Accessibility to Medicines in Khartoum State, Sudan
Problem Statement: High medicines prices and unavailability of vital items in all medicine outlets of Khartoum State denied patients from getting one aspect of their basic human rights, health services. However, investigating, determinants of such phenomena and presenting information to policy makers would help to take measures that make medicines available at affordable prices. Methods: Thirty private pharmacies, thirty public outlets and eighteen non-governmental organization pharmacies and twelve private hospital outlets were visited to check medicines prices and availability. The documents of the national medicines procurement agency were reviewed. The director of the state procurement agency, three managers of pharmaceutical enterprises and the director of the national medicines and poisons board were interviewed. Key Findings: The public sector procured lowest-priced generics LPGs and originator brand OB products at 0.86 times and 1.27 times the International Reference Price. Availability of OB and LPG medicines was 3.4% and 71.4% in public sector while in private sector the availability of OB and LPG medicines was 17.9% and 83% respectively. In the public pharmacies patients paid 2.55 times and 1.92 times the International Reference Prices respectively while in private retail pharmacies LPGs and OB medicines were sold to patients at 3.01 times and 15.87 times the International Reference Price. Conclusion: Both availability and patient prices of medicines in private sector pharmacies were higher than the availability and patient prices in public sector pharmacies. Patient prices in private sector in Sudan were higher than those in Eastern Mediterranean Region Organization countries.
Introduction
Access to affordable and assured quality medicines is one crucial element for achieving goals of health care system as envisaged to improve population health status, respond to their expectations and protect them from financial losses (The world Health Organization WHO health report 1999a). In addition, utilization of health services is highly dependent on availability of Medicines. One third of the global population lacks access to needed medicines .The situation is even worse in the poorest countries of Africa and Asia, where 50% of the population lacks such access [1]. In developing countries today because of high prices, medicines account for 25-70% of total health expenditure, compared to less than 15% in most high income countries [2]. Moreover up to 90% of populations in developing countries buy medicines through out-of-pocket payments due to lack of social insurance and inadequate publicly subsidized services [3]. Countries worldwide adopt pricing policies and/ or regulations with varying degrees of success to make medicines accessible to their populations. Still several countries are failing to implement policies and strategies to improve access to affordable medicines due to lack of technical capacity to analyze and interpret the relation between price data and local policies and to respond effectively to high prices or unusual price variations [4] Sudan is one of the poorest in the world with estimated GDP per capita income of US$ 1866 (World Bank 2011). Poverty prevailing across the nation with 46.5% of the population living below the poverty line according to the national definition of poverty (3.4SDG per person/day) [5]. Total health expenditure in 2010 US$3.755 million, total annual expenditure on health per capita (US$122) and total health expenditure was 6.2% of GDP [4]. Consequently the best-of opted to seek medical care in private sector while the worse-of who could not afford the cost of care in private sector either sell their asset to pay for medical care or abandon seeking treatment for their illness.Since1990 the government of Sudan adopted several policies and strategies to make medicines available at affordable prices in both public and private sectors. In early 1990s the government adopted cost- sharing mechanism for patients seeking health service at public sector facilities. However, emergency cases at hospitals were exempted from user fees as well as renal dialysis, immune suppressant medicines for renal implantation, chemotherapy, radiotherapy and treatment of hemophilia [6]. In 1996 the government established National Health Insurance Fund. It sought comprehensive coverage with predetermined benefit package to insurers who contribute through either deduction from their salaries or pay defined monthly premiums [5]. In 2005, National Ministry of Health updated the National Drug Policy NDP to become a guide for development, promotion and implementation of all pharmaceutical sector activities. The NDP promotes the essential drug concept and the use of Essential Medicine List for medicine supply in the public sector and for reimbursement purposes. In 2010 the National Medicines and Poisons Board adopted the External Reference Pricing method to regulate prices of imported and locally produced pharmaceutical products in both public and private sectors to ensure that medicines are of quality and at affordable prices [7]. In 2014 National Medical Supplies Fund NMSF enforced pooled purchasing mechanism which unified purchasing the needs of all public organizations for pharmaceutical products and consumables from NMSF. This mechanism ensures purchasing medicines through exercising economy of scale which lead to costs reduction [8].
General Objective
To measure prices, availability and affordability of medicines in public and private, NGO and private hospitals sectors.
