Pharmacovigilance Difficult to Succeed without Clinician’s Involvement Approach to the Patient with Drug Allergy
Pharmacovigilance (PV): PV “is the science and activities relating to the detection, assessment, understanding, and prevention of adverse effects, or any other possible drug-related problems. All medicines and vaccines undergo rigorous testing for safety and efficacy through a clinical trial process, that involves studying these products in a relatively small number of selected individuals for a short period of time. Certain side effects emerge once these products are used by a heterogenous population, including people with other concurrent diseases, and over a long period of time. The WHO Programme for International Drug Monitoring (PIDM) was launched in 1968 with 10-member countries to promote ADR reporting, has 172 countries reporting by 2021 but not yet uniform in the world?. Drug Allergic reactions occur when the body's immune system has a reaction to a substance it sees as harmful, called an allergen. They are academically classified into six types: 1. dose-related (Augmented), 2. non-dose-related (Bizarre), 3. dose and time-related (Chronic), 4. time-related (Delayed), 5. withdrawal (End of use), and 6. failure of therapy (Failure). For clinical management four allergic reactions are recognized 1. immediate, 2. cytotoxic, 3. immune-complex mediated and 4. delayed hypersensitivity reactions. Diagnosis depends upon asking for a) patient’s identity data b) disease information c) drugs being used including Allergies if any, and doing skin test or drug sensitivity test and latest ALLERGY SCREENING TESTS BY IMMUNO – EIA, where IgE is assessed the normal for All Allergens is ≤ than 0.35 IU/ ml Management for a drug allergy involves two general strategies- 1. Treatment for present allergy symptoms by treating symptoms and 2. Treatment to enable taking an allergy-causing drug if it's medically necessary. Materials & Methods: This manuscript uses a case study under the care of the author, though mild challenging the management, supported by Top 10 Adverse Drug Reaction Related Notifications in 2019-2020 in India and literature review and global and National Health Mission guidelines and published articles
Introduction
Pharmacovigilance (PV) “is the science and activities relating to the detection, assessment, understanding, and prevention of adverse effects, or any other possible drug- related problems. All medicines and vaccines undergo rigorous testing for safety and efficacy through clinical trials process involving studying these products in a relatively small number of selected individuals for a short period of time. Certain side effects may only emerge once these products have been used by a heterogenous population, including people with other concurrent diseases, and over a long period of time. WHO initiated PV program in 1968 with 10-member countries to promote ADR reporting, but not yet uniform in the world? [1].
Drug allergy is an abnormal response to the medicine or metabolites through immunological reactions or hypersensitivity reaction that occurs during or after use of the drug. Allergic reaction to drug gets into the classification of adverse drug reaction, that has 5 components of toxicity, side effects, idiosyncrasy, intolerance, and medications allergy [2].
It is better to use the word Medicine instead of drug (which means abused substances). A medicine is pharmaceutical product used in or on human body for the prevention, diagnosis, treatment of a disease or modification of a physiological function [3]. The term side-effect is used in clinical settings and refers to any unintended effect of a pharmaceutical product, related to the known pharmacological properties of the drug. Adverse drug reaction refers to a response of a medicine which is noxious and unintended, that occurs at doses given normally to human beings and it focuses on individual response, in which individual factors play an important role, there is no overdose, phenomenon is noxious and unintended [3].
Drug toxicity is associated with medicinal effects of a drug overdose. Drug side effects are the main effects of the drug in addition to properties that arise due to the pharmacological properties of the drug or interactions with other drugs. Idiosyncratic drug reactions are not related to the pharmacological properties of the drug, but due to some unknown causes. Intolerance is not a reaction to the drug because of the pharmacological properties, arising from non- immunological processes. Drug Allergy is due to Immunologic sensitization after a first exposure to a drug and occurs after a latency period. Allergenicity of the drug depends on the molecular weight. Drugs with small molecular weight cannot directly stimulate the immune system when it is not joined with other materials to be as allergen, called hapten. Hapten can form covalent bonds with the protein network, is stable, and this bond will remain intact during processing in macrophages and presented at lymphocytes.
Drug allergies occur through four mechanisms of hypersensitivity.
- If specific antibodies IgE are formed in patients with atopic then it is the reaction type I.
