Fear, Reaction and Rational Behavior to Covid-19 in Public, Health Professionals and Policy Planners
THE COVID-19 ICEBERG: Being highly infectious disease, COVID-19 can spread exponentially but most of those infected remain asymptomatic or develop mild symptoms, thus may remain undetected. In fact, the majority of COVID-19 iceberg is made up of the dormant undetected cases forming the submerged part of the iceberg. The undetected cases of COVID-19 infection can be quantified through serological tests for presence of antibodies against the SARS-CoV-2 in a given population which form the basis of sero-surveys to provide crucial data. Age Groups and Perceived Covid-19 Threat: The millennials or Gen Y (women more than men) appear to be more fearful compared to other age-groups for contracting the infection. Whereas, the older generations (Gen X and older, Gen Alpha), are the most vulnerable but less afraid of the virus and the disease than millennials. Across the Generations, those belonging to the Gen Z are found to have least fear and low susceptibility. Fear and Other Reactions to Covid-19: Though case-counts and fatalities are been relatively higher in Europe and the US, as compared to most Asian countries, fear to the viral infection by residents of Asian countries including India was on higher side. Most of the respondents to global survey have been found to be fearful of contracting the infection. Apart from this, fears about the availability of essentials and access to various amenities afflict the susceptible populations. The key concerns by the healthcare professionals involve prevention from exposure to the infection, the adequate protection, and their personal and social support. Conclusion: Protecting Communities: The aphorism, prevention is better than the cure, fits the COVID-19, as presently there are no specific treatment modalities available. The fear may be the key to prevent the disease by using barriers like face masks and to practice social distancing. The lockdown measures enforced by various governments in countries around world work on basis of curtailing infection by distancing, isolation, quarantine measures. With the swift of growth of critically ill COVID-19 patients, it requires utilizing all clinicians within a medical center to significantly improve the critical care capacity. As the elective surgery and alike activities are cancelled or postponed, the hospitals become focused facilities for COVID-19 with all the medical and paramedical staff working for the cause.
Covid-19 Iceberg: Identifying Dormant Cases
The COVID-19 is highly infectious disease, but most of those infected are asymptomatic or develop mild symptoms, and thus remain undetected clinically. In fact, the total infected cases represent an iceberg with the apparent cases being those who are confirmed positive cases and the dormant undetected cases forming the major submerged part of the iceberg (Figure 1). These undetected cases of COVID-19 infection can only be quantified through universal test for presence of antibodies against the SARS-CoV-2 in a given population [1].
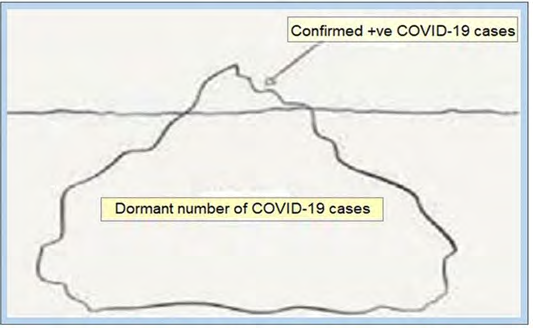
The serological tests to detect presence of antibodies in the blood can only establish a prior infection. The antibodies tests for the presence of SARS-CoV-2 antibodies indicating a previous infection are invasive tests through blood samples as compared to the non-invasive molecular tests, the swab tests, to determine the presence of the virus in a person’s airways to identify active infection. The swab tests do not identify if a person has been infected earlier with SARS- CoV-2 and recovered.
The serological tests analyse blood samples for two types of antibodies, anti-SARS-CoV-2 S protein IgG and IgM, using an ELISA (enzyme-linked immunosorbent assay) technique [2]. These tests are called sero-surveys and involve collection and analysis of mass blood samples to provide crucial data including the herd immunity for epidemiological models and help to outline the extent to which the nCoV-19 has spread undetected in the communities and populations. The data collected can also help to measure the impact of the enforcement measures like lockdown and public health efforts and form the basis and guide for planning the future prophylactic as well as treatment-oriented steps. A recent study led by the Pasteur Institute has reported that about 2.8 million people, 4.4% of the French population, have been infected by the SARS-CoV- [2, 3]. Another project, a Spanish study published on 12 May 2020, also documented similar findings, stating that about 5% of the country’s population has contracted the disease [4].
Fear and Other Reactions to Covid-19
The spread of COVID-19 pandemic is a major public health concern threatening people’s general and mental health and safety of life all over the globe. There are a number of studies for assessment and validation of the anxiety symptoms related to COVID-19 [5, 6]. It has been documented that though the number of cases and fatalities have been relatively higher in the Europe and the US compared to most Asian countries, the fear of the viral infection appears to be higher in residents of Asian countries including India, except Singapore, than various European nations and the US. In India, 62% of respondents to the survey stated that they were fearful of contracting the disease. The analysis is based on a large-scale global survey conducted by market research firm YouGov in association with the Institute of Global Health Innovation (IGHI) at Imperial College London [7]. The survey was initially started with eight Asia-Pacific countries in early in February 2020 and was extended to cover 26 countries by mid-March. The survey was run for over five weeks or more, planned to gather information about COVID-19, and aimed to offer an understanding about the people’s reactions to the pandemic spread of the virus and the measures taken by governments to contain it. The agency, YouGov has recently shared the data about views and behaviors of people around the world [8].
Another study involving general Indian population, found that the anxiety levels were high, in general. More than 80 % felt preoccupied with the thoughts of COVID-19 and 72% found the need to use masks and sanitizers, whereas 12.5% had sleep difficulties, 37.8% suffered from fear about acquiring the infection and 36.4% felt distress related social media [9]. A small study involved 263 participants, 106 males and 157 females with the mean age of 37.7±14.0 years, and 74.9% a high level of education. The mean IES (Impact of Event Scale) score to measure current subjective distress in the participants was 13.6±7.7 and it was concluded that the COVID-19 was associated with mild stressful impact in the sample, with the pandemic still ongoing [10].
Reaction to COVID-19 among Healthcare Professionals Assessment of the change in behavior and attitudes focusing on the healthcare providers’ concern about getting infected and related concerns in light of the Covid-19 pandemic was assessed using a structured questionnaire sent through an electronic medium like email or a chat-app like We Chat, Whats App, etc. It was found that the fear of getting Covid may outweigh other concerns as the hospitals were often regarded as COVID-19 infection reservoirs by general public as well as healthcare professionals. There was a large concern about the aerosolized spread of the virus through being exposed to coughing respiratory patients and aerosol-generating procedures, associated with the apprehension that they may not be able to maintain a safe social distance appropriately. Almost everyone expressed concern about screening and testing and measures taken once a patient screened positive to keep the remaining patients and themselves safe.
A study was done to examine the abnormality in mental health and explore their resilience and social support issues in Chinese health care workers dealing with the COVID-19 pandemic. Out of a total of 1521 health care workers, 147 had a prior emergency care experience while 1374 did not have. The results from the Symptom Check-List-90 (SCL- 90), Chinese version of Connor-Davidson resilience scale (CD-RISC) and Social Support Rating Scale (SSRS) showed that those without emergency care experience had inferior performance in mental health, resilience, and social support than others [11].
In addition, the anxiety and stress may also be caused by organizational factors and fear about resource shortages such as personal protective equipment (PPE) and protective masks are common, and concerns about not being able to provide competent care if deployed to a new area, about rapidly changing information and lack of communication, lack of specific drugs, the shortage of ventilators and intensive care unit beds necessary to take care for the surge of critically ill patients, and significant change in their own daily social and family life [12]. Some fraction of fear and anxiety is common but a severe degree of the symptoms were found in 2.2 % to 14.5% of all participants and the severity of symptoms was influenced by age and gender, and their role in healthcare and specialization and proximity to COVID-19 patients [13].
The COVID-19 Situation and Lockdown Measures
An analysis from a recent survey indicates that more than half of urban Indians think that the Covid-19 situation in the country is getting worse. Whereas, the remaining half believes that the situation will resolve in India in the next three months or a little longer. About 32% respondents think that it may take significantly longer, to wear off by the end of August to end of October 2020. A lower number of respondents anticipated to improve it both locally and globally, respectively 7% and 10%, till the end of the year [14].