Specific Objectives
To investigate prices and availability of selected medicines in private, public, NGO and private hospitals outlets in Khartoum State for period 20 November to 5 December 2014 To measure affordability of patients to buy medicines in Khartoum State for period 20 November to 5 December To compare prices in different sectors in Sudan with selected countries from African and EMRO regions
Materials and Methods
Cross-sectional survey to measure prices, availability, and affordability of medicines was carried out in Khartoum State health facilities. The study combined both quantitative and qualitative analytical methods. Key persons of medicine procurement and distribution in public sector and private sector were interviewed and procurement data of the national procurement agency were reviewed to collect qualitative dat. The quantitative data was collected by the survey tool for documenting medicine prices in 90 public, private, NGO and private hospitals outlets in Khartoum State using HAI/WHO methodology. A data of 50 items were chosen from HAI/WHO core list plus supplementary medicine list added for their local importance. For each selected medicine in specific dosage form and strength, two products were monitored; *Originator brand OB: the original patented pharmaceutical product. *Lowest price generic equivalent LPG, the lowest price generic product in the facility at the time of visit. In order to calculate affordability of standard treatments for common conditions, a cost of therapy exceeding one day’s wage of the lowest-paid unskilled government worker was considered unaffordable. Data
analysis was processed by MS Excel work book developed by HAI/WHO.
Study Instrument and Tools
Three different types of instrument and tools were
- Standardized questionnaire form developed by HAI/WHO
- In-depth interview with key informants
- Document reviewing Operational definition of variables The following are the variables used in the study
- Dependent variables: price of medicines, median price ratios, percent availability, affordability
- Independent variables: Pricing policy, pooled procurement, Generic competition, Exchange rate, patent status Data management and statistical analysis
- Descriptive statistics: , affordability, prevalence of generic medicines
- Inferential statistics: percent availability, median price rations, percent of originator brand medicines in public sector, procurement price for public sector
Results
The price data are not presented in local currency units but, rather, medicine price results are expressed as Median Price Ratios MPRs calculated using International Reference Prices IRP (Figure 1). Reference prices are internationally available list of prices against which the local prices are compared by means of a ratio where: Median Price Ratio (MPR) =median local unit price/median international reference unit price The ratio is thus an expression of how much greater or lesser the local medicine price is than the international reference price e.g. an MPR of 2 would mean that the local medicine price is twice that of the international reference price (Tables 1 & 2). Median price ratios facilitate cross-country comparisons of medicine prices.
All: the number of medicines available during the visit (OB&LPGs) EML: Essential Medicines List OB: Originator Brand LPGs: Lower Price Generics
| Product Type | Public Sector (n=30 | Private Sector (n=30 | No. of Medicines in | % Difference Private | |||||||||
| outlets) | outlets) | both Sectors | to Public | ||||||||||
| OB | 1.92 | 2.41 | 3 | 25% | |||||||||
| LPG | 2.55 | 3.01 | 49 | 18% |
Table 1: Comparison of public sector patient prices to private sector patient prices. OB: Originator Brand LPG: Lower Price Gener
| Public Sector | Private Sector | NGO Sector | Private Hospitals | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Patient & Treatment | ||||||||||||||||||
| OB | LPG | OB | LPG | OB | LPG | OB | LPG | |||||||||||
| Father- Metformin | 1 | 3.8 | 1.4 | 3.8 | 1.3 | 3.8 | 1.6 | |||||||||||
| Child-Isophane insulin | 3 | 3.5 | 3.2 | 3.7 | ||||||||||||||
| Mother-Azithromycin | 1.2 | 1.2 | 1.2 | 1.8 | ||||||||||||||
| Total days' wage for tx | 5.2 | 6.1 | 5.7 | 7.2 |
Table 2: A affordability of treatments for a family with diabetes and upper respiratory infection: Number of days ‘wage of the lo
Discussion
Access to health care, including essential medicines is a fundamental human right. Realization of such right call for coordination and collaboration of various actors for financing and provision of health care services.