- If antibodies are formed IgG and/ or IgM, complement activation it is reaction type II.
- If allergy occurs due to immune complex, then it is the reaction type III.
- When the cellular immune response arises, it is the reaction type IV.
Most common Drug allergies are by type I and IV.
Active Case Report
A teen aged boy is getting rashes over face & neck since early February 2022. Periodical papular eruptions mainly over face & neck lasted for few hours and disappeared. The size of the rashes was about 1 to 5 cm in diameter. Smaller were circular in shape and as 2 or more collapsed to form butterfly shape. Doubting irritant contact dermatitis due to detergents, soaps, cleaners, and allergic rashes due to cosmetic products, fragrances, the boy was put on antihistaminic. That relieved temporarily after 5 days but recurred after stopping the drug. Another course of antihistaminic was tried followed by slow tapering the drug over 2-week period, following the process of elimination of known allergens like stopping soap, hair oil and creams and other cosmetics he used but that too did not help much (Figures 1-8 & Tables 1-3).
Basic Investigations Done
- Total IGE in Blood (serum) = 550 IU/ml using CLIA technology, as against an expected highest level 170 IU.
- Serum Ferritin level was 65.6 ng/ml well within normal range.
- A recent laboratory test for allergen has indicated allergy to Cucumber, Capsicum, Yeast, home dust. The process of elimination is continuing with evading success.


| Reg. No: 2201022699 | Reg. Date & Time: 02/05/2022, 1255 | Name: ACHUTH ANTHA RAO | Age & Gender: | Sample Type: SERUM | Remarks : * Mild Allergy Mid-high Allergy * High Allergy | |
|---|---|---|---|---|---|---|
| ALLERGY SCREENING TESTS (BY IMMUNO - EIA) | ||||||
| TEST | RESULT | NORMALS | ||||
| IgE | 432.20 IU/Ml | 0.5 - 158 IU/ml | All Allergens is ≤ than 0.35 IU/ml | |||
| TEST | RESULT | TEST | RESULT | TEST | RESULT | |
| ALMOND ** | 1.8 | BAJARI | 0.18 | BANANA | 0.21 | FOODs |
| CAPSICUM ** | 1.4 | CUCUMBER** | 1.4 | VINEGAR ** | 1.2 | FOODs |
| WALNUT. | 0.15 | WHEAT | 0.29 | YEAST ** | 1.5 | FOODs |
| DOG DANDER * | 0.8 | HOUSEDUSTMITE *** | 3.6 | HOUSEDUST ** | 1.5 | INHALANTS |
| COTTON DUST | 0.14 | PAPER DUST ** | 1.1 | COW DANDER | 0.17 | INHALANTS |
| CIPROFLOXACIN * | 0.8 | OFLOXACIN * | 0.7 | TINIDAZOLE ** | 1.3 | DRUGS |
| AMOXYCILLIN | 0.34 | AMPICILLIN | 0.05 | ASPIRIN | 0.21 | DRUGS |
| DETERGENT | 0.2 | LEATHER | 0.04 | PLASTIC | 0.02 | CONTACT |
| CAUSTIC SODA | 0.3 | PERFUME | 0.28 | WOOL MIX | 0.08 | CONTACT |
Total Items Tested: Food=88 (6 Non-Veg), Inhalants=89, Drugs=22 and Contacts=15 Note: This is an illustrative extract showing all allergic items and sample non-allergic items in each category Table1: Comprehensive Allergy Test Panel.
Based on the above allergy test dated 2 May 2022, the boy is avoiding contact with a pet Dog, touching paper over neck & face, and avoiding foods like capsicum, cucumber, and Almond. He is advised use Benadryl lotion on the face and take Benadryl tablets if required. In the last 10 days the situation is under control and the patient is under further observation.
Discussions
Drug allergies may be over-diagnosed, and some patients may report drug allergies but are never confirmed. Even the clinicians under report minor drug allergies. Misdiagnosed drug allergies may result in the use of less appropriate or more expensive drugs [4, 5].
Drug allergies can occur through four mechanisms of hypersensitivity.
- If specific antibodies IgE are formed in patients with atopic then it is the reaction type I.
- If antibodies are formed IgG and/ or IgM, complement activation it is reaction type II.
- If allergy occurs due to immune complex, then it is the reaction type III.
- When the cellular immune response arises, it is the reaction type IV.
Signs & Symptoms
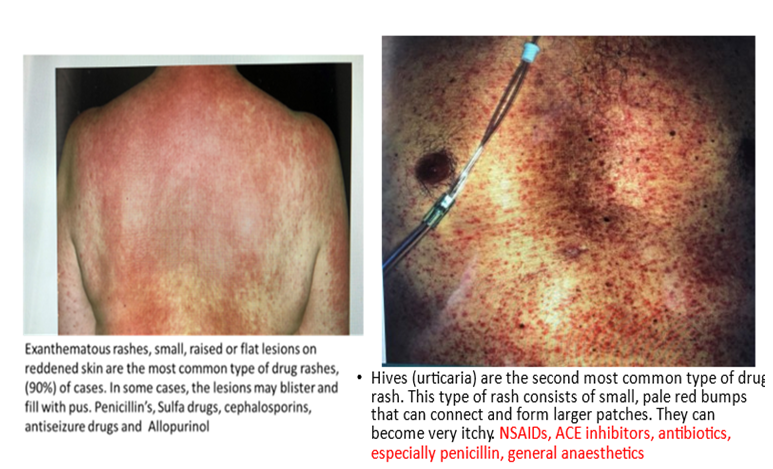
One drug can cause a variety of symptoms in different persons, and they can be mild to severe. Skin eruptions are the most frequent clinical symptoms, can include itching, Urticaria, larynx oedema, purpura, contact dermatitis, erythema multiforme, and erythema nodosum. Common medication triggers are Penicillin Injection, Muscle relaxants like the ones used for anaesthesia, Aspirin, ibuprofen, and other NSAIDs and Anti-seizure medications. For the clinician’s purpose the allergic reactions are classified into 6 categories. • Exanthemata’s Rashes (ER) and Hives/ Urticaria (U) The author has been seeing exanthemata’s rashes since 1968 mainly following Penicillin and in mid-1970’s following Lignocaine local anaesthetic injections used to do vasectomy operations on an outpatient basis. Urticaria was more common after use of anti-epileptics and general anaesthesia using ethyl chloride and ether drops for tubal ligation operations in late mid 1980’s. ER are small raised or flat red lesions, in some case becoming blisters and pustules following penicillin injections and oral Sulpha drugs. The use of Penicillin injections has come down drastically in the last 2 decades as better alternative antibiotics were introduced.
Urticaria small, pale red bumps that connect to from large patches is the second common feature seen triggered after use of Penicillin, NSAIDs.
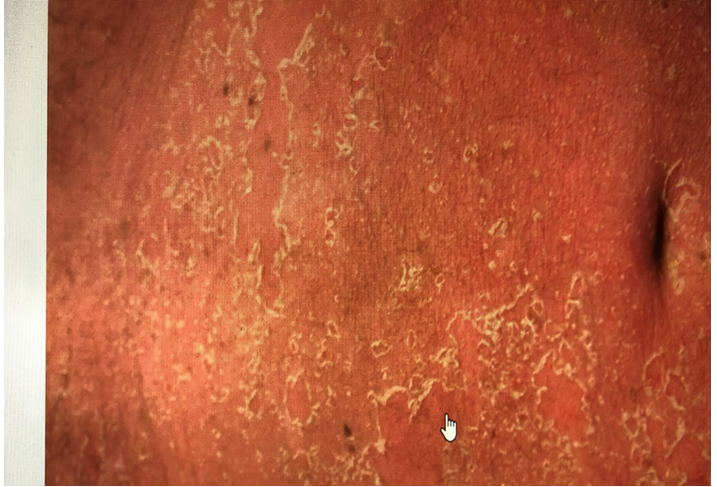
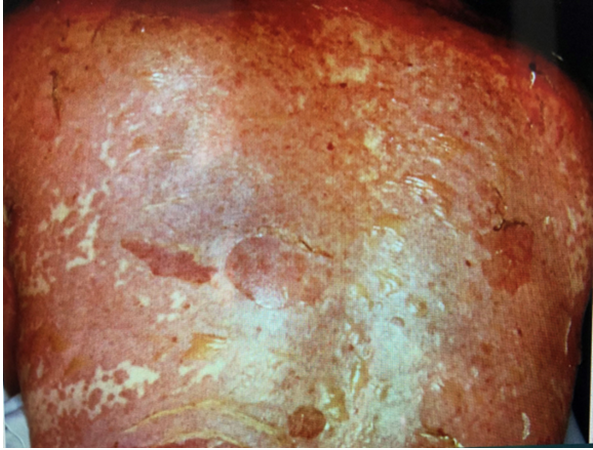
• Erythroderma Erythroderma is a potentially life-threatening condition with entire skin becoming itchy and red. May experience a fever, skin hot to the touch. sulpha drugs, penicillin’s, antiseizure drugs, chloroquine. Allopurinol and isoniazid may cause Erythroderma. The author saw one such case during mid-1970’s following chloroquine tablets as a part of Plasmodium Vivax radical treatment.
• Stevens-Johnson syndrome (SJS) and toxic epidermal necrolysis (TEN) Are a variety of very severe reactions, mostly triggered by medications, like Sulpha drugs, antiseizure drugs, some NSAIDs, allopurinol and nevirapine. The allergy causes skin tissue to die (necrosis) and detach. The mucous membranes of the eyes, mouth, and/or genitals are also commonly affected. Both rashes appear to be similar, but the only difference in SJS affects 10% of body & and TEN affects 30% of body.
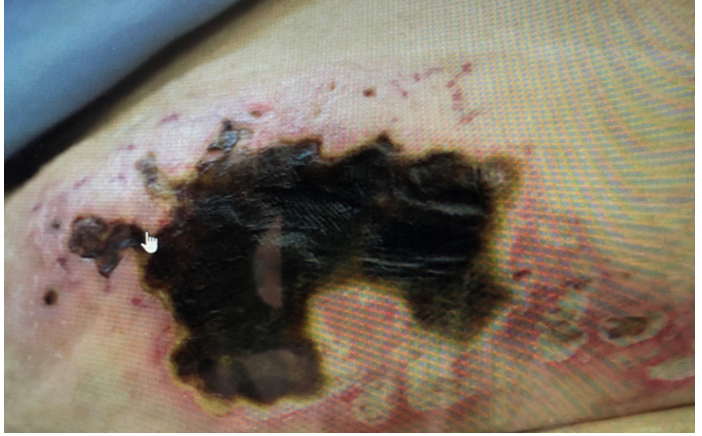
• Anti-coagulant induced Necrosis Certain blood thinners, such as warfarin, cause anticoagulant-induced skin necrosis. At first, you might notice skin turns red and painful. As necrosis progresses, the tissue beneath your skin dies. The risk of this reaction tends to be higher at the start of taking a very high dose of a new blood thinner.
• Ultra-violet sensitivity Tetracyclines, Sulpha drugs, antifungals, antihistamines, retinoids, statins, Diuretics and some NSAIDs can make skin extra sensitive to ultraviolet light, causing a subsequent itchy sunburn if you go outside without wearing sunscreen and protective clothing.

• Anaphylaxis Anaphylaxis is a severe, potentially life-threatening allergic reaction. It can occur within seconds or minutes of exposure to something an individual is allergic to, such as peanuts or bee stings. In Anaphylaxis our immune system releases a flood of chemicals that results in sudden blood pressure drops suddenly and the airways narrow, blocking breathing and the person can go into shock. The signs and symptoms include a rapid, weak pulse; a skin rash; and nausea and vomiting. It needs to be treated right away. Anaphylaxis is rare, and most people recover from it. Epinephrine (adrenaline) injection be given as soon as possible, that reverses the symptoms within minutes. If this doesn’t happen, a second shot within half an hour must be given. Antihistamines have no role in the management of an anaphylactic reaction. Previous H/O anaphylactic reaction and a family history of anaphylaxis or have asthma, have a higher risk of having another one.
Academic Classifications of Allergic Reactions
Drug Allergic reactions occur when the body’s immune system has a reaction to a substance it sees as harmful, called an allergen. They are academically classified into six types:
- dose-related (Augmented),
- non-dose-related (Bizarre),
- dose and time-related (Chronic),
- time-related (Delayed),
- withdrawal (End of use), and
- failure of therapy (Failure).
| Maemonics* | Features | |
|---|---|---|
| A: Dose rellated | Augmented | Related to pharmacology (toxic effect for side-effect). eg. bradycardia with beita blockers digoxari toxicity |
| B: Non-dose related | Bizarre | Unrelated to pharmacology (i) idiosyncratic es fractures with proton purno inhibitors (ii) immunological eg. |
| C: Drose and time related | Continuous or chronic | Related to cumulatis edrug use NSAID induced renal failure |
| D. Dellayed effect | Delayed | Apparent only some time after use of drug (0 endometrial carcinoma in women associated with the use of stilboesterol by their mothers during pregnancy, (io thalidomide taken by mothers in first trimester and phocomelia in the baby |
| E: Withdrawal | End of use | Related to discontinuation that is too abrupt eg. Addisonian crisis after steroid withdrawal |
Table 2: A clinicians’ guide to adverse drug reactions.
The letters A, B. C. D and E help to remember the TYPE of reaction. Table 2: A clinicians’ guide to adverse drug reactions.
Clinicians & ADR Success
The current Pharmacovigilance system alone in most of the developing countries like India cannot succeed in handling drug allergies. The role of clinicians particularly in small settings is very important to address the prevailing under-reporting of ADRs. From the Clinicians point of view, it is better to use the concept of “suspected adverse reactions” as it is not possible to label the reaction as ADR, that may or may not have causal association.
For clinical management Four different types of allergic reactions are recognized
- immediate,
- cytotoxic,
- immune-complex mediated and
- delayed hypersensitivity reactions.
A validated questionnaire used study of KAP of a regionally representative sample of 570 physicians including 113 general practitioners, 123 paediatricians,
110 pulmonologists, 113 dermatologists, and 111 gastroenterologists from all major institutions in Hyderabad, India revealed that overall, 90% of questions were correctly answered and differences emerged with respect to specific items like 1) The lateral thigh being the preferred location for epinephrine administration (P = .001); (2) a positive skin prick test or radioallergosorbent test is sufficient for FA diagnosis (P = .04); and (3) the appropriate epinephrine dose for a 27-kg child (P = .006). Approximately 95% of the participants in each group were confident in their ability to care for patients with FA, yet 91% desired additional periodic FA training sessions [7].
A 2-year long term prospective study included 4005 ambulatory elderly patients (60 yrs. or above; either sex) at a public teaching hospital, observed 406 (10%) patients with ADRs, in elderly. The total number of ADRs was 422 in 406 prescriptions. Type A ADRs accounted for 46 % of the total ADRs. Majority of the ADRs (88.6%) were classified as ‘probable’ and the preventable reactions were 22%. The percentage of moderate reaction was 16% and only 1.6 per cent ADRs was severe in nature. The most common type of ADR was peripheral oedema. The most commonly offending class of drug was cardiovascular drugs (57.6%). Using logistic regression analysis, the study inferred risk factors that contributed to ADRs were age above 80 yrs. (OR=1.7), prescription of multiple drugs (OR=1.8), longer duration of treatment (OR=2.28) and multiple diagnoses (OR=1.8) [2, 8].
Diagnosis of Drug Allergies
Current understanding suggests that drug allergies may be over-diagnosed and/ or that patients may over- report. Misdiagnosed drug allergies result in the use of less appropriate or more expensive drugs [3, 4].
Skin Tests
In a skin test, doctor or a nurse administers a small amount of a suspect drug with a tiny needle that scratches the skin, an injection, or a patch. A positive reaction to a test will cause a red, itchy, raised bump suggesting a drug allergy.
A negative test result usually means the patient is not allergic to the drug, but in some cases may not completely rule out the possibility of a drug allergy.
Blood Tests
Antibiotic Sensitivity Test: An antibiotic sensitivity test helps to find out which antibiotic will be most effective in treating infections of a given patient. This test is done if an infection has been shown to have antibiotic resistance or is otherwise hard to treat like Tuberculosis, MRSA, and C. diff. A bacterial or fungal infection that is not responding to standard treatments may also necessitate this test. A sample from the infected site: Blood culture, Urine culture, Wound culture, Sputum culture is taken for such a test. There is very little risk to having a blood culture test. You may have slight pain or bruising at the spot where the needle was put in, but most symptoms go away quickly. Throat culture: Technician will insert a special swab into your mouth to take a sample from the back of the throat and tonsils as was done in Covid 19 PCRT. Throat culture may cause slight discomfort or gagging.