In most countries, fear levels were stated to rise in response to the mounting case count and governmental efforts to contain the pandemic through lockdown measures, over the last few weeks. As schools and offices are shut down and the government has imposed mobility restrictions to complete lockdown, the fears in public appear to have accentuated. The increase in fear levels was relatively high in countries such as France, Australia, and the UK, where the proportion reporting high levels of fear nearly doubled after lockdown measures were introduced. The greatest shift in fear levels was in Sweden, where the number of people fearful of contracting COVID-19 infection rose from 7% to 46% during last few weeks.
The lockdown measures may have been authoritarian in some countries like China, whereas most of the countries across the world have promulgated softer versions reacting to public opinion and with idea of limiting the damage to economic activities. But, in general, the lockdown measures have generated fears about the availability of essential goods and access to various amenities. Following the lockdown, the people across the world, became worried about the availability of essentials items like food, medicines, and other supplies. Many, about 37%, feared about falling sick, whereas about 25% feared their likely handicapped access to health services. A significant number, about 20% expressed fear about losing their jobs and other vocation related issues. The survey also found that while approving of the government’s lockdown strategy, a significant number of citizens among various nations including Indians were fearful of the impact of lockdown on availability and quality of the essential services. The long-term psychological impact of the Covid-19 pandemic on front line health care workers has yet to be fully understood. However, health systems lack a practical model for providing mental health support to front-line staff engaged with the pandemic [8].
Age Groups and the Perceived Threat
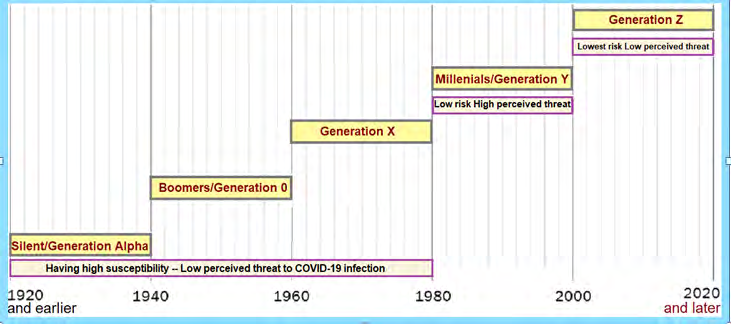
Generations or the age-groups are often considered by their periodic span along the timeline, though there is no agreed upon formula to define the length of the span. In general, those born between 1981 to 2000 can be called Millennials (witnessed the dawn of the Millennium) or Generation Y. The Generation X is born between 1961 to 1980, whereas the Baby Boomers, Generation O, are those born between 1941 to 1960. Those born between 1921 to 1940 form the Silent or Generation Alpha. Whereas, Generation Z (or Gen Z for short, or Zoomers) is the demographic cohort succeeding Millennials or Gen Y. Most members of Generation Z are born in the mid-to-late 1990s and the early 2010s, and most of the Gen Z have used digital technology since relatively young age and are comfortable with the Internet and social media, and are the successors of Gen Y.
Through the collected data, in the survey by YouGov [7] and the Institute of Global Health Innovation, it has been inferred that among the populations groups within India and elsewhere, it is millennials or Gen Y who appear to be most fearful to COVID-19 infection compared to other age-groups. Among the millennials in India, women were more scared of the infection than men [14]. Across Generations, those belonging to the Gen Z generation (post-millennial adults) were less scared than millennials. Even the older generations (Gen X and older, Gen Alpha), who are more vulnerable to covid-19 than millennials, were less afraid of the virus and the disease than millennials (Figure 2).
The Experience and Lessons in Covid Care
The Experience and Lessons from China
As we see in retrospective, the measures applied by the government and health care dispensed out have turned out to effectively and efficiently controlled the COVID-19 pandemic in China. At the community level in the affected areas, everybody was kept under quarantine, and strict social distancing and screening were enforced [15]. Similarly, stringent measures and triaging was applied for the hospitals and the care for non-Covid and Covid including the suspected patients was strictly bifurcated. The physicians, who were not designated to treat Covid patients, did not have contact with such patients. There were designated and well-announced medical facilities in the cities for Covid patients including the suspected ones, and the non-Covid medical units worked routinely and intensively screened their patients epidemiologically and symptomatically before being entered to the facility. In case, suspected, they were immediately sent to Covid-designated facilities.
Clinically, the doctors working in Covid units were well informed, and the communication from the government down to the physicians and to potential patients and to society was effective. There were clear clinical guidelines, which were updated constantly. There was a massive response from the physicians. The Covid facilities relied much on radiological findings and the CT scan was an early investigation even before a serological test was being done. Every person was assigned an electronic QR code that was to be updated every week.
During the initial phase of the COVID-19 outbreak in China, more than half of the 1210 respondents from 194 cities in China from general population rated the psychological impact as moderate-to-severe, and about one- third reported moderate-to-severe anxiety, with 53.8% of respondents rating the psychological impact of the outbreak as moderate or severe, 16.5% had moderate to severe depressive symptoms, 28.8% reported moderate to severe anxiety symptoms, and 8.1% suffered with moderate to severe stress levels [16].
In a limited survey of Chinese physicians involving 450 responders, the issue of fear of infection and reaction to the pandemic was noted. About 20% of the responders stated that they needed psychological support during that time. While about 50% of all the responders stated that they were afraid that they could be infected by their patients, they still continued working. On inquiring about considering leaving the medical profession or switching into being a medical professional in non-clinical settings, about 11% to 15% of physicians stated that they had those thoughts but did not make any steps toward it. On asking about the use of digital medicine and telemedicine, 45%, said that they see telemedicine as a good alternative in the future.
In general, the care of physicians and medical professionals during this outbreak has been high and strong. There have been measures to assure their health and protection. The physicians were well prepared and briefed about the disease. The panic and the mass hysteria that is being observed all around the world was not present in China and this has helped health care professionals to proceed systematically and consistently to succeed in terms of focusing on patient care. The lessons learnt from Chinese handling of the COVID-19 pandemic were importance of maximum of protection to healthcare professionals, more stress on radiological including CT scan than serological testing and recording epidemiological and clinical data to create a big data to be useful in future [17].
The Experience in European Countries COVID-19 Pandemic in Italy
Italy reported its first cases of COVID-19 on 31 January 2020. The Italian government reacted by declaring the state of emergency, quarantined the cluster areas, and lockdown. Italy being the first country in Europe to be hit by COVID-19, the lockdown of business and various services, anxiety and fear disoriented people [18]. The health professionals in Italy faced the threat of infection and encountered difficulties in protecting themselves. The unprepared Italian health system, having a modest number of ICU beds and few sub- intensive care beds about8.4 per 1,00,000 population, was handicapped by the surge of COVID-19 patients and as the hospitals were overcrowded, the infection rate in medical personnel increased amounting to nearly 9,000 medical professionals infected as on March 30, leading to further loss of capacity for healthcare system.
Seen in retrospect the number of cases and deaths in Italy cannot be explained simply because of the epidemic starting in the country earlier than other countries in Europe [19]. The specific age structure of the Italian population is an important factor, which the most elderly population in Europe. According to the study by Onder G, et al. [19] for the Italian people infected with COVID-19 and died, the median age of people has been 80 years, whereas the average age was 67 years for patients requiring critical care support. Further, because presence of concomitant diseases such as heart disease and history of chronic smoking, the elderly Italian population was vulnerable to the COVID-19 associated morbidity and mortality. About 99% people who died had at least one comorbidity, and 48.6% had 3 or more diseases that contributed to their death.
As of 30 May 2020, Italy has 43,691 active cases, with 232,664 confirmed cases and 33,340 deaths. Due to the limited number of tests performed, the real number of infected people in Italy is estimated to be much higher. The healthcare workers have been affected by Covid infection, with a high number of the infected healthcare workers being women because of their predominance among nurses. This resulted in death in a considerable number of medical professionals, more than 145 doctors in Italy had died with COVID-19 by 22 April [20]. Healthcare personnel are also subject to high levels of stress and the risk of professional burn-out is considered high, particularly among nurses and doctors alike especially in more affected areas.
COVID-19 Pandemic in Spain
The ongoing COVID-19 pandemic was first reported to have spread to Spain, simultaneously with Italy, on 31 January 2020. By 13 March, COVID-19 cases were confirmed in all 50 provinces of the country [21]. Despite the lockdown imposed on 14 March 2020, by late March, the Community of Madrid has recorded the most cases and deaths in the country. Medical professionals and those who live in retirement homes have experienced especially high infection rates [22]. As of 31 May 2020, there have been 239,429 confirmed cases and 27,127 deaths, but the actual number of cases is considered to be much higher, as many people with only mild or no symptoms have been tested [23].
Recently, on 13 May, the Spanish Government nation- wide seroprevalence study have shown that the percentage of population which could have been infected during the pandemic is approximately 5%, amounting to about 2 million people [24]. The number of persons testing sero-positive is about ten times higher than the number of confirmed cases. Similarly, the number of deaths, recorded as confirmed deaths due to COVID-19, may be an underestimate due to lack of testing and reporting.
COVID-19 Pandemic in France
The COVID-19 pandemic in France was confirmed to have reached on 24 January 2020, earlier than any other European country [25]. Following the arrival of pandemic, France went onto lockdown on 16 March 2020, which was extended twice and ended on 11 May 2020. As of 30 May, France has reported over 151,496 confirmed cases, 28,771 deaths, and 68,268 recoveries. A study led by the Pasteur Institute has reported that about 2.8 million people, 4.4% of the French population, appear to have been infected by the SARS-CoV-2, by 11 May 2020 when the lockdown measures were eased [26]. The study underlines the massive impact of the lockdown had on SARS-CoV-2 transmission in France and suggested that efficient control measures to limit transmission risk will have to be maintained beyond the 11 May 2020 to avoid a second outbreak of COVID-19 epidemic.
The US Experience in New York
The first COVID-19 case was confirmed in New York City on 1 March 2020. On March 3, the first person-to-person transmission in New York was reported. The COVID-19 cases have multiplied since then exponentially [27]. On March 20, the New York was closed down non-essential businesses, but the public transportation system remained open. By April, loss of jobs soured mainly affecting low income jobs in the retail, transportation, and restaurant sectors. Some of the most affected communities included densely populated neighborhoods in New York with high immigrant populations. This was accompanied by xenophobia and racism against Asians. By early May, over 5,200 Latinos in the city had died of COVID-19, the largest ethnic group with fatalities from the disease [28].
Innovative ICU Care Models for COVID-19
With the swift of growth of critically ill COVID-19 patients, it was required to utilize all clinicians within medical centers in New York to improve the critical care capacity. Simultaneously, the cancellation of elective cases and the consolidation of outpatient practices created a large pool of clinicians available for redeployment. With the innovative models, various hospitals became focused facilities caring for critically ill Covid-19 patients [29].
Utilizing the innovative ICU care model, the NewYork- Presbyterian, in association with Weill Cornell Medicine and Medical School of Columbia University structured a supervised pyramid-staffing model to serve 550 incremental ICU beds. The surge ICU beds were created in medical and surgical units, and in procedural areas such as the cardiac catheterization lab and in the operating rooms. There evolved concept of the emergency department ICU. The
multidisciplinary team consisted of anesthesiologists, pulmonologists, general surgeons, and cardiologists, to assist in critical care and develop the physician staffing complement for a Covid-19 ICU. The ICU frontline role staffed by residents, advanced practice providers, and certified critical care nurse.
This was supported by utilizing e-consultation and an inpatient tele-consult model to allow subspecialists to reach more patients and to decrease staff exposure and PPE utilization. There was developed an e-ICU program which enabled physicians for video enabled ICU rounds and critical care consultation. Simultaneously, a remote patient monitoring program took care of low and moderate-risk patients discharged from the emergency department, sub- intensive units, and indoor wards.
Rational Behavior for Covid-19 Prophylaxis
As regards the fear to contracting the virus, respondents in Asian countries have reported taking more precautions (such as avoiding public places and wearing face masks) compared to Western peers. On most parameters, Indians ranked close to the median. The survey also noted that in case of personal hygiene (washing hands, using sanitizers, etc.), people from some countries were relatively less cautious about hygiene compared to others from more developed countries. The residents from most of the counties rated their governments’ actions to contain the pandemic favorably. As per the survey, more than 80 percent respondents in Vietnam, India, and Denmark approved their government’s response to handling covid-19.
There are various surveys in offing and underway. The COVID-19 Symptoms & Social Distancing Web Survey by Harvard, aims to gather information on the prevalence of COVID-19 symptoms and social distancing behavior [30]. Another survey, the Knowledge, Attitude and Practice Survey on COVID-19 is a platform to receive feedback from the public on measures to improve efforts in the fight against COVID-19 and encourage behavior change [31]. There is also an International Survey on Coronaviruscovid19-survey.org to measure Worldwide COVID-19 Attitudes and Beliefs [32].
Anxiety and Concerns among Healthcare Professions
The healthcare professionals suffer with various concerns, which are different from the public at large [33]. The responses from 8 listening sessions with groups of physicians, nurses, advanced practice clinicians, residents, and fellows have disclosed the sources of anxiety and concerns among healthcare workers. Hear me, protect me, prepare me, support me and care for me was the message from health care professionals dealing with the COVID-19 pandemic delivered to their organizations, according to an article published in JAMA [34].
In general, the healthcare professionals are worried about availability of appropriate personal protective equipment, risk of exposure to COVID-19 at work and taking the infection home to their family, uncertainty that their organization will support for their personal and family needs if they develop infection, and issues about strenuous duties and long working hours and being able to provide competent medical care and access to up- to-date information and communication [35].
On the part of the policy planners, along with maintaining critical supplies, there should be maintenance of an adequate healthcare workforce to maximize the ability of each healthcare worker to handle increased number patients and overall workload. The simple and genuine expressions of gratitude for the commitment of health care professionals should be properly supplemented by concrete support and facilities.
Evolving Care-Practices for Covid-19
To combat the Covid-19 pandemic, the healthcare planners need a clear, systematic approach to quickly evaluate critical needs and identify areas of weakness. In addition, the healthcare setups need to proactively deploy a robust preparedness strategy. By acting early and rationally the healthcare systems may avoid being crippled by a sudden surge of the patients leading to crisis.
The cornerstones of an effective Covid-19 preparedness plan for a health system are mitigating transmission; conserving, supporting, and protecting staff and eliminating nonurgent strains on the healthcare delivery; and good communication [36].
The hospitals and clinics are likely hubs for the spread of Covid-19. The strategies should be taken to minimize unnecessary exposure and transmission of Covid-19 by limiting those entering the health care facility, reducing the staff to essential minimum, and screen and isolate people entering the facility. All noncurrent procedures should be cancelled or rescheduled. The mild and stable COVID-19 patients should be sent home for self- quarantine. The moderate COVID-19 cases should be evaluated for respiratory symptoms, distress, and hypoxia. Separate spaces required to separate services like screening, diagnostic and other testing and for healthcare providers. The healthcare providers need to feel optimally protected. Finally, there should be clear communication about disease, clinical state of the patient and risks involved, and the services available.
References
-
Walker PGT, Whittaker C, Watson O, Marc B, Kylie ECA, et al. (2020) The Global Impact of COVID-19 and Strategies for Mitigation and Suppression. Imperial College London, pp: 1-19.
-
Crook D, Adams ER, Bell J, Berry T, Beer S, et al. (2020) Evaluation of antibody testing for SARS-CoV-2 using ELISA and lateral flow immunoassays. MedRxiv preprint pp: 1-24.
-
Salje H, Kiem CT, Lefrancq N, Bosetti P, Juliette P, et al. (2020) REPORT-Estimating the burden of SARS-CoV-2 in France. Science 1-10.
-
The preliminary results from a study by the Carlos III public health institute.
-
Ahorsu DK, Lin CY, Imani V, Mohsen s, Mark DG, et al. (2020) The Fear of COVID-19 Scale: Development and Initial Validation. Int J Ment Health Addict pp: 1-9.
-
Soraci P, Ferrari A, Abbiati FA,Elena DF, Antonino U, et al. (2020) Validation and Psychometric Evaluation of the Italian Version of the Fear of COVID-19 Scale. Int J Ment Health Addict pp: 1-10.
-
(2020) Covid-19.
-
Adibe B, Perticone K, Hebert C (2020) Creating Wellness in a Pandemic: A Practical Framework for Health Systems Responding to Covid-19. NEJM Catalyst-Innovations in Care Delivery.
-
Roy D, Tripathy S, Kar Sk, Nivedita S, Sudhir KV, et al. (2020) Study of knowledge, attitude, anxiety & perceived mental healthcare need in Indian population during COVID-19 pandemic. Asian J Psychiatr 51: 102083.
-
Zhang Y, Ma ZF (2020) Impact of the COVID-19 Pandemic on Mental Health and Quality of Life among Local Residents in Liaoning Province, China: A Cross-Sectional Study. Int J Environ Res Public Health 17(7): 2381.
-
Cai W, Lian B, Song X, Tianya H, Huifen Li, et al. (2019) A Cross-Sectional Study on Mental Health Among Health Care Workers During the Outbreak of Corona Virus Disease. Asian J Psychiatr 51: 102111.
-
El-Hage W, Hingray C, Lemogne C, Yrondi A, Brunault P, et al. (2020) Health Professionals Facing the Coronavirus Disease 2019 (COVID-19) Pandemic: What Are the Mental Health Risks? (Article in French) 7006(20): 30076.
-
Bohlken J, Schomig F, Lemke MR, Matthias P, Steffi GRH (2020) COVID-19 Pandemic: Stress Experience of Healthcare Workers - A Short Current Review. Psychiatr Prax 47(4): 190-197.
-
(2020) Livemint.
-
(2020) COVID-19 pandemic in mainland China.
-
Wang C, Pan R, Wan X, Yilin T, Linkang Xu, et al. (2020) Immediate Psychological Responses and Associated Factors during the Initial Stage of the 2019 Coronavirus Disease (COVID-19) Epidemic among the General Population in China. Int J Environ 17(5): 1729.
-
Ewelina Biskup, Edward Prewitt (2020) Looking to the Future to Prepare for Covid-19’s Second Wave. NEJM Catalyst Innovations in Care Delivery 1(3).
-
(2020) COVID-19pandemicin Italy.
-
Onder G, Rezza G, Brusaferro S (2020) Case-Fatality Rate and Characteristics of Patients Dying in Relation to COVID-19 in Italy. JAMA 323(18): 1775-1776.
-
(2020) Coronavirus in Italy, first ok movements from 4/5, not between Regions. Conte: “He’s not a free everyone”.
-
(2020) COVID-19 pandemic in Spain.
-
Hedgecoe, Guy (2020) Top of the curve? Spain hopes Covid-19 peak reached as deaths pass 4,000. The Irish Times.
-
Lau H, Khosrawipour V, Kocbach P, Agata M, Ichii H, et al. (2020) Internationally lost COVID-19 cases. Journal of Microbiology, Immunology, and Infection 53(3): 454- 458.
-
Vardar, Serdar (2020) Two million Spaniards have been in contact with the new coronavirus.
-
(2020) COVID-19 pandemic in France.
-
Salje H, Kiem CT, Lefrancq N, Noemie L, Paolo B, et al. (2020) Estimating the burden of SARS-CoV-2 in France. Science pp: 1-10.
-
(2020) COVID-19 pandemic in the United States.
-
(2020) Corona virus updates.
-
Kumaraiah D, Yip N, Ivascu N, Hill L (2020) Innovative ICU Physician Care Models: Covid-19 Pandemic at NewYork- Presbyterian. pp: 1-6.
-
(2020) Harvard University.
-
(2020) International Survey of corona virus.
-
(2020) Infectious disease advisor.
-
Shanafelt T, Ripp J, Trockel M (2020) Understanding and addressing sources of anxiety among health care professionals during the COVID-19 pandemic. JAMA.
-
Weilenmann S, Ernst J, Petry H, Roland VK, Francesca P, et al. (2020) Health Care Workers Mental Health During the First Weeks of the SARS-CoV-2 Pandemic in Switzerland: A Cross-Sectional Study. MedRxiv preprint.
-
Kuy SR, Gupta R, Correa R, Sameer V, Raymond T (2020) Best Practices for a Covid-19 Preparedness Plan for Health Systems. NEJM Catalyst Innovations in Care Delivery pp: 1-11.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda