Natural Evolution of a Marfan’s Syndrome in a Medical Desert in Sub-Saharan Africa: Case Report
Marfan syndrome is an autosomal dominant connective tissue disorder associated with a mutation in the Fibrillin-1 (FBN1) gene on chromosome 15. It is a rare disease that affects one in 3,000 to 5,000 people. We describe here the case of a 35-year-old young man suffering from this syndrome and whose diagnosis was made at the terminal stage of the evolution in an environment lacking any means of diagnosis and care in sub-Saharan Africa.
Introduction
Marfan syndrome is an autosomal dominant connective tissue disorder associated with a mutation in the Fibrillin-1 (FBN1) gene on chromosome 15. It is a rare disease that affects one in 3,000 to 5,000 people. [1].
The most affected organs are the eye, the skeleton, the heart and the vessels. The prognosis of the disease is mainly related to the dilation of the initial aorta, determining an aneurysm that can progress to dissection or rupture.
Without treatment, life expectancy was limited to 40- 50 years [2] but with current progress in diagnosis and treatment, it approaches that of the general population [2]. Unfortunately, there are many regions in the world where conditions are not in place for the diagnosis of this type of pathology. This is the case in the Democratic Republic of Congo, a country in Central Africa, where a 35-year-old man died of a rupture of an aneurysm of the initial aorta whose diameter reached 150 mm, and whose summary is presented below.
This is a 35-year-old male subject who was living in a town in the eastern Democratic Republic of Congo, Kisangani, and was referred to us from a medical center where he was hospitalized. For a consultation during our visit in this city. Kisangani is the capital of a province of almost 200,000 km² (199,567), the largest in the country, with no cardiologists.
The patient had diffuse chest pain and dyspnea stage 4 for several months. He had no risk factors or cardiovascular history. In addition, he had no symptomatology suggestive of ocular involvement. After a first clinical and echocardiographic evaluation, the hypothesis of a Marfan syndrome with huge aneurysm of the initial aorta was mentioned and the patient transferred to Kinshasa for transfer formalities in South Africa, the country does not have medical infrastructure for the surgical management of the case. While waiting for the transfer, the patient was taken care of in our cardiological center.
His physical examination included the following essential elements: blood pressure at 100/60 mmHg, pulse at 100 / minute, respiratory rate at 26 cycles / minute, oxygen saturation in the open air at 90%, elongated constitution, spontaneous turgor jugular veins, asymmetric thorax with xiphoidal excavation (pectus excavatum) and slight bulging of the right hemi-thorax, arterial hyperpulsatility at the base of the neck with musset sign, 3/6 aortic breath and 3/6 mitral systolic murmur radiating to the armpit, congestive hepatomegaly, and lower extremity edema (Table 1). Ophthalmological examination could not be performed in this emergency context in the absence of signs of ocular involvement.
| Blood pressure (mmHg) | 100/60 |
|---|---|
| Pulse (beats/min) | 100 |
| Respiratory rate (cycles/min) | 26 |
| Oxygen saturation (%) | 90 |
| Slender constitution | lanky |
| Chest examination | Pectus excavatum deformity |
| Cardiac examination | - Complete arrhythmia |
| - Aortic insufficiency murmur | |
| - Mitral insufficiency murmur | |
| - Peripheral signs of congestive heart failure | |
| Vascular examination | Peripheral signs of aortic insufficiency. |
Table 2: Clinical data.
The Paraclinical Assessment gave the Following Main Results
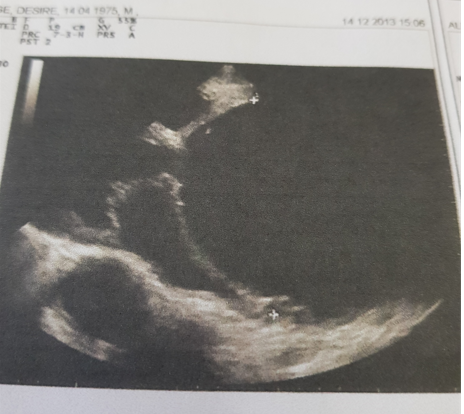
ECG: atrial fibrillation with ventricular rate at 100 / min, left anterior hemiblock and left ventricular hypertrophy; Cardiac echo-doppler: dilated valvular cardiomyopathy associated with extensive aneurysmal dilatation of the initial aorta and moderate dilatation of the thoracic and abdominal aorta (Table 2).