Results
These are usually described in one of the following ways: Susceptible: The tested medicine stopped the growth or killed the bacteria or fungus causing your infection. The medicine may be a good choice for treatment.
Intermediate: The medicine may work at a higher dose.
Resistant: The medicine did not stop the growth or kill the bacteria or fungus causing the infection. It would not be a good choice for treatment. Comprehensive allergy Panel: A single blood tests for detecting allergic reactions includes Food Allergens [96 Parameters], Non-Veg Allergens [11], Inhalant Allergens including Pollens, Fungi, insects [67], Drug Allergens [28], Dusts, Dander and others and IgE Level [1] (Table 1).
Management for a Drug Allergy
A clinician must follow two general strategies: • Treatment for present allergy symptoms: Treatment of anaphylaxis: Anaphylaxis requires an immediate epinephrine injection as well as hospital care to maintain blood pressure and support breathing. Withdrawal of the drug. discontinuing the drug is the first and the only step in treatment in majority of cases Antihistamines: Prescribe an antihistamine such as diphenhydramine (Benadryl /Allegra) that can block immune system chemicals activated during an allergic reaction. Corticosteroids: Either oral or injected corticosteroids may be used to treat inflammation associated with more-serious reactions. Treatment to Enable Taking an Allergy-Causing Drug if it’s Medically Necessary These interventions are generally avoided if drugs have caused severe, life-threatening reactions in the past. Provide the drug under careful supervision: Be ready with services to treat an adverse reaction if it occurs. Graded Challenge: Clinicians give two to five doses of the drug, starting with a small dose and increasing to the desired dose. If the patient reaches the therapeutic dose with no reaction, then the drug given as prescribed. Drug desensitization: If it’s necessary for the patient to take a drug that has caused an allergic reaction, then you give a very small dose and then progressively larger doses every 15 to 30 minutes over several hours or days. If you can reach the desired dosage with no reaction, then the treatment is continued [4].
Approach to Drug Reactions Patients
Ask for a) patient’s identity data b) disease information c) drugs being used including Allergies if any. A clinician needs to elicit answers to questions like- 1. Does the patient have indication for each of the drug prescribed? 2. Are the drugs effective for the condition? And are they safe, 4 Is patient willing to take the drugs for intended periods & dosage?.
Why more ADRs Occur in India & what are we doing? Whenever a new drug is launched in the market, it is assumed to be safe, based on vigorous studies of quality, effectiveness, and safety parameters. Regulatory authorities approve the drug depending on its efficacy at acceptable limit of safety. Rarely serious ADRs occur, during the preapproval period of the drug.
There are 2 types of ADRs reported in India. Type A reactions are predictable from the known pharmacology of a drug and are associated with high morbidity and low mortality. Type B reactions are idiosyncratic, bizarre, or novel responses that cannot be predicted from the known pharmacology of a drug and are associated with low morbidity and high mortality.
A study of 6270 consecutive patients with allergic manifestations attending a clinic from July 01, 2008, to June 30, 2018. Patients underwent a complete allergy work-up including total serum IgE levels, skin prick tests, patch tests, pulmonary function tests and nasal function test. The results revealed that insect allergens have a high positivity rate. Atopy, Pollen allergy and food allergy are less common in India. Cocoa is the commonest food allergen [7, 8].
Common forms of ADR resolutions for civil cases in India: Pharmacovigilance Programme in India is in a nascent form and reporting is generally poor and only severe cases are reported. Common resolutions include- Mediation. Arbitration.
Neutral Evaluation. ..., Settlement Conferences. ...and Community Dispute Resolution Program. Legal recourse is resorted only if a nurse /doctor administers medicines to which an individual is allergic, despite knowing the fact and pursue a case for damages [9, 10].
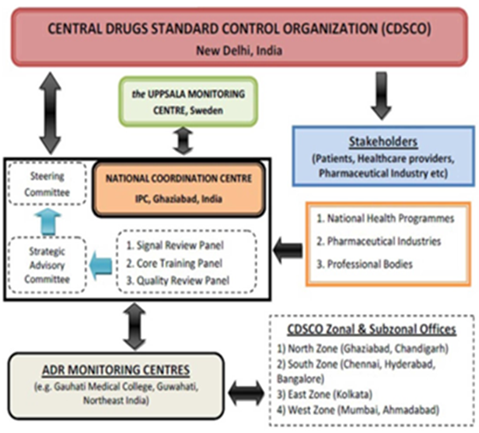
Pharmacovigilance Programme of India (PvPI)
Launched by the MoH&FW, Govt. of India in the year 2010 at AIIMS New Delhi National Coordinating Centre (NCC), transferred to IPC as NCC in April 2011 that became IPC-PvPI became the NCC for Materiovigilance Programme of India (MvPI) from July 2015. IPC, NCC-PvPI became a WHO Collaborating Centre for Pharmacovigilance in Public Health Programmes & Regulatory services from July 2017 NHP 2017 needs to take it forwards [11].
| 1 | Chloroquine | Steven Johnson Syndrome -Toxic Epidermal Necrosis | 2020-Jan-30 |
|---|---|---|---|
| 2 | Lamivudine | Hearing Loss | 2020-Jan-13 |
| 3 | Proton Pump Inhibitor | Acute Kidney Injury | 2019-Nov-04 |
| 4 | Diclofenac | Nicolaus syndrome | 2019-Jul-24 |
| 5 | CarbamazepineD | Drug Rash with Eosinophilia and Systemic Symptom (DRESS)t | 2019-Jun-19 |
| 6 | Cefixime | Mouth Ulceration | 2019-Jun-19 |
| 7 | Meropenem | Hypokalemia | 2019-Jun-19 |
| 8 | Artemether + Lumefantrine | Steven Johnson Syndrome (SJS)a | 2019-Jun-19 |
| 9 | Phenobarbital | Drug Rash with Eosinophilia and Systemic Symptom (DRESS)1 | 2019-Jun-16 |
| 10 | Amlodipine | Gingival Hypertrophy | 2019-Jun-13 |
Table 3: Top 10 Adverse Drug Reaction Related Notifications in 2019-2020 in India [11,12].
Way forwards:
- Educating individual practitioners about possible ADRs, their assessment & management
- Establish Facilities for ADRs tests in all districts under National Health Mission
- States / district professional organization and NHM should start collating ADR cases from both Public and Private sector and share on Digital platforms.
- Periodical sharing of the ADRs by Central & Sate Drugs standard Control organization at least quarterly & SOS.
- Post-marketing surveillance of ADRs by companies introducing new product for the safety of the drug.
- Pharmacovigilance studies by states to identify types of unpredictable drug reactions.
- Expansion of Pharmacovigilance in Public Health Programmes & Regulatory services in states
- Protection to the individual doctors against legal action in unforeseen conditions
References
-
Edwards IR, Aronson JK (2000) Adverse drug reactions: definitions, diagnosis, and management. Lancet 356(9237): 1255-1259.
-
Kaufman G (2016) Adverse drug reactions: classification, susceptibility and reporting. Nurs Stand 30(50): 53-63.
-
(2020) Pharmacovigilance regulation-prequalification/ regulation-and-safety. WHO.
-
Ranganathan SS (2007) A clinicians’ guide to adverse drug reactions. Ceylon Med J 52(2): 41-44.
-
(2020) Drug allergy. Patient Care & health information.
-
(2015) What is India doing to curb Adverse Drug Reactions.
-
Shaikh WA, Shaikh SW (2019) Allergies in india--a study of 6270 patients. Journal of Evolution of Medical and Dental Sciences 8(10).
-
Jain PD (2020) Knowledge, attitude, and practices of medical clinicians regarding food allergy and anaphylaxis in Hyderabad, India. Ann Allergy Asthma Immunol 125(5): 560-564.
-
Forms of Alternative Dispute Resolution.
-
Sahu RK (2014) Adverse drug reactions monitoring: prospects and impending challenges for pharmacovigilance. Springerplus 3: 695.
-
Mandavi (2012) Adverse drug reactions & their risk factors among Indian ambulatory elderly patients. Indian J Med Res 136(3): 404-410.
-
Kalaiselvan V (2019) Pharmacovigilance in India: Present Scenario and Future Challenges. Drug Safe 42(3): 339-346.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda