or concomitantly treated. However, it was unstable in patients with joint pathology that had not received treatment [11]. In our case, the patient did not present joint pathology before surgery and neither development after it. Therefore, no surgical intervention related to the ATM was necessary, other than passive condylar repositioning during orthognathic surgery.
Finally, it must be considered that relapse has a multifactorial etiology where variables such as age, degree of advancement or retreat, muscular activity, and even the surgeon’s ability to accentuate the mandibular condyle in the glenoid cavity passively can affect results. In addition, it is believed that the fixing material can play a relevant role. Al- Moraissi and Ellis, in a systematic review and meta-analysis, observed a slight advantage over bicortical screws in terms of postoperative stability, however no statistically significant differences were found [12]. In our team we always use three bicortical screws on each side of the mandible, and so far we have had good results.
In our study, the condylar topography showed changes in mechanical stress distribution uniformly in the three- dimensional model’s post-surgical simulation. The reductions of the various stress areas were shown not to have a statistical significance. However, the patterns of the overturning of the forces in the right mandibular condyle evidenced a more significant pre-surgical Von Mises effort in the medial region, presenting a change in the pattern of this effort, towards the lateral side in the post-surgical simulation. On the other hand, the pre-surgical shear stress presented a more accentuated component in the medial region, with a better post-surgical distribution of the shear stresses. The left mandibular condyle demonstrated an undiminished pattern of pre and post-surgical Von Mises efforts. The pre and post-surgical shear stresses showed negative patterns that initially appeared in the lateral portion of the left condyle. In the postsurgical simulation, these biodynamic patterns’ clinical relevance was observed in the medial portion, which should be evaluated in the clinic scenario since the shear forces are highly damaging to the disc and articular cartilage. Therefore, proper manipulation of the proximal segment at the time of performing a bimaxillary orthognathic surgery procedure with occlusal plane change does not represent a risk in altering the condylar morphology if the distribution of the biomechanical efforts can be distributed adequately with a passive accentuation of the condyle in the mandibular fossa during the surgical procedure.
Conclusion
Despite the fact that many articles report cases of condylar resorption or remodeling after orthognathic surgery, most articles suggest that search information is needed with technological tools that provide better information. Consequently, this case of finite element analysis, which to our knowledge is the first to use this technique to evaluate the load received after this type of procedure. Likewise, it is observed that an adequate load distribution on the condyle is possible after bimaxillary orthognathic surgery with anticlockwise rotation. Finally, our case can be the basis and the beginning of studies with finite element analysis that use larger samples and adequate control of variables in order to obtain higher quality information.
Consent
The consent for publication was obtained.
Conflict of Interest Statement
The authors have expressed no conflict of interests.
References
-
Phillips RM, Bell WH (1978) Atrophy of mandibular condyles after sagittal ramus split osteotomy: report of case. J Oral Surg 36(1): 45-49.
-
Arnett GW, Milam SB, Gottesman L (1996) Progressive mandibular retrusion--idiopathic condylar resorption. Part I. Am J Orthod Dentofacial Orthop 110(1): 8-15.
-
Arnett GW, Milam SB, Gottesman L (1996) Progressive mandibular retrusion-idiopathic condylar resorption. Part II. Am J Orthod Dentofacial Orthop 110(2): 117-127.
-
Chen S, Lei J, Wang X, Fu KY, Farzad P, et al. (2013) Short- and long-term changes of condylar position after bilateral sagittal split ramus osteotomy for mandibular advancement in combination with Le Fort I osteotomy evaluated by cone-beam computed tomography. J Oral Maxillofac Surg 71(11): 1956-1966.
-
Vandeput AS, Verhelst PJ, Jacobs R, Shaheen E, Swennen G, et al. (2019) Condylar changes after orthognathic surgery for class III dentofacial deformity: a systematic review. Int J Oral Maxillofac Surg 48(2): 193-202.
-
Kim YJ, Lee Y, Chun YS, Kang N, Kim SJ, et al. (2014) Condylar positional changes up to 12 months after bimaxillary surgery for skeletal class III malocclusions. J Oral Maxillofac Surg 72(1): 145-156.
-
Park SB, Yang YM, Kim YI, Cho BH, Jung YH, et al. (2012) Effect of bimaxillary surgery on adaptive condylar head remodeling: metric analysis and image interpretation using cone-beam computed tomography volume superimposition. J Oral Maxillofac Surg 70(8): 1951- 1959.
-
Kor HS, Yang HJ, Hwang SJ (2014) Relapse of skeletal class III with anterior open bite after bimaxillary orthognathic surgery depending on maxillary posterior impaction and mandibular counterclockwise rotation. J Craniomaxillofac Surg 42(5): e230-e238.
-
Kim YJ, Oh KM, Hong JS, Lee JH, Kim MH, et al. (2012) Do patients treated with bimaxillary surgery have more stable condylar positions than those who have undergone single-jaw surgery?. J Oral Maxillofac Surg 70(9): 2143-2152.
-
Nunes de Lima V, Faverani LP, Santiago JF, Palmieri C, Filho OM, Pellizzer EP (2018) Evaluation of condylar resorption rates after orthognathic surgery in class II and III dentofacial deformities: A systematic review. J Craniomaxillofac Surg 46(4): 668-673.
-
Al-Moraissi EA, Wolford LM (2017) Does Temporomandibular Joint Pathology With or Without Surgical Management Affect the Stability of Counterclockwise Rotation of the Maxillomandibular Complex in Orthognathic Surgery? A Systematic Review and Meta-Analysis. J Oral Maxillofac Surg 75(4): 805- 821.
-
Al-Moraissi EA, Ellis E (2016) Stability of bicortical screw versus plate fixation after mandibular setback with the bilateral sagittal split osteotomy: a systematic review and meta-analysis. Int J Oral Maxillofac Surg 45(1): 1-7.
-
Nagahara K, Murata S, Nakamura S, Tsuchiya T (1999) Displacement and stress distribution in the temporomandibular joint during clenching. Angle Orthod 69(4): 372-379.
- Reconstruction of Nasal Defect Using a Local Flap Based in the Nanoperforants Concept: A Case Report
- Transplant Tourism in Japan: Insights from Nationwide Surveys and Emerging Ethical Challenges
- The Challenge of Peritoneal Vaginoplasty in Transgender Women: Review Literature and Personal Perspectives
- Algorithmic Paternalism: Autonomy Versus Automation
- Dermatoscopy in Gorlin Syndrome: Avoiding the Disfigurement in Patients
- How Artificial Intelligence is Ushering in a New Era of Innovation in General and Plastic Surgery: A Short Communication