Integrated Treatment Protocol with Dorsal Sphincterotomy and Local Application of Seethodaka Thaila in the Management of Parikarthika (Chronic Fissure in Ano)-A Pilot Study
The causes of anal fissure are not fully understood, but junk food, change or irregularity in diet and diet timings and also sedentary life style are some predisposing factors of ano rectal disorders. Anal fissure is second most common disease seen in Ano-rectal clinics. Modern surgical techniques like manual anal dilatation is advocated for fissure in ano, but it weaken the internal sphincter associated with risk of incontinence. Hence the proper and effective therapy is required for the treatment of chronic anal fissure which is simple, safe and effective, without any complication, avoidance of incontinence of stool and recurrence. Seethodaka thaila is Sri Lankan medicated oil widely used for treatment of aseptic wounds, burns and post-surgical wounds in Ayurveda. Material and Methods: Ten patients of chronic fissure in ano were treated with seethodaka thaila local application for postoperative wound, after fissurectomy and dorsal sphincterotomy, daily for 4 weeks. Results: Post-operative fissure wound healed within 4 weeks of time duration. The patients got complete relief of sign and symptoms after four weeks and no recurrence till one year. Conclusion: On the basis of this Pilot study, it is concluded that dressing with seethodaka thaila followed by fissurectomy and dorsal sphincterotomy is effective in wound healing.
Introduction
Anal fissure is a longitudinal tear or disruption in the anoderm at the distal end of anal canal. It typically extends from below the dentate line to the anal verge and usually located posteriorly in the midline, probably because of the relatively unsupported nature and poor perfusion in that location [1, 2]. An anal fissure is second most common disease condition among ano rectal diseases, seen in an Ano Rectal Clinics (ARCs). In the present era, there is change or irregularity in diet and diet timings, sedentary lifestyle and also due to anatomical condition and manifestation of this Pilot Study disease take place. In addition to a change in diet & lifestyle and mental stress also disturb in digestive system which results in ano-rectal disorders.
Acute fissure in ano is a simple linear ulcer in the anal canal. In chronic stage, ulcer may become deeper, margins become indurate & thickened, due to repeated healing and ulceration when occurs constipation. There develops a typical sentinel tag at the distal end of fissure, simultaneously an anal papilla develops at the proximal end of fissure within the anal canal. Acute superficial break in the continuity of anoderm in mid posterior at 6 o’clock 90% or mid anterior at 12 o’clock position 10% is more common. Fissure in ano occurs most commonly in midline posteriorly. Anterior anal fissure is much more common in females, especially those who have borne children, childbirth leading to a damaged pelvic floor and subsequent lack of support of the anal mucous membrane. Fissure is more common in women than men. This disease condition is most common in middle age [3].
Parikartika is mentioned in Susruta chikitsa Sthana as one of the complication of virechana therapy [4] and improper usage of Vasti [5] while in Charaka Siddhi Sthana as atisara vyapad [6, 7, 8]. In Kashyapa Samhita, the similar condition is mentioned in pregnant women and classified as Vataja, Pittaja and Kaphaja on the basis of Doshic profile [9]. Acharya Susruta describes as Vata & Pitta Dosha predominance condition. On the basis of symptoms of this disease, fissue in Ano can be compared with Parikartika in Ayurvedic classics. Similarly, secondary causes like Ulcerative Colitis, Crohn’s disease, Syphilis and Tuberculosis have also been held responsible for the formation of the disease fissure-in-ano.
As mentioned above, this Thaila use for local application for new injuries, septic wounds, burns, fracture healing and in post-operative Ayurvedic surgeries [10]. This Pilot Study
Case History
aimed to evaluate the clinical efficacy of Seethodaka Thaila local application in the management of post-operative wound healing, followed by fissurectomy and dorsal sphincterotomy. Seethodaka thaila which is help in promoting formation of healthy granulation tissue in less time and no complication of keyhole deformity seen after dorsal sphincterotomy.
Methodology
Dorsal Sphincterotomy
After spinal anesthesia, patient laid in lithotomy position and painting, draping was done. Excision of sentinel tag with fissure bed and also papilla was done if available. Then identified the internal sphincter through that excision and the internal sphincter was divided with electric cautery. After achieved haemostatic, wound packed with seethodaka oil and dressed.
Wound Dressing
From the day second patient was advised daily warm water sitz bath mixed with Pancha Valkala Kwatha. Then the post-operative wound was cleaned with NS (Normal Saline) and packed with Seethodaka taila by using sterile gauze piece. The dressing was done once daily for four weeks.
| Case No. | Age & Gender | Complains & duration | Site of Fissure | Presence of Papila | Presence of Sen. Tag | Diagnosis | Anaesthesia |
|---|---|---|---|---|---|---|---|
| 1 | 40years Male | Pain & Burning since 3/12 BPR as drops-2/12 Constipation on/off -since 4ys | 6 o’clock position | No | Yes | Acute on Chronic Fissure | Spinal |
| 2 | 42years Female | Pain & Burning 1y BPR as streak 6/12 Constipation on/off -since 6ys | 6 o’clock position | Yes | Yes | Acute on Chronic Fissure | Spinal |
| 3 | 38years Male | Pain & Burning,1/12 BPR as drops -1/12 Constipation - 3ys | 6 o’clock position | No | Yes | Acute on Chronic Fissure | Spinal |
| 4 | 40years Male | Pain & Burning,3/12 BPR as streak-3/12 Constipation on/off -since 5ys | 6 o’clock position | Yes | Yes | Acute on Chronic Fissure | Local |
| 5 | 49years Male | Pain & Burning 9/12 BPR as drops 3/12 Constipation 1y | 6 o’clock position | Yes | Yes | Acute on Chronic Fissure | Spinal |
| 6 | 35years Female | Pain & Burning 3/12-5/12, No BPR Constipation 6/12 | 6 o’clock position | No | Yes | Chronic Fissure | Spinal |
| 7 | 30years Female | Pain, Burning & BPR drop wise since 15days Constipation 2ys | 6&12 o’clock positions | No | Yes | Acute on Chronic Fissure | Spinal |
| 8 | 34years Male | Pain & Burning1/12, BPR as drops 10days Constipation 4-5ys | 6&12 o’clock positions | No | Yes | Acute on Chronic Fissure | Spinal |
| 9 | 32years Female | Pain, Burning & BPR on/off as streak, since more than 1yr. Constipation 7ys | 6 o’clock position | Yes | Yes | Acute on Chronic Fissure | Spinal |
| 10 | 30years Female | Pain & Burning, since 3weeks, BPR since 2weeks Constipation 2ys | 6 o’clock position | No | Yes | Acute on Chronic Fissure | Local |
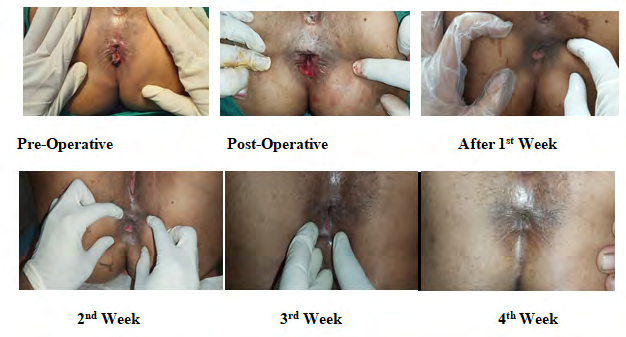
Observation of the Wound
Case No 01

Case No. 02
Case No. 03

Case No 04
Case No 05

Case No 06
Case No 07
Case No. 08

Case No. 09
Case No. 10
Assessment
The assessment of the wound was done on the basis of subjective parameters i.e. Pain and Burning as gradation and objective Parameters as Oozing and Healing of the wound at weekly intervals till four weeks. Eranda brusta harithaki churna 5g after meal at bed time as laxative was advised during the treatment for all patients.
Discussion
Out of those patients 100% were vegetarian. It doesn’t mean that patients who are taking vegetable diet are more prone to this disease condition. But it is related to spicy food and the persons who take more chillies, spicy as well as more oily food are more prone to develop Fissure in ano. In chronic fissure in ano when there is development of acute pain due to acute tear/ulcer at ano-derm. Patient usually takes medication & it heals spontaneously. But due to reoccurrence which is due to incomplete healing of fissure and sphincter spasm again patient had severe pain in ano during defecation.
Speciality accoding to Kashyapa Samhita, pain is the predominant character of this ailment. Burning also associated with the Pitta involvement. But the rarely presence of Kaphaja symptoms also seen as itching at peri-anal region is one of the symptom, sometimes due to discharge. This disease does not give very marked changes in the blood picture. Therefore, the progress seen in these cases, repeated blood examination during the course of treatment also is insignificant. Most of ancient Samhitas have mentioned Parikarthika is a complication of Virechana or basti therapy, if not done by expert physician. But practically found that excessive Virechana or improper use of basti is not the only causative factors of this disease. Out of theses 10 cases any of the patient did not give any history of either of therapeutic purgation or recent use of enema. All of the cases in this series suffered from habitual constipation and often passed hard column of stool that lead to injury at ano-derm. So after sphincterotomy the dorsal potion of sphincter is divided then there is no spasm. So healing of ulcer takes place and recurrence was not noted till one year in this study but reported minimum cases [11]. In dorsal sphincterotomy study, reported that if there is development of keyhole defect that leads to sometime recurrence [12]. In lateral sphincterotomy some part of internal sphincter is not be divided as it is blind procedure and pain may persist in some cases [13].
But in this Pilot study none of patient found with keyhole defect because after dorsal sphincterotomy the wound was taken care with local application of seethodaka thaila which is effective for wound healing & that healing fissure achieve good tensile strength [14]. Ayurveda oils are usually helpful to provide nutrition to the cell along with healing effect. Daily warm sit bath with pancha valkala kwatha is helpful for cleaning and all ingredients process kashaya predominant property, so helpful as Vrana shodhana [15, 16].
The healing of fissure is different from the healing of any other ulcer in the body, because in the former, there is constant contamination of the wound by faeces and its frequently friction with the mucosa while there is continuous spasm of the sphincteric muscle. They are the important factors which keep a fissure away from normal healing. In such situation a drug which produces a soothing effect, vata-pittahara, vedana sthapana, vrana shodhana and vrana ropana influences reduction of inflammation will be more suitable than a simple conventional antiseptic oinment. Seethodaka Thaila probably have these properties. Its well- known fact that the Vata and Pitta Doshas are predominant in Fissure in ano. Seethodaka Thaila is probably having anti- inflammatory and steroidal activity counting for its increased efficiency. The relief of severe pain within 24-48 hours is something remarkable about this drug although the ulcer takes as few days as three to four weeks for complete healing.
Conclusion
Study concluded that integrated approach in chronic fissure with dorsal sphincterotomy and local management with pancha valkala kwatha warm sitz bath and seethodaka thaila local application is good treatment protocol. Limitation of the study needs to be trial in more number of patients for its scientific validation. On the basis of these ten cases that complete healing of the post-operative wound within 4 weeks of time after local application of Seethodaka Thaila, no recurrence was noticed during the follow up period of 1 year. Hence the drug is safe, easy to apply and well tolerable in patient of chronic fissure for post-operative wound healing.
References
-
Russell RCG, Norman SW, Christopher JKB (2008) Bailey and Love’s Short Practice of Surgery 25th [Edn.], London: Arnold Publication, pp: 1251-1252.
-
Mapel DW, Schum M, Worley AV (2014) The epidemiology and treatment of anal fissures in a population-based cohort. BMC Gastroenterol 14: 129.
-
https://www.scribd.com/doc/27187148/Parikartika- Fissure-in-Ano-Defination-Parikartan
-
Shastri KA (2014) Maharishi Susrut, Susrut Samhita, Chikitsa Sthana, Vamana Virechana Vyapat, 34/16, Hindi commentary, by A.M.S, Chaukhamba Sanskrit Sansthan, Varanasi, pp: 187.
-
Shastri KA (2014) Maharishi Susrut, Susrut Samhita, Chikitsa Sthana, Anuwasana Uttara Vasti Chikitsa, 36/37, Hindi commentary, A.M.S, Chaukhamba Sanskrit Sansthan, Varanasi, pp: 196.
-
(2008) Agnivesha, Charaka , Dridhabla, Charak Sanhita, Siddhi sthana, Vamana Virechan Vyapada, 6/61, Chaukhamba Sanskrit Series Office, Varanasi, pp: 281.
-
(2008) Agnivesha, Charaka, Dridhabla, Charak Sanhita, Siddhi sthana, Vasthi Vyapad Siddhi, 7/56, Chaukhamba Sanskrit Series Office, Varanasi, pp: 305.
-
(2008) Agnivesha, Charaka, Dridhabla, Charak Sanhita, Siddhi sthana, Netra Vasthi Vyapad Siddhi, 5/5, Chaukhamba Sanskrit Series Office, Varanasi, pp: 251.
-
Tewari PV (2016) Maharshi Kashyapa, Acharya Vruddha Jeewaka, Kashyapa Sanhita , Khilasthan, Pregnant woman chaptor 09/10, 10/102.2-103.1 chcumbha Viswa bharati, Varanasi, pp: 565.
-
(2008) Ayurveda Pharmacopeia of Sri Lanka 1(1): 263.
-
Memon AS, Siddiqui FG, Hamad A (2020) Fissurectomy with posterior midline sphincterotomy for management of chronic anal fissure. J Coll Physicians Surg Pak 20(4): 229-231.
-
Yüksel O, Bostanci H, Leventoğlu S, Sahin TT, Menteş BB (2008) Keyhole deformity: a case series. J Gastrointest Surg 12(6): 1110-1114.
-
Madalinski MH (2011) Identifying the best therapy for anal fissure. World J Gastrointest Pharmacol Ther 2(2): 9-16.
-
Ayurveda Pharmacopeia of Sri Lanka 1(1): 263
-
Khadkutkar DK, Kanthi VG, Dudhamal TS (2016) Antimicrobial Activity of Panchavalkal Powder and Ointment. International Journal of Medicinal Plants and Natural Products (IJMPNP) 2(1): 9-15.
-
Dhurve VA, Dudhamal TS (2020) Formulations of Panchavalkala As Vrana Shodhana and Vrana Ropana: A Brief Review. Indian J Ancien Med Yog 13(1): 17-22.
- Management of Ear Keloid with Ksharsutra: A Case Study
- Yoga and Global Sustainability: A Holistic Path to One Earth, One Health
- Autoimmune Diseases in Ayurveda: A Narrative Review with Classical and Modern Perspectives
- Management of Cluster Headache Associated with Pituitary Apophysitis by CERT (Chakrasiddh Energy Release Technique): A Case Report on Energy Rebalancing
- Zygophyllum Geslini Coss : Biochemicals and Antioxidant Activity
- Observations of a Beginner Vaidya