Availability of Medicines in the Public Sector
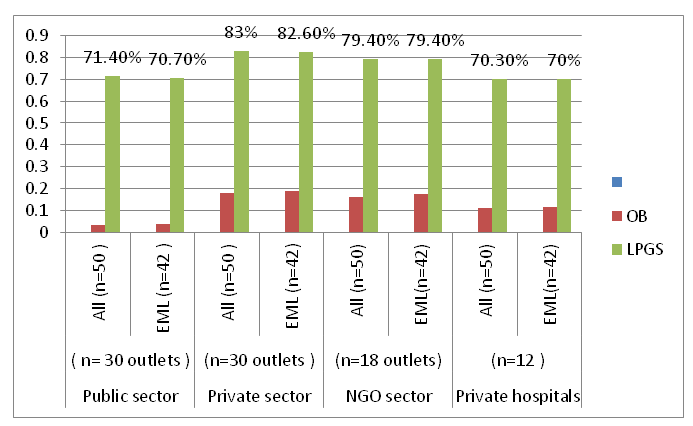
Availability was calculated by the percentage % of facilities where individual medicine was found. It is worth noting that the availability data only refer to the day of data collection at each particular facility and might not reflect average monthly or yearly availability of medicines at individual facilities. Overall public sector availability was 71.4% and 3.4% for lowest priced generics and originator brands respectively. The mean availability for essential medicines was 70.70% in the public sector. These findings were consistent with the results of a previous survey carried out in Sudan in 2013 which showed percent availabilities of 3.7%, 68.1% and 68.2% for OBs, LPGs and EML respectively in the public sector [9, 10, 11]. The possible explanation of high availability of LPG medicines against OB medicines in public sector facilities is: that most public sector outlets surveyed were affiliated to RDF- Khartoum State which due to adherence to national essential medicines list and national treatment guidelines where only generic medicines were encouraged for efficiency criterion. In addition, most public sector outlets in the different levels of health care system stock the essential medicines which were the bulk of the LPG medicines surveyed . It also worth mentioning that in the public sector when generic medicines of assured quality were available, the availability of originator brands was not of concern. The positive finding is the availability of LPG hypo tensors amlodipine, atenolol, furosemide, lisinopril and losartan was very good in all public facilities. These help patients with insurance benefits to get their treatments at affordable price. Availability of medicine for other chronic diseases such as diabetes and asthma was also very good. Clopidgrel was not available at any of public sector outlets surveyed which may be because of the fact that it has been recently removed from reimbursement list of the Social Health Insurance Fund .Antipsychotic lamotrigine and olanzapine were also unavailable in any of public sector outlets surveyed. The unavailability of these three items in the public sector facilities could have direct implications on access to medicines as patients are then forced to buy these medicines from private pharmacies with high prices. Many antibiotics of different classes and strengths were available at primary health care outlets indicating well controlling of infectious diseases at the first level of health care system .The availability of medicines that are listed in essential medicines list for primary health centers were penicillin benzyl 73.3%, chloramphenicol eye drop 60%, amoxicillin cap 100%, co- trimoxazole suspension 70% and Metronidazole 76.7%. Other second and third generation antibiotics which were not listed in the essential medicine list for primary health care level but were found at primary health centers, ceftriaxone 73.3% and ciprofloxacin tab 90% Comparing results of this survey with previous survey results carried out in 2005 [12], the availability of originator brands was decreased in public sector and private sector alike but availability of LPGs was increased in both sectors. This may be due to shortage of hard currency assigned by Central Bank for pharmaceutical private enterprises to import medicines [13]. In addition pooled procurement system launched by NMSF in 2014 also had direct effect on enhancing availability of generic medicines in public sector facilities.