| Left atrial | |
|---|---|
| - Area (cm2) | 48 |
| - Indexed volume (ml/m2) | 133 |
| Left ventricle | |
| - Diatolic diameter (mm) | 66 |
| - Ejection fraction (%) | 36 |
| Interventricular septum | |
| - Diastolic thickness (mm) | 10 |
| Posterior wall | |
| - Diastolic thickness (mm) | 10 |
| Valves | |
| - Aortic insufficiency | severe |
| - Mitral insufficiency | severe |
| Aorta | |
| - Sinus of Valsalva and ascending aorta (mm) | 130 |
| - Isthmus (mm) | 50 |
| - Abdominal aorta (mm) | 24 |
Table 1: Echocardiographic data.
Chest angioscan: monstrous dilation 15 cm from the ascending aorta and 6 cm from the descending aorta with compression of the adjacent structures.
Diagnostic conclusion: strong suspicion of a Marfan syndrome associating:
- A large aneurysm of the initial aorta and diffuse dilatation of the ascending and descending aorta.
- Global heart failure with moderate severe and moderate mitral insufficiency, with severe impairment of left ventricular systolic function and pulmonary arterial hypertension.
While awaiting evacuation to a specialized center for thoracic and cardiovascular surgery, minimal symptomatic treatment of heart failure has been instituted, made of furosemide and oxygen.
The preparations for his transfer having been dragged, the patient died on the 7th day of his admission in a brutal installation shock table preceded by a strong acute chest pain, compatible with the rupture of the aneurysm of the aorta (Figure 1).
Comment
Marfan syndrome is a rare disease but its prevalence in Africa is not known due in particular to the inadequacy of health facilities and qualified medical personnel in most rural areas. The few data available for sub-Saharan Africa (SSA) suggest that eye damage is the predominant cause of consultation [3, 4, 5, 6]. In the present case, given the cardiac emergency, the ophthalmological examination could not be performed. A large-scale study could help describe the different organic conditions in this environment. This patient could have been saved if he had been detected early. But at the stage where the diagnosis was made, the prognosis, even after surgery, would have been very reserved because of the severity of the aortic and valvular lesions. This severity of cardiovascular damage could explain the precocity of death, compared to the average survival of untreated patients.
Most rural areas or provinces in SSA are real medical deserts where you can walk several tens or sometimes a hundred kilometers without meeting a single doctor. This exposes the population to sometimes fatal complications of undiagnosed diseases that follow their natural evolution. This situation is linked to the low level of socio-economic development of these countries. In the meantime, the solution may be through the organization of campaigns to detect certain diseases in under-medical areas, in order to mitigate the impact of these deadly and yet avoidable complications.
References
-
Judge DP, Dietz HC (2005) Marfan’s syndrome. Lancet 366: 1965-1976.
-
Pyeritz RE (2009) Marfan syndrome: 30 years of research equals 30 years of additional life expectancy. Heart 95: 173-175.
-
Schaftenaar E, Baarsma GS, Peters RPH (2015) Bilateral dislocation of the ocular lens in an African child. Archives of Disease in Childhood 100: 732.
-
Ukponmwan CU (2013) Ocular features and management challenges of Marfan’s Syndrome in Benin City, Nigeria. Niger Postgrad Med J 20(1): 24-28.
-
Ekure EN, Onakoya AO, Oke DA (2009) Marfan syndrome: a study of a Nigerian family and review of current cardiovascular management. West Afr J Med 28(1): 48- 53.
-
Diop IB, Ba SA, Sarr M, Kane A, Ly M, et al. (1994) Cardiovascular manifestations of Marfan’s syndrome; apropos of 6 cases. Dakar Med 39(2): 231-236.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda