Role of Platelet Rich Fibrin Matrix in Management of Electric Burns
Electric burns injury is a problem which is still found now a day. The wound of electric burns ranges from mild blistering to full thickness charring of tissues. When the wound goes into the healing phase there is difficulty due to the nature of the burns and the large area it involves. Any problem with the edge of the wound can be detrimental to healing and may cause delay in wound healing. In this article, we share our experience of using Platelet Rich Fibrin (PRF) for wound bed preparation in electric burns wound healing.
Abbreviations
PPP: Platelet Poor Plasma; PRFM: Platelet Rich Fibrin Matrix; RBCs: Red Blood Cells; PRF: Platelets Rich Fibrin; PRP: Platelet Rich Plasma; VEGF: Vascular Endothelial Growth Factor; FGF-b: Fibroblast Growth Factor-b; HGF: Hepatocyte Growth Factor; Ang-I: Angiopoietin-I.
Introduction
Electric burns is a common problem in our country, ranging from low voltage household to high voltage burns. Fatalities due to electric burns has come down due to progress in the field of household safety. Electric burns causes burns over the surface with loss of tissue and the plastic surgeon faces difficulty in the wound management. Wound bed preparation is a novel concept which is used for the management of wounds that fail to heal well and can be summarized with the T.I.M.E with T for tissue: non- viable or deficient. I for infection/inflammation, M for moisture balance. E for epidermis which was later changed to E for edge which allows the granulation tissue to come. Conventionally Autologous Platelet Rich Plasma is in practice and is used as one of the agents, but recently in literature, we have come across platelet rich fibrin matrix for the use in wound bed preparation.
Materials and Methods
This study was conducted in the department of Plastic Surgery at tertiary care center after the departmental ethical committee approval was taken. Informed written consent was taken from the patient in study. The details of the patient in study are as follows: 8-year old male child with no known co morbidities with h/o Accidental electrocution burn injury (High voltage) sustaining 35 percent burns to the face, neck, chest, abdomen, bilateral upper limb and bilateral lower limb with deep burn injury to the scalp (entry wound) and right great toe (exit wound), previously underwent treatment in department of plastic surgery at tertiary care center. The patient got discharged with healed scalp wound except at one place at less than 0.5cm superficial, presented to us with raw area 1 x 1 cm over scalp with no history of fever.
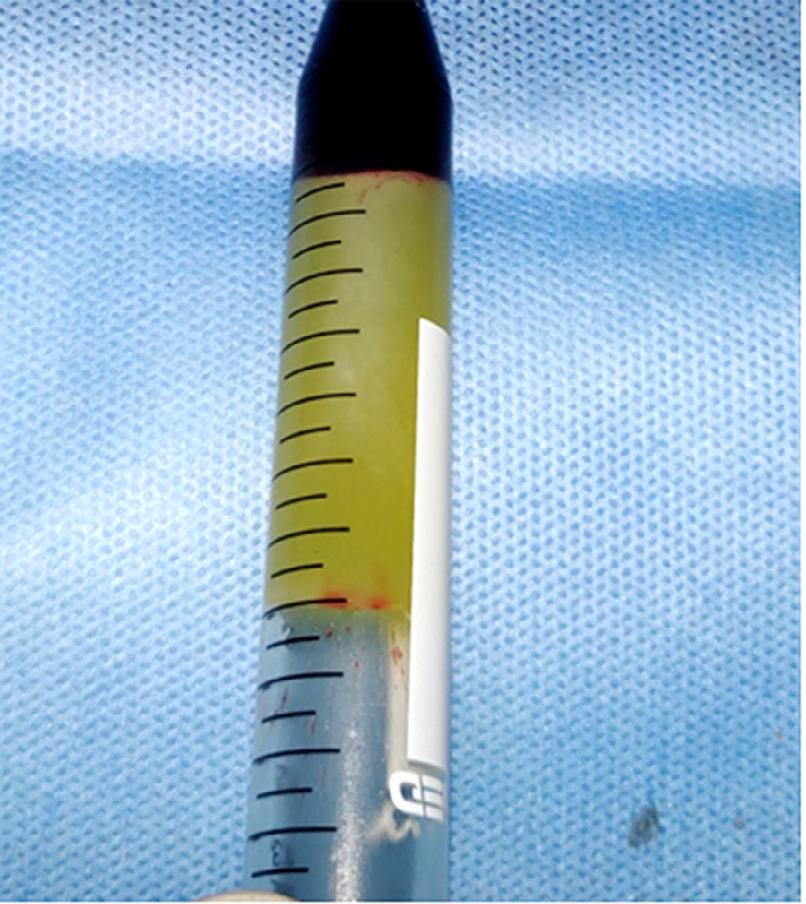
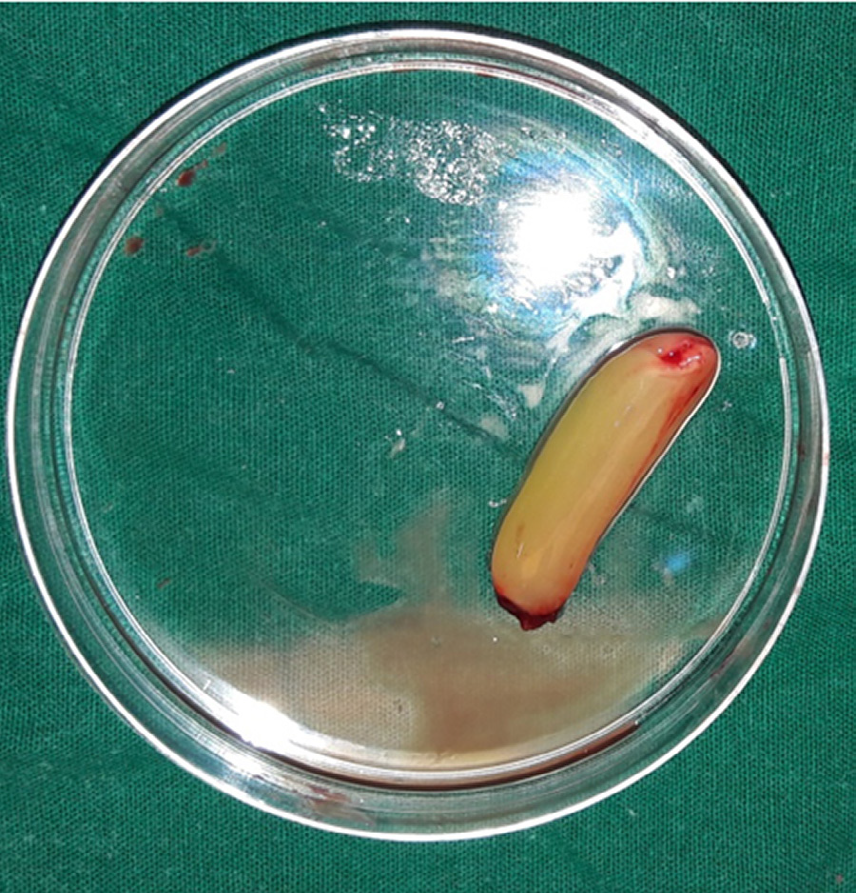
Wound bed preparation was planned for the patient’s wound over the scalp with Platelet Rich Fibrin Matrix (PRFM). Under strict aseptic precautions, ten ml of venous blood was drawn, added to a sterile centrifugation tube devoid of anticoagulant. Centrifugation was done at 3000 rpm (approximately 400g) for 10 minutes. Three layers were obtained: upper straw coloured platelet poor plasma (PPP), red coloured lower fraction containing red blood cells (RBCs) and the middle fraction containing the PRFM (Figure 2). The upper straw coloured layer (PPP) was discarded. PRFM was separated from red corpuscles at the base using a sterile forceps and scissor, preserving a small RBC layer measuring around one mm in length (Figure 3), which was transferred onto a sterile gauze. The PRF was transferred to the raw area Figure 1 and covered with a sterile dressing. Two sittings were done one week apart and the wound bed was reassessed 2 weeks. The wound showed healing as evidenced by healthy tissue (Figure 4).


Discussion
Burn injury is a major cause of trauma to the human body, causing death as well as disability, with a long healing period and high cost in hospital treatment. The mortality rate of burn injury has decreased with new treatment modalities, but secondary infections and prolonged healing periods still affect the mortality rates. Early debridement and skin grafting have been successful, but insufficient graft donor area and poor patient circumstances for surgery hinder skin grafting. In these circumstances, using products that would increase the wound healing process can be used. For this purpose, different kinds of dressings and pharmacotherapies have been developed, but most are costly, and the mechanisms underlying these therapies have not been fully documented. Wound bed preparation has emerged as a means of preparing the wound to accept advanced wound healing measures. It has become clear that it may not be possible to treat a poorly prepared wound bed with advanced therapies. Wound bed preparation was redefined as the global management of the wound to accelerate endogenous healing or to facilitate the effectiveness of other therapeutic measures [1].
Wound bed preparation started to be summarized by the acronym T.I.M.E by June 2002 with T for tissue: non-viable or deficient. I for infection/inflammation, M for moisture balance. E for edge. Debridement, control of inflammation and moisture are essential parts of wound bed preparation that may stimulate the edge of the wound to migrate, but if they fail, advanced therapies is required. Platelets play a crucial role in haemostasis [2] and also in the wound healing process. Platelets release a variety of cytokines as well as growth factors [3], which control and enhance the migration, proliferation, and functions of keratinocytes, fibroblasts, and endothelial cells. Chronic wounds stall in the inflammatory phase of healing. They lack the growth factors and do not heal. Platelet derived autologous products, platelets rich fibrin (PRF) and platelet rich plasma (PRP) are a rich source of growth factors. The application of platelet rich derived therapies is useful in this regard.
Fibrin is the active form of Fibrinogen [4]. Fibrinogen is transformed to insoluble fibrin by thrombin with role in platelet aggregation. Platelet concentrates lacking coagulation factors, termed platelet rich fibrin (PRF) was developed for its anticipated properties in tissue regeneration and wound healing. During centrifugation, fibrinogen gets concentrated in the upper part of the tube and combine with thrombin to form a fibrin clot. There is release of growth factors from PRF. The release of these factors commences 5 - 10 mins after clotting and continues for at least 60 - 300 mins, provides slow sustained release [5]. PRF is made of a fibrin matrix gel polymerized in a tetra molecular structure, with platelets, leucocytes, cytokines, and circulating stem cells [6]. PRF has few distinct advantages over PRP. The technique of PRF preparation is simpler, involves minimal handling, and not dependent on anticoagulation thrombin activator. The consumables required are easily available in a hospital. Further, the gel form of PRF is easy to apply on raw area compared to the liquid formulation of PRP [7]. The effects of PRF are due to factors of healing that act in complex synergy, such as leukocytes, fibrin matrix, and circulating progenitor cells. The activity of the autologous growth factors along with biomechanical stiffness of plasmatic proteins after fibrin mesh formation offer a unique architecture that is favorable to healing process. The growth factors released from the alpha granules of activated platelets, and factors such as fibrin, fibronectin and vitronectin play pivotal role in tissue repair and regeneration. These growth factors include vascular endothelial growth factor (VEGF), fibroblast growth factor-b (FGF-b), PDGF, hepatocyte growth factor (HGF), EGF, and angiopoietin-I (Ang-I) among others [8]. This is a preliminary study to assess the usefulness of PRF injection in management of electric burns. It therefore helps in the wound bed preparation. More long term clinical study are needed to determine whether PRF can be used for wound bed preparation in electric burns. This was done on a single patient and needs large population based study to apply in practice.
Conclusion
Platelet rich fibrin matrix is an effective tool in the management of electrical burn.
References
-
Falanga V (2002) Wound bed preparation and the role of enzymes: a case for multiple actions of therapeutic agents. Wounds 14: 47-57.
-
Choukroun J, Diss A, Simonpieri A, Girard MO, Schoeffler C, et al. (2006) Platelet-rich fibrin (PRF): a second- generation platelet concentrate. Part IV: clinical effects on tissue healing. Oral Surg Oral Med Oral Pathol Oral RadiolEndod 101(3): e56-60.
-
Zhao L, Lian L, Suzuki A, Stalker TJ, Min SH, et al. (2015) Platelet Pitp-Alpha Promotes Thrombin Generation and the Dissemination of Tumor Metastasis but Has Minimal Effect on Vascular Plug Formation. Blood 126(23): 418- 418.
-
Mosesson MW (2005) Fibrinogen and fibrin structure and functions. J ThrombHaemost JTH 3(8): 1894-1904.
-
Dhurat R, Sukesh M (2014) Principles and Methods of Preparation of Platelet-Rich Plasma: A Review and Author’s Perspective. J Cutan Aesthetic Surg 7(4): 189- 197.
-
Choukroun J, Diss A, Simonpieri A, Girard MO, Schoeffler C, et al. (2006) Plateletrich fibrin (PRF): A second- generation platelet concentrate. Part IV: Clinical effects on tissue healing. Oral Surgery, Oral Med Oral Pathol Oral Radiol Endodontology 101: e56-e60.
-
Nishimoto S, Fujita K, Sotsuka Y, Kinoshita M, Fujiwara T, et al. (2015) Growth Factor Measurement and Histological Analysis in Platelet Rich Fibrin: A Pilot Study. J Maxillofac Oral Surg 14: 907-913.
-
Anitua E, Pino A, Orive G (2017) Opening new horizons in regenerative dermatology using platelet-based autologous therapies. Int J Dermatol 56(3): 247-251.
- Reconstruction of Nasal Defect Using a Local Flap Based in the Nanoperforants Concept: A Case Report
- Transplant Tourism in Japan: Insights from Nationwide Surveys and Emerging Ethical Challenges
- The Challenge of Peritoneal Vaginoplasty in Transgender Women: Review Literature and Personal Perspectives
- Algorithmic Paternalism: Autonomy Versus Automation
- Dermatoscopy in Gorlin Syndrome: Avoiding the Disfigurement in Patients
- How Artificial Intelligence is Ushering in a New Era of Innovation in General and Plastic Surgery: A Short Communication