Availability of Medicines in the Private Sector
Availability is much better in the private retail pharmacies with the median availability of 17.9% and 83% for OB and LPG medicines respectively .This result also consistent with results of previous survey conducted in Sudan in 2013 [11]. Medicines for treatment of hypertension were more available in the private pharmacies than in public pharmacies. The availability of LPG captopril was low 63.3% but that of LPG lisinopril 93.3% and LPG losartan 96.7% was good perhaps owing to the shift of the prescribers to newer ACE inhibitors. Availability of LPG medicines for other chronic diseases was also good, metformin 93.3%, glibenclamide 100%, but mental illness treatments showed poor availability lamotrigine 53%, olanzapine 73.3%. Interestingly, OB salbutamol inhaler availability 83% was higher than availability of LPG equivalent 70%, indicating that private pharmacies stock originator brands to benefit from brand premium the anti-malaria artesunate and artemether injection were fairly available in both private as well as public sector outlets indicating need-based availability since malaria is widely prevalent. Similarly the availability of antimicrobials was good in both sectors. The availability of 78% of LPG medicines in the private pharmacies surveyed was above 76% indicating that private retail pharmacies always keep higher level of medicines availability than public sector does. This finding strengthening the crucial role of the private sector in patients’ accessibility to medicines in Khartoum State
Public Procurement Prices
Procurement price data was found for 42 medicines in 2011/2013 tender sheet. Of these medicines 37 (88%) out of 42 were from essential medicines list which stressed the adherence to Essential Medicines List and standard treatment guidelines .Only five originator brands were found in the 2011/2013 tender list likewise this result also consistent with the national medicine policy which call for procuring medicines of assured quality from countries with effective control systems. Based on 2013 MSH Reference Price, National Medical Supplies Fund procured generics at 1.27 times their International Reference Price IRP and originator brands at 0.86% times their IPR. The latter figure was below the acceptable level of MPR<1 as suggested by HAI/WHO. Thus NMSF has efficient procurement system. The former finding clearly showed the impact of tender system on decreasing medicine prices. Previous studies conducted in 2012 and 2013 using HAI/WHO methodology showed median MPR for LPG medicines were 1.2,times and 1.83 times respectively [11, 14]. The potential explanation of higher MPRs of generics than the MPRs of the originator brands owned to restricted tender system conducted by NMSF to encourage the national pharmaceutical manufacturers whom their medicines prices were not internationally competitive. Thus too low prices sought by NMSF tender system could result in problems of quality or/ and development of the national pharmaceutical in future. Median MPR for individual medicines shows 37 medicines 88% out of 42 items procured by NMSF in 2011/2013 tender had prices below the international reference price and only five medicines had prices higher than international reference price of one , artesunate 8.5 times, azithromycin 1.18 times, ceftriaxone 1.57 times, Clopidgrel 8.58 times, insulin isophane 1.25 times.
Public Sector Patient Prices
It is worth mentioning that the international reference prices are bulk procurement prices for not for profit and/or for profit suppliers/buyers prices, not retail prices. Therefore public procurement prices may be fairly close to international reference price but patient prices across public, private, NGO or private hospitals are likely to be considerably higher due to the charges and profits added on to the procurement price of a medicine as it proceeds through the distribution system. Overall, patients paid 2.55 times and 1.92 times the reference prices for generics and originator brands respectively in the public outlets. These findings were consistent with studies carried out in Sudan and other neighboring countries. Generic medicines with low MPR in public pharmacies were artemether inj, allopurinol, atorvastatin, gliclazide and lisinopril. If we consider MPRs of less than 5 times as reasonable. Out of the 49 generics analysed, 10 had MPRs greater than 5times.Three originator brands were found in public outlets surveyed. Two out of the three had reasonable MPRs, OB Insulin isophane 1.63 times and OB salbutamol inhaler 1.92 times but OB glimepiride had exorbitantly high MPR of 31.75 times the IRP. The prices of OBs in the basket varied from 1.63 times to 31.75 times. This means that for some medicines patients’ price were moderately cheap but most of them were very expensive with prices up to 31 times the international reference price Forty nine LPG products (98%) were found in the public sector surveyed indicating adherence of public sector to essential medicines list. Fifty percent of the LPGs were priced at 1.44 (25TH percentile) to 4.2 (75TH percentile) times their IRP; thus; there is moderate variation in MPRs across individual LPG products in the public sector outlets. These findings were consist with previous studies carried out in Sudan [11, 14].
Private Sector Patient Prices
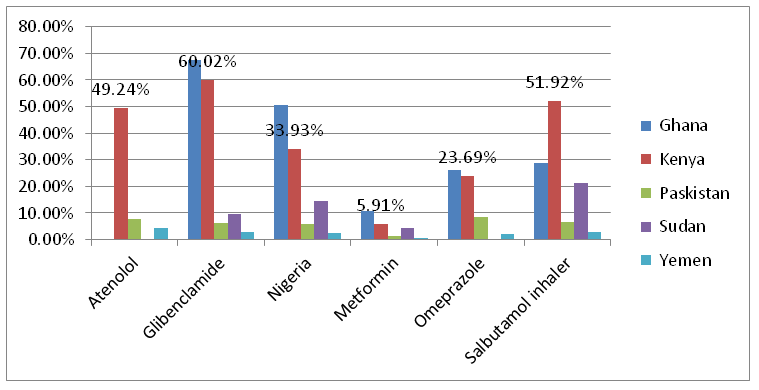
In 30 private pharmacies surveyed, LPGs and OBs were sold to patient at 3.01 times and 15.87 times the international reference price respectively. Earlier survey conducted in Sudan in 2012 had also shown similar prices of medicines in the private sector pharmacies [15]. Generic medicines with low MPR in private pharmacies were artemether inj, allopurinol, atorvastatin and lisinopril. Generic medicines with high MPR were acetylsalicylic acid 8.5 times, carbamazepine 8.68 times and acyclovir15.16 times. The latter medicine had few competing products in the market that may push to make it of reasonable price for patients Overall, originator brands were very expensive in the private pharmacies and were nearly six times the price of the LPGs. Despite the availability of generic equivalents patient price of some originator brands were extremely high compared to reference prices, for example, OB atenolol 25.94 times, OB Clopidgrel 38.15 times, OB furosemide 54.47 times, O glibenclamide 23.69 times, and OB glimepiride 31.75 times. The high prices of medicines in resource-poor settings like Sudan can substantially restrict access to them especially as 65% of populations spend out-of- pocket for their medical care [16].
Inter-Sectors Patient Prices
Several factors made medicines prices varied such as the sector in which they are purchased, the type of the procurement agent, the distribution route and the patent status. This survey showed large differences in the prices of the same generic substance between the public pharmacies and the private pharmacies; the patients paid 18% more when purchasing their LPG medicines from private pharmacies. The low price of generic medicines in the public pharmacies was owning to bulk procurement prices that passed on to patients. The difference between patient price in private pharmacies and public procurement price was huge. For example the procurement price of OB salbutamol inhaler at National Medical Supplies Fund NMSF was SDG 20 per bottle while some private pharmacies were charging between SDG 31.7 and SDG 35 per bottle meaning that the increment was up 75%. This price variations indicate poor compliance of private pharmacies with official price regulations set by NMPB. Wider difference in prices between originator brands and their generic equivalents was noted; patients paid 25% more for OBs from private pharmacies. The minimum and maximum prices for originator brand medicines in the basket varied from 1.87 to 54.47. In addition, the variability of 25th and 75th MPR percentiles was high recorded as 5.11 and 25.94 respectively. This means that different prices were assigned to the same product. In Sudan, a pricing mechanism has been built into the registration system as a routine administrative exercise from the very beginning of medicine registration [17].
International Medicine Prices Comparison
Prices of medicines varied across countries. The public sector procurement prices for Sudan were around 45.3% higher compared to other neighboring countries. The median procurement price for LPG for Sudan was found to be 1.27 times the international reference price IRP compared to 0.55 times, 0.61 times, 0.67 times and 0.78 times the IRP for Kenya, Ethiopia, Tanzania and Uganda respectively [15, 16, 17, 18]. The private sector patient prices for originator brands for Sudan, as illustrated in Figure 2 show medicines prices in Sudan were higher than prices of medicines in Pakistan and Yemen as an example from EMRO countries. This finding was consistent with results of previous studies conducted in Sudan [14, 19, 20, 21]. However, private patient prices for originator brands in Sudan where lower than those of Kenya, Ghana and Nigeria.
Assessment the Affordability of Standard Treatment Regimens
The affordability of treatments for common conditions was calculated as the number of days’ wages of the lowest-paid unskilled government employee needed to purchase medicines prescribed at a standard doses. The daily wage of the lowest paid unskilled government employee was 15 SDG (US$ 2.3). In 1992, the government of Sudan adopted a user fees policy in an attempt to improve the accessibility to health services including essential medicines in the public sector [7]. Unfortunately, all medicines might not be available at the time of the patient visit to a particular public health facility. Therefore, those seeking care in the public sector health facilities were very often end buying medicines from private pharmacies where the prices of medicines were higher than that of public pharmacies. The survey found out that the cost to the patient varied between public, NGO, private, and private hospitals sectors. The cost of medicines also varied between originator brands and generic versions. For example in the private pharmacies there were 5 fold differences between the price of originator brand lisinopril and its generic equivalent. With the exception of LPG metformin 500mg, LPG atenolol 50mg, LPG co-trimoxazole suspension and LPG artesunate 100mg, purchasing treatments for other medical conditions with OB or LPG medicines were unaffordable in the public sector. In general, data points showed more working days for patients who sought to purchase their treatments from private, NGO and private hospitals sectors than the public sector. In all medical conditions it was more expensive to be treated in the private sector facilities than public sector facilities, for example it costs three times more in the case of adult respiratory infection with LPG ceftriaxone 1g in private sector. For malaria treatment with artesunate100mg was the same in all sectors. In case of chronic conditions such as diabetes it was more expensive to be treated in the private, NGO and private hospitals sectors than public sector. For example LPG metformin500mg costs 1day’s wage, 1.4 days’ wage, 1.3 days’ wage, and 1.6 days’ wage in the public, private, NGO, private hospitals respectively. For treatment of hypertension with LPG lisinopril. It costs 2.3days wages, 3days wage, 2.8 days wages, 3.3 days wages in the public, private, NGO, and private hospitals respectively. For treatment of asthma with OB salbutamol inhaler. It costs 1.6 days ‘wages, 2days’wages, 1.6 days’ wages, 2.2 days’ wages in the public, private, NGO, and private hospitals respectively. However, consultation fees, diagnostic tests and other costs were not included in these prices. Moreover, previous studies showed that the average number of medicines per prescription in Sudan is about 2 in public health facilities and more than that in private clinics, Therefore the total treatment cost would be considerably higher than that calculated by this survey [22, 23]. When a family with a combination of three diseases conditions is considered, it was shown that the bread winner, who is unskilled lowest paid government employee, would need to work 5.2, 6.1, 5.7 and 7.2 days to purchase the necessary lowest priced generic medicines from public, private, NGO or private hospitals outlets respectively. Fortunately, the National Health Insurance Fund launched the strategy of comprehensive health service coverage and contracted with private pharmacies to provide medicines to beneficiaries which might help to increase accessibility to medicines for all citizens. It also pay claims for medicines unavailable at its point of services.
Conclusion
Availability of OB and LPG medicines was 3.4 % & 71.4% in public sector pharmacies versus 17.9% and 83% for OB and LPGs medicines in private sector pharmacies. Both availability and patient prices in private pharmacies were higher than the availability and patient prices in the public pharmacies. Patients paid 25% more and 18% more for originator brands and lowest priced generics respectively when purchasing their medicines from private pharmacies. High price differences were observed between originator brands and their generic equivalents in the private pharmacies. The price of originator brands were nearly 6 times the price of lowest priced generics. For the lowest paid unskilled government employee treatment for most common conditions was required more than one day’s wage with an exception of pediatric pneumonia with LPG co-trimoxazolesusp, malaria with LPG artesunate 100mg, hypertension with LPG atenolol 50mg and diabetes with LPG metformin 500mg. Private sector patient prices for originator brand medicines in Sudan were higher than those in EMRO countries.
Study Implications and Recommendations
Rapidly rising costs of health care and high medicine prices are growing concern worldwide, especially in settings where patients often have to pay the full price of medicines. 43.2% was the share of government expenditure on health [24, 25]. Ironically, the dismal figure spent on hospitals instead of directing it to primary health centers to ensure availability of essential medicines to treat more people with the same resource allocation. The availability of generic medicines in the public sector was found to be lower than that of private sector. The pooled procurement policy launched by NMSF in 2014 will hope to enhance availability of quality assured generic medicines in public facilities. Some individual generic medicines were found with high MPR in public sector. The possible suggestion will be, the public sector should pass on low procurement prices to patients to improve access to more affordable treatments. With respect to private sector, the availability of generic medicines was good 83% because private pharmacies compete to save fairly high level of medicines stock to increase their market share and gain profit and because they also benefit from the NMSF strategy that providing chronic diseases medicine through the private sector at public procurement prices. These studies found out patient prices in private pharmacies were higher than that in the public pharmacies. Several options are proposed to address the higher prices of medicines in the private sector. First, promotion of quality assured generic medicines should be strengthening to doctors and patients alike. Second, enforcement of regressive mark- ups for medicines as cited in registered pharmaceutical products regulation since 2010 will incentivize pharmacists to sell generic medicines which have higher margins than originator brands 37% of Sudanese population have insurance coverage which indicate that the large part of the population have not insurance coverage [6]. Fortunately, the National Health Insurance Fund and other Insurance schemes have to accelerate the comprehensive coverage strategy to include those has not insurance service.
Study Limitations
The study has four main limitations that should be taken into account when interpreting the results. First, the scope of the study focus on prices of medicines and did not address macro-contextual factors that directly or indirectly influence prices or/and availability of medicines. Second, the study time was the day of data collection at each particular facility that might not reflect average monthly or yearly availability of medicines at individual facilities. Third, the reliability of median price ratios is dependent on supplies prices, in cases where there are no supplier price found, buyer price is used as a proxy, MPR results may be skewed by high/low international reference price. Finally, availability is determined for the list of medicines surveyed, therefore availability of other strengths, dosage forms, or therapeutic alternatives were not account for.
Contribution of the Findings
This paper investigate accessibility to medicines in Khartoum State, discusses critical areas of price concerns, provides a few suggestions to control charges on the supply chain of medicines and concludes by identifying the roles and responsibilities for various stakeholders to help making medicine prices affordable particularly for poor.
References
-
WHO (2004) WHO medicines strategy. 2nd (Edn.), World Health Organization.
-
WHO (2004) The World Medicines Situation. 2nd (Edn.), World Health Organization.
-
Mclntyre D, Thiede M, Dahlgren G, Whitehead M (2006) What are the economic consequences for households of illness and of paying for health care in low and middle-income country contexts? Soc Sci Med 62(4): 858-865.
-
Cameron A, Ewen M, Auton M, Abegunde D (2011) The World Medicines Situation. World Health Organization.
-
National Health Insurance Fund Sudan publication (2007) Dar Taiab Alasma publisher, Khartoum, pp: 26-30.
-
National Ministry of Health (2010) Annual Health Statistical Report 2010. Khartoum: National Health Information Centre, National Ministry of Health, Sudan, 2010.
-
Ahmed MY (2013) Medicine Prices. Availability and Affordability in Sudan.
-
National Health Insurance Fund (2003) National Health Insurance Fund Sudan Act.
-
Central Bureau of statistics. Statistical Report 1990- 2009. Khartoum: Sudan Central Bureau of Statistics, 2010.
-
Mohamed GK (2010) The Impact of the RDF on Accessibility of Medicines: Experience of Khartoum State- Sudan LAP Lambert Academic Publishing.
-
NMPB, Medicine Regulatory Authority in Sudan. The Registered Pharmaceutical products Regulation 2010.
-
Sudan National Medicines and Poisons Board (2014) Khartoum.
-
NMSF (2014) Pooled purchasing mechanism, National Medical Supplies Fund Khartoum: Sudan.
-
Alfadol KI (2005) Medicine price survey in Sudan.
-
Kheder SI (2014) Evaluating medicine prices, availability, affordability and price components in Sudan. 9(1): 1-12.
-
Ali GK, Yahia Y (2012) Controlling medicine prices in Sudan: the challenge of the recently established Medicines Regulatory Authority. East Mediterr Health J 18(8): 811-820.
-
Martin OO (2000) Uganda Medicine Pricing Survey Report.
-
Julius Ombogo (2004) Asurvey of Medicine Prices in Kenya.
-
NMPB (2014) Medicine Regulatory Authority in Sudan. Sudan Drug Index (2014) Khartoum: Sudan National Medicines and Poison Board.
-
Faris A, Tefera B (2005) Survey on prices of medicines in Ethiopia.
-
Justin Temu M, Damain F, Rimoy G, Mugoyela V, Mung’ong’o S (2004) Survey of Medicine Prices in Tanzania.
-
Kiani A, Qadeer A (2006) Prices, availability and affordability of medicines in Pakistan, pp: 1-33.
-
AL qubati YM, Al Awdy AM (2006) A survey Report on Medicine Availability, Prices and Affordability. Medicine Prices in Yemen, pp: 1-41.
-
Awad AI, HimadHA (2006) Drug-use practices in teaching hospitals of Khartoum State, Sudan. Eur J Clin Pharmacol 62(12): 1087-1093.
-
Abelmoneim IA, El-Tayeb IB, Omer ZB (1999) Investigation of drug use in health centres in Khartoum State, Sudan medical Journal 37(2): 21-26.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda