Unmasking and Managing Hypercalcaemia-In Clinical Settings!
Objective: In this article I present 2 cases of hypercalcaemia identified and managed in 2021 in smaller settings and review of literature of such cases in bigger facilities India with an objective of alerting private practitioners’ role in managing such cases efficiently. Hypercalcaemia is not a disease but just a biomarker of a total serum calcium concentration > 10.4 mg/dL (> 2.60 mmol/L) or ionized serum calcium > 5.2 mg/dL (> 1.30 mmol/L). Principal causes include Primary hyperparathyroidism, vitamin D toxicity, and cancer. The serum Calcium and Phosphorous (Ca/P) ratio is a most valuable tool for the diagnosis of Primary hyperparathyroidism, better than serum Calcium alone. Locations of cases reported: Kalimpong in West Bengal and Chikkaballapur near Bengaluru Participants: i) A - 66-year-old Kamala Pradhan, a known diabetic, my patient in Delhi for last 5 years presenting with pruritus, muscle weakness, lack of appetite and weight lost for 3 months and accidentally diagnosed after a Blood test as moderate hypercalcaemic due to over consumption of Vit. D (weekly 60 K units for 3 years) and ii) the second case of a rural 45 year’s old women from Bengaluru in May 2021 diagnosed as Cancer Cervix stage 3 at a private cancer hospital in Bangalore who succumbed in about 3 week’s time Measurements: i) In the first a serum test indicated serum Calcium level 20 mg/dl and Vitamin D 150ng/ml in first test and after management for a months’ time Calcium levels came down to 10mg/dl and Vitamin D levels to 50ng/ml. ii) Second case had calcium level of 120 mg/dl indicating Calcium crisis. Results: The first case of moderate hypercalcemia due to Vit D intoxication improved, the Calcium level came down to 10mg/dl and D Vitamin came down to 50ng/ml with clinical improvements in 12 weeks’ time. The Calcaemic crisis was not monitored as the patient died within 3 weeks of starting treatment. Conclusion: A case of successful management of moderate due to Vitamin D intoxication and another case of calcinemia crisis due to advanced cervical cancer, with serious complications, and death are reported for education of general practitioners. Material & Methods: The author a family physician for 54 years and a Public Health practitioner for 45 years, have used 2 cases of hypercalcaemia followed in 2021 and review some other published cases, along with a few retrospective studies in India and abroad, that lead to hypercalcaemia and current recommendations for the management of elevated serum calcium levels.
Introduction
Hypercalcaemia is a common metabolic abnormality seen in both inpatient and outpatient settings, showing an elevation of Serum calcium levels in the peripheral blood. It is not a disease, but a disorder indicated by Biomarkers of Calcium and Potassium.
In plasma, calcium exists in 3 different forms: (1) 50% as ionized or the biologically active form, (2) 45% bound to plasma proteins (mainly albumin), and (3) 5% complexed to phosphate and citrate. Almost all our body’s calcium is stored in your bones. A very small amount -- about 1% -- is in our blood as Ionized calcium in our blood, that helps in muscle contraction, nerve signalling, and blood clotting. Serum calcium levels fluctuate based on the serum albumin levels. Serum Calcium, is variable, depending on age, sex, physiological state (e.g., pregnancy), and even season owing to the seasonal variation of vitamin D, which regulates the calcium concentration. Total calcium reference normal ranges are as follows i) Babies< 10 days: 7.6-10.4 mg/ dL; 1.9-2.6 mmol/L, & Umbilical: 9-11.5 mg/dL; 2.25-2.88 mmol/L ii) 10 days-2 years: 9-10.6 mg/dL; 2.3-2.65 mmol/L, iii) Child: 8.8-10.8 mg/dL; 2.2-2.7 mmol/L and iv) Adults: 9-10.5 mg/dL; 2.25-2.62 mmol/L that tend to be bit reduced in elderly persons.) Hypercalcemia is categorized based on serum calcium levels, as i) Mild if calcium levels are 10.0– 12 mg/dL (2.5–3 mmol/L) OR ionized calcium 5.25–8 mg/ dL (1.31–2 mmol/L), ii) Moderate when total calcium levels is 12–14 mg/dL (3–3.5 mmol/L) and hypercalcaemic crisis when the total calcium level is > 14 mg/dL (> 3.5 mmol/L) [1, 2, 3].
Hypercalcemia is caused by a) overactive parathyroid glands due to a small benign tumour or enlargement of one or more of the four parathyroid glands b) Some types of Cancers and c) Some medicines like Thiazide diuretics, Teriparatide, Oestrogens, Tamoxifen and Lithium d) Over supplementation of Calcium- main forms of calcium supplements are carbonate, citrate, gluconate, and lactate. Some calcium supplements are combined with vitamins and other minerals. Foods high in calcium include cheese, cottage cheese, yogurt, pudding, and ice cream (Figure 1).
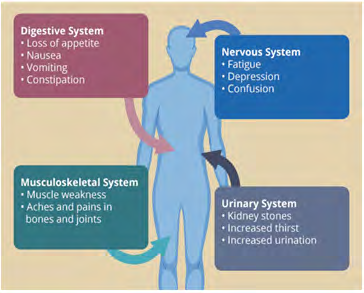
Too much calcium in our blood affects our digestive, nervous, urinary, and musculoskeletal systems. Based on the system affected it can weaken bones, create kidney stones, and interfere with how heart and brain work. Clinical manifestations include nausea, vomiting, fatigability, muscle weakness, depression, anorexia, and constipation, increased thirst, and urination. Most common cause of Hypercalcaemia is Primary hyperparathyroidism that affects people between age 50 and 60 yrs., affecting women 3 to 4 times more than men.
Case Reports: Cases I managed /Followed in 2021
1. A - 66-year-old Kamala Pradhan (names changed) called me in early December 2021 from Gurung Basti Kalimpong, West Bengal complaining that she is suffering from pruritus, muscle weakness, lack of appetite and weight loss for 3 months. Kamala was a known diabetic of a decade under my treatment in Delhi with FBS- 182, Hb1Ac (9,2) Vitamin D3 (25 Hydroxy) levels of 12.4 ng/ml in March 2018 and was advised to take oral antidiabetics, diet regulation and walking for 2-3 Kms a day and D-rise a Vitamin D supplement before once a month to start with, then once a fortnight for 4 times and once every month regularly thereafter. I moved to Bengaluru in April 2018, and they moved to Kalimpong in 2019, but our telephonic consultations continued once in 4-6 months. The history revealed that She continued to take D-Rise at weekly interval for almost 3 years and due to Covid 19 Pandemic exercise (walking) was almost stopped. A blood tests in December 2021 showed Hb1Ac 8.2, FBS 160, Creatinine 0.83 mg/dl and serum Calcium level 20 mg/dl and Vitamin D 150ng/ml. Diagnosing as Vit. D intoxication, I stopped the Vitamin D supplementation and advised over hydration with frequent fluids intake and diuretics. In the report of 8 April 22 the Calcium levels came down to 10mg/dl and Vitamin D levels to 50ng/ml within 12 weeks’ time. All the symptoms had disappeared, and she was feeling normal. 2. A rural 45 year’s old women (an aunt of one of my PG students) from Chikkaballapur 100 kms away from Bengaluru had reported on 4th May 2021 with symptoms vaginal bleeding, back pain, urine leakage & pelvic pain for 2 months to a gynaecologic oncology service at a cancer hospital & research centre, Bangalore. She had consulted a family doctor first who referred her to the Cancer hospital. On admission her Pulse was 72/min, BP 85/135 mm hg, Temperature 98.200 F, SPO2 97%
(mandated in Covid 19 Pandemic) & Weight 44kgs. Investigations: A battery of tests like blood sugar, cholesterol, LFT, THYROID and Parathyroid hormones & serological RA factors were normal, Serum Calcium was high at 120mg/dl & abnormal & Hb% was low (8dl/mg). After an evaluation for abnormal vagina bleeding, cervical biopsies that demonstrated invasive adenocarcinoma of the cervix (Stage IV B CA Cervix) the diagnosis was confirmed. Since it was in an advanced stage, a palliative management including radiation therapy for control of bleeding & pain, and systemic chemotherapy for disseminated disease was opted and was given IV fluids and with diuretic for hypercalciuria. After 22 days of treatment, she got discharged along with medications prescribed Inj. Amikacin 100mg IV OD, Inj. Pantoprazole 40mg IV OD, DNS which was given by the local doctor. However, there was no progress and she died on 17th June 2021.
Clinician’s Suspicion in Smaller Settings
Clinicians suspect if a routine Calcium level shows abnormal level of Calcium and seek a Parathyroid Hormone Test (PHT) test. The confirmation of diagnosis in small settings depend solely on measuring parathyroid hormones in blood /serum. The test would cost between INR 700-1500. Clinical laboratories generally measure the total serum calcium level. As changes in the albumin level causes misleading increases or decreases, respectively, in the total serum calcium level, it is valuable to measure the serum level of ionized calcium. Alternately there are formulas to calculate the serum ionized calcium level or to “correct” the total calcium level (add 0.8 mg per DL to the total calcium level for every 1.0 g per DL of serum albumin below the level of 3.5 g per DL).
Other Cases in India from Literature Review
• Multiple myeloma with hypercalcaemic encephalopathy, AIIMS Jodhpur 2019: An 84-year-old female presented to the emergency department of AIMS Jodhpur, in October 2019 with complaints of constipation, vomiting, decreased appetite, and excessive urination for the last 10 days and altered sensorium for the last 2 days. There was a history of generalised bone pain for last 3 months for which she was prescribed calcium. Except Bell’s palsy 5 months back with complete recovery, past and family history was unremarkable. On examination, the patient was drowsy but arousable. She was dehydrated, and blood pressure was 146/90 mm Hg. Her systemic examination including neurological did not reveal any localisation.
Investigations revealed anaemia (Hb—6.5 g/dl), deranged renal function (urea—118 mg/dl, creatinine 5.62 mg/dl), increased total protein (9.27 g/dl) and globulin (7.34 g/dl), low albumin (1.93 g/dl), and hypercalcemia (total calcium-15.07 mg/dl). Random plasma glucose (131 mg/dl) and serum electrolytes (sodium/ potassium—141/3.92 meq/L) were in the normal range. Serum PTH levels and serum ammonia levels were normal (39.4 mmol/L, normal 17–90 mmol/L).
Non-contrast computerised tomography of brain showed age-related changes in the bilateral cerebral hemisphere with multiple lytic lesions of varying sizes noticed in the cranial vault and base of the skull. The patient was diagnosed as hypercalcaemic encephalopathy with suspicion of multiple myeloma. To confirm the diagnosis of multiple myeloma, serum protein electrophoresis was performed, which showed M protein (in the beta region) 4.9 g/dL with increased beta 2 microglobulin (9284 ng/ml, normal 609–2366 ng/ml). Bone marrow aspiration showed 60% plasma cells. The final diagnosis of multiple myeloma with hypercalcaemic encephalopathy was made.
The patient was treated with iv. fluids (0.9% normal saline, 200 ml/hr with the rate adjusted to maintain urine output 100–150 ml/hr) with loop diuretics and calcitonin. The next day, zoledronic acid (at modified dose according to GFR) was added. On day 9 of hospitalisation, the patient was put on dexamethasone, lenalidomide, and bortezomib. At the end of 2nd week patient’s sensorium was improved, with normalization of serum calcium and renal function [4, 5, 6].
• Hypercalcaemia with Breast Cancer: i) A 60-year-old woman with a history of breast cancer presents with confusion and dehydration. She had postural hypotension and low central venous pressure on examination of the jugular veins. The serum calcium level is 18.0 mg per decilitre (4.5 mmol per litre), Phosphorus level was 5.0 mg per decilitre (1.6 mmol per litre), the blood urea nitrogen level is 80.0 mg per decilitre (28.6 mmol per litre), the serum creatinine level is 2.0 mg per decilitres (177 μmol per litre), and the albumin level is 3.3 g per decilitres [7]. ii) A 48-year-old woman was given a diagnosis of infiltrating ductal breast carcinoma (T2N1M0; grade I; positive for oestrogen receptors, progesterone receptors and human epidermal receptor-2 [HER2] status; with 3/31 positive nodes). left lumpectomy with axillary node dissection followed by chemotherapy and radiotherapy was the treatment given. Thirteen years later, she was given a diagnosis of breast cancer recurrence. The patient had hypercalcemia on multiple occasions, with corrected calcium levels ranging from 2.72 to 2.85 (normal 2.1–2.6) mmol/L, dating back to the time of diagnosis of her breast cancer. She did not have symptoms directly attributable to hypercalcemia apart from one episode of nephrolithiasis 11 years after diagnosis. Hypercalcemia was again noted two years later, with a serum corrected calcium level of 2.95 mmol/L [8].
• Vitamin D intoxication: i) A 53-year-old male patient, with history diabetes mellitus, hypertension, non-dialysis chronic renal failure and smoking was admitted to a hospital in September 2011 to investigate worsening of the renal function, pruritus, muscle weakness, lack of appetite and weight lost. Table 1 displays the results of the biochemical tests before hospitalization.
| Month/year | Calcium | ||||
|---|---|---|---|---|---|
| (8.4-10.4) mg/dL | Ionized calcium (1.14- 1.31) mmol/L | Parathyroid hormone (12.0-65.0) pg/mL | Creatinine (0.6- 1.2) mg/dL | 25(OH)D (30- 100) ng/mL | |
| Aug/Sept. 2011 | 13.4 | 2.11 | 18 | 4.67 | |
| Mar-12 | 10 | 1.37 | 25.2 | 3.5 | 70 |
Table 1: Biochemical tests before and after hospitalization.
The treatment included hyperhydration; administration of furosemide, corticosteroid, and iron; and replacing erythropoietin by methoxy polyethylene glycol-epoetin beta due to suspected skin allergy. Intranasal and subcutaneous calcitonin was also introduced [9].
ii) A 70-year-old female, known hypertensive for thirty-five years and diabetic for seven years underwent total knee replacement (TKR) for osteoarthritis left knee in December 2010. For perioperative glycaemic control, multiple subcutaneous injections of insulin were advised. Patient later presented with poor glycaemic control, decreased appetite, and constipation for last 1 month with history of episodes of transient loss of consciousness for 15 days and recurrent vomiting. Biochemical work-up showed hypercalcemia (Serum calcium 12.4 mg/dL). Sr. albumin, ALP, Sr. phosphorus and PTH levels were normal, thus suggesting PTH independent hypercalcemia. A check of vitamin D levels were 2016 ng/mL, thus confirming vitamin D toxicity. Retrospective analysis of treatment history revealed patient receiving 4 injections of Architol (6 Lac units IM injections) prior to presentation. Work-up for malignancy was negative, brain imaging and EEG were normal. Holter was suggestive of intermittent CHB. Patient was given hydration, injection calcitonin 100 I.U. subcutaneously, injection pamidronate 60 mg infusion, with serum calcium levels normalizing, with relief in constipation, vomiting and behavioural improvement. However, persistence of rhythm disturbances led to permanent pacemaker placement. (Vitamin D toxicity presenting as hypercalcemia and complete heart block [10] (Tables 2 & 3).
| Mechanism | Category | Examples | ||
|---|---|---|---|---|
| Excessive bone resorption | Humoral hypercalcemia of cancer | Bladder, Breast, Leukaemia, Lymphoma, Ovarian, Prostate, Renal cell, Squamous cell (lung, head and neck) | ||
| Osteolytic hypercalcemia of cancer, due to bone metastases or hematologic cancer | Leukaemia, Lymphoma, Metastatic breast, prostate, non-small cell lung cancers, Multiple myeloma | |||
| Increased mobilization of calcium from bone | Hyperthyroidism, Immobilization (eg, orthopaedic casting traction), Osteoporosis in older people, Paget disease of bone, Paraplegia or quadriplegia, Rapid growth during childhood and adolescence | |||
| Parathyroid hormone excess | Familial hypocalciuric hypercalcemia, Parathyroid carcinoma, Tertiary hyperparathyroidism | |||
| Vitamin toxicity | Vitamin A toxicity, Vitamin D toxicity | |||
| Excessive GI calcium absorption, intake, or both | Sarcoidosis and other granulomatous diseases | Berylliosis, Coccidioidomycosis, Histoplasmosis, Leprosy, Silicosis, Tuberculosis | ||
| Other disorders | Milk-alkali syndrome, Vitamin D toxicity | |||
| Other mechanisms | Drugs | Lithium toxicity, Theophylline toxicity, Thiazide treatment | ||
| Endocrine dysfunction | Addison disease, Cushing disease, postoperative Myxoedema | |||
| Other disorders | Aluminium-induced Osteomalacia, Idiopathic infantile hypercalcemia, Neuroleptic malignant syndrome | |||
| Artefactual | Exposure of blood to contaminated glassware, Prolonged venous stasis as blood sample was obtained | |||
| Intervention | Mode of action | Dose | Adverse effects | |
| Rehydration with NS followed by loop diuretics | ||||
| IV normal saline1.2 | Enhances GFR and renal excretion of Ca2+ | 200-500 mL/h or 2-4 L/d for 1-3 days depending on the patient’s cardiovascular and renal status | Volume overload; may exacerbate heart failure | |
| Furosemide | Inhibits Ca2+ resorption in the renal tube | 20-40 mg IV, after rehydration has been achieved | Hypokalemia, renal failure, and abnormalities of cardiac conduction | |
| First-line medications: intravenous bisphosphonate | ||||
| Pamidronate | Inhibits osteoclast activity: decreases bone resorption | 60-90 mg IV over 2-4 hours as a single dose in a solution of 50-200 mL NS or D5W (allow at least 7 days before retreatment) | Nephrotoxicity; flulike symptoms with fever, chills, and headache | |
| Zoledronic acid 1,2,5 | 4 mg IV over 15 minutes in a solution of 50 mL NS or D5W | |||
| Denosumab | Inhibits RANKL to decrease osteoclast activity | 120 mg SQ every 4 weeks: administer additional 120 mg on days 8 and 15 during the first month | Hypertension, fatigue, nausea, arthralgia, and hypocalcemia | |
| Second-line medications | ||||
| Glucocorticoids | Inhibits vitamin D conversion to calcitriol | Oral prednisone 20-40 mg/d for 10 days, intravenous hydrocortisone 200 mg daily for 3 days or equivalents | Immune suppression, myopathy, elevated blood glucose, weight gain, and elevated blood pressure | |
| Calcitonin | Inhibits bone resorption | 4-8 10/kg SQ or IM every 12 hours | May rebound: elevated Ca2* after 24 hours; causes vomiting, cramps, and flushing | |
| Gallium nitrate1,2,2 | Inhibits osteoclast activity | Intravenous continuous infusion at 100-200 mg/m2 over 24 hours for 5 days | Bone marrow suppression; nephrotoxicity | |
Table 2: Key Causes of Hypercalcaemia.
• A Case of Constipation due to hypercalcemia secondary to TB in Dharwad, Karnataka: A 75-year-old monk was admitted to SDM College of Medical Sciences and Hospital, Sattur, Dharwad-580009, Karnataka, India in 2014 with complaints of constipation for the past 3-4 months who was on Laxatives and intermittent enema with partial benefit. He had mild anorexia and no significant weight loss.
On examination he was well built and moderately nourished elderly male with borderline hypertension. Systemic examination revealed mild right sided pleural effusion and other systems were unremarkable.
Investigations revealed normal hemogram, normal thyroid function studies, mild renal dysfunction, normal urinalysis, and moderate Hypercalcemia.
He was treated with hydration for hypercalcemia but was not getting optimized & renal failure was worsening. The intact parathyroid hormone (PTH) was low suggestive of non-PTH related hypercalcemia. His Vitamin D3 {1, 25 (OH) 2} level was available after a week which was very much elevated.
HRCT Chest showed multiple nodular lesions along the broncho-vascular bundles, in both upper lobes, right middle lobe and anterior segment right lower lobe. Fibrotic streaks were also noted in bilateral apical region. Few calcified bilateral hilar lymph nodes noted.
A provisional diagnosis of sarcoidosis was made, and he was put on prednisolone (0.5 mg / Kg / day). After 4 days of starting prednisolone, he started having high grade fever with chills and cough with expectoration. His sputum samples were positive for acid fast bacilli and hence was put on Anti-Tuberculous Therapy (ATT). After about 15 days of starting steroids and 1 week of ATT his fever subsided, sensorium improved. His hypercalcemia and renal dysfunction normalized. His constipation got relieved.
Steroids were withdrawn completely at the end of 4 weeks. He completed the full course of ATT for 6 months and at the completion of ATT he was free from constipation, renal functions remained normal and there was no hypercalcemia.
Hypercalcemia is seen in ~ 25 % cases of tuberculosis but ~ 7 to 12 % cases only are symptomatic. Hypercalcaemia is not uncommon among patients with newly diagnosed TB, but rarely symptomatic.
Hypercalcemia in sarcoidosis is secondary to increased synthesis of 1, 25 (OH) Vitamin D3 by the activated macrophages [10, 11].
Discussions
Many organs are involved in the regulation of calcium. Chief among these are the parathyroid glands and, when calcium levels drop, the parathyroid glands increase secretion of parathyroid hormone (PTH). Vitamin D, which is partially regulated through PTH, also plays an important role in the regulation of calcium. The first step of vitamin D metabolism occurs at the skin- ultraviolet light catalyses the production of Vitamin D3, (cholecalciferol), from 7-dehydrocholesterol. Cholecalciferol is then hydroxylated at the 25 positions by the liver to form 25-hydroxycholecalciferol (called calcifediol). Calcifediol is then hydroxylated at the 1 position in the kidney to form 1,25-dihydroxycholecalciferol (calcitriol). This final step is regulated by PTH, and calcitriol is the active form of vitamin D. Calcitriol increases serum calcium by causing increased calcium absorption in the intestines, increased calcium reabsorption in the kidneys, and stimulation of osteoblasts to reabsorb calcium from bone (Figure 2).
![Figure 2: Hypercalcemia-Causes, Signs, Symptoms, Workup, Treatment [Source-3].](/fulltextimages/9511/fig_2.png)
Differential Diagnosis of Hypercalcaemia
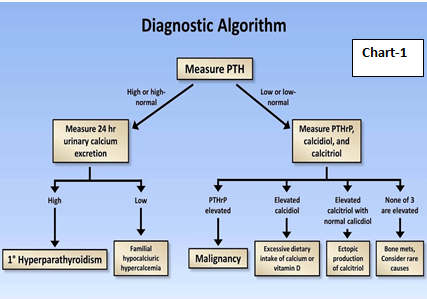
The differential diagnosis of hypercalcemia consists of A) Parathyroid hormone (PTH)-mediated hypercalcemia and B) non-PTH-mediated hypercalcemia. Causes of PTH-mediated hypercalcemia include primary hyperparathyroidism, familial hypocalciuric hypercalcemia, and ectopic PTH secretion. Causes of non-PTH-mediated hypercalcemia comprise vitamin D-mediated hypercalcemia (vitamin D intoxication, lymphoma, granulomatous diseases), vitamin A intoxication, hyperthyroidism, drug-induced hypercalcemia (hydrochlorothiazide, theophylline, and lithium), immobilization, milk-alkali syndrome, adrenal insufficiency, and humoral hypercalcemia of malignancy (Figure 3).
- Pathophysiology: True hypercalcemia occurs through three basic mechanisms: i) enhanced osteoclastic bone resorption (in local osteolytic hypercalcemia, HHM, 1,25(OH)2D-secreting lymphomas, and the rare case of ectopic hyperparathyroidism); ii) enhanced renal tubular reabsorption of calcium (in HHM and ectopic hyperparathyroidism); and iii) enhanced intestinal absorption of calcium (in 1,25(OH)2D-secreting lymphomas and possibly ectopic hyperparathyroidism).
- Diagnosis: The diagnosis of hypercalcaemia is made when the corrected serum calcium concentration is 2 standard deviations above the mean of values found in people with normal calcium levels, in at least two samples at least one week apart over a period of three months. The presence of high or not adequately suppressed serum parathyroid hormone levels should point the diagnosis towards hypercalcaemia of parathyroid origins.
- Management Principles: When biochemical screening is common, asymptomatic primary hyperparathyroidism is the most likely form of the disease. In countries where vitamin D deficiency is prevalent and biochemical screening is not a feature of the health care system, symptomatic disease with skeletal abnormalities is likely to predominate. When PTH levels are part of the evaluation for low bone mass, the normo-calcaemic variant is seen. Guidelines for surgical removal of hyperfunctioning parathyroid tissue apply to all three clinical forms of the disease (Figure 4).
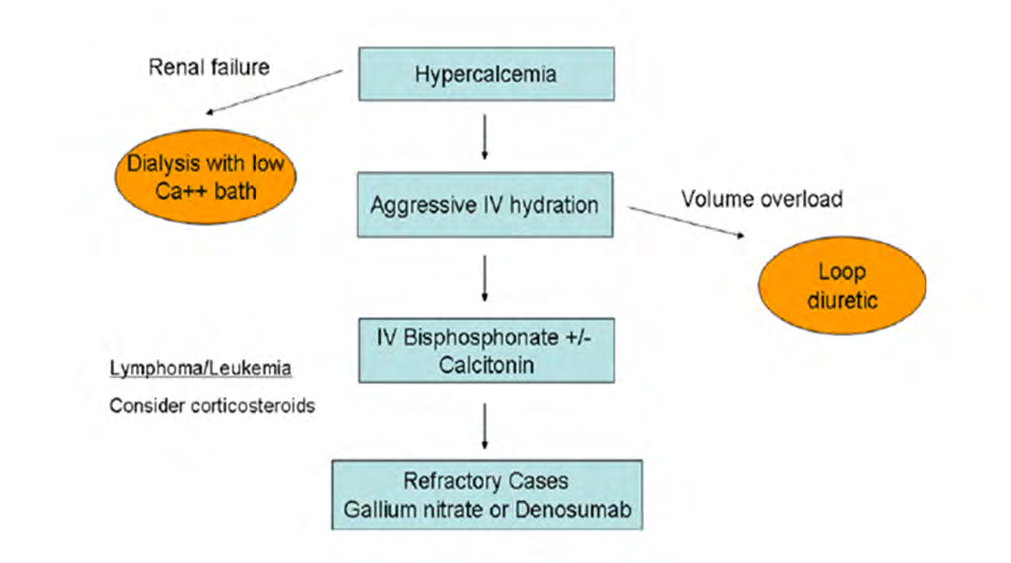
• Standard Treatment: Mild hypercalcaemia is usually caused by primary hyperparathyroidism, and the treatment for which is typically surgery. Persons aged 50 or more with serum calcium levels <0.25 mmol/L above the upper limit of normal and without end organ damage may be followed up conservatively. Treatment with a calcimimetic agent, cinacalcet, is an option in selected cases. Severe hypercalcaemia requires admission to hospital and treatment with aggressive intravenous hydration and bisphosphonates along with treatment of the underlying disease.
ICD 10 Classification
In International classification (10) the hypercalcaemia is categorised under Disorders of mineral metabolism. E-83- Disorders of Mineral Metabolism, E83.50 - Unspecified disorder of calcium metabolism, E83.51 – Hypocalcaemia [4].
E 83.52 Disorders of Calcium Metabolism, - Hypercalcaemia, hypocalciuric, familial E83.52, Milk-alkali disease, or syndrome, Burnett’s syndrome, Dementia (degenerative primary/ old age/ persisting) due to hypercalcemia with behavioural disturbance.
E83.59 - Other disorders of calcium metabolism [4]
Prevention: Not all hypercalcemia can be prevented but avoiding excess intake of calcium pills and calcium-based antacid tablets is recommended [3].
Primary Hyperparathyroidism
Primary hyperparathyroidism (PHPT), the most common cause of hypercalcemia, is often identified in postmenopausal women with hypercalcemia and parathyroid hormone (PTH) levels that are either frankly elevated or inappropriately normal. PHPT can present as adenoma (85%), hyperplasia (14%) or carcinoma (1%) with 1% of the adult population and incidence increasing to 2% after the age of 55 years.
Three types of clinical presentation are: 1.Target organ involvement of the renal and skeletal systems. 2. Mild asymptomatic hypercalcemia; and 3. High PTH levels in the context of persistently normal albumin-corrected and ionized serum calcium values.
A recent study indicates that about 36.1%) PHPT patients had normocalcaemic PHPT and 63.9% were hypercalcaemic. The study proposes use of Ca/P ratio as better biomarker for Hyperparathyroidism [12].
The factors that determine the incidence in each country are a) extent to which biochemical screening is employed, b) the prevalence of vitamin D deficiency, and c) whether a medical centre or practitioner tends to routinely measure PTH levels in the evaluation of low bone density or frank osteoporosis.
• Primary Hyperparathyroidism In India: A cocktail of contemporary and classical presentations: Lesson from 47 cases (A retrospective, review of clinical, biochemical, and histopathological data of all 47 patients with PHPT between January 2008 and June 2012 indicated that the mean age and the duration of the disease were 43 years (9-78 years) and 5.5 years (3 months to 8 years), respectively. Female to male ratio was 2.1:1. Common presenting features were bone pains (86%), fatigue (96%) and abdominal pain (27%). The other manifestations included nephrolithiasis (49%) fracture (40.4%) and pancreatitis (27%). Rare presentations including behavioural disturbances, seizures, encephalopathy, arrhythmias, myopathy, oliguria, intractable constipation and paraparesis. Few patients were also misdiagnosed as rheumatoid arthritis, sciatica, and lumbar spondylosis.
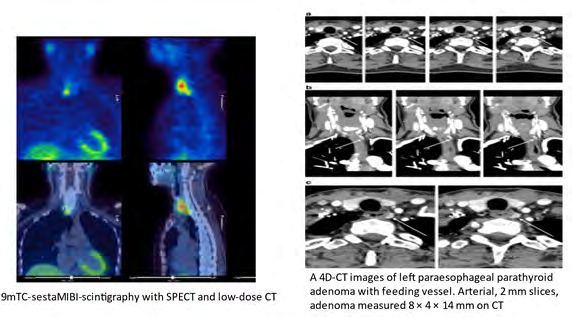
The mean corrected serum calcium, phosphorus, PTH and vitamin D level were 12.69 mg/dl, 2.55 mg/dl, 807.87 IU/land 26.89 ng/dl, respectively. Sestamibi scan diagnosed parathyroid adenoma in all except four cases. The diagnosis in this study was based on {(1) Persistent elevation of serum calcium above the upper limit of normal; (2) increased circulating intact PTH; and (3) histological evidence of parathyroid adenoma or hyperplasia. Serum calcium and phosphorus levels were measured by ion-specific electrode and phosphomolybdate ultraviolet method, respectively. Serum intact PTH levels and 25(OH) vitamin D levels were measured by Radioimmunoassay [12, 13].
• Hypercalcemia-induced AKI in a tertiary care Center from northern India: A prospective observational study conducted on 30 patients in the Department of Medicine in a tertiary care centre from J & K, India, from June 2010 to June 2012. Patients admitted with hypercalcemia were assessed for AKI, evaluated & treated for hypercalcemia, monitoring renal function during hospitalization and at 1 month of discharge.
Hyperparathyroidism and multiple myeloma accounted for 13(43.3%) and 10 (33.3%) cases, respectively. Mean ±SD corrected serum calcium at diagnosis & after treatment at 1 month was 13.56 ± 1.86 mg/dl & 9.49±1.35 mg/dl, p < 0.001. Mean ±SD serum creatinine at baseline and after treatment of hypercalcemia was 2.87 ±1.68 mg/dl and 1.49±1.34 mg/dl, p < 0.001. Twenty-three (76.7%) patients had AKI. AKI recovered after treating hypercalcemia in 25 (83.3 %) patients. Mean ± SD days taken for the decrease in serum creatinine to ≤ 1.5 mg/dl was 8.28 ± 4.17 days. Mean ± SD serum creatinine after treatment of hypercalcemia in hyperparathyroidism group versus non-parathyroid group was 0.97 ± 0.35 mg/dl and 1.88 ±1.67 mg/dl, respectively: p value 0.009 [13].
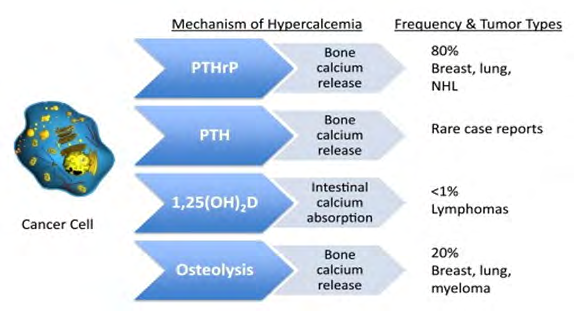
• Hypercalcemia of Malignancy: Hypercalcemia is the most common life-threatening metabolic disorder associated with cancer, commonly seen in later-stage malignancies and predicts a poor prognosis. Hypercalcemia -reported to occur in up to 20 -30 % of patients with cancer during their disease. The most common causes include humoral hypercalcemia of malignancy mediated by parathyroid hormone–related peptide, osteolytic cytokine production, and excess 1,25-dihydroxy vitamin D production [5, 7] (Figure 5).
Symptoms include Loss of appetite, Nausea and vomiting, Constipation and abdominal (belly) pain, The need to drink more fluids and urinate more, Tiredness, weakness, or muscle pain, Confusion, disorientation, and difficulty thinking, Headaches, Depression (Figure 6).
The diagnosis depends on combination of history, physical examination, imaging, and pathologic analysis of tumour. There is no confirmatory test for hypercalcemia related to local actions of malignancies on bone. Humoral hypercalcemia of malignancy (HHM) is caused by the over secretion of parathyroid hormone-related peptide (PTHrP) from malignant tumours. Bisphosphonate therapy is initiated as soon as hypercalcemia is detected, and it takes 2 to 4 days to lower the calcium levels. Two bisphosphonate agents 1) Pamidronate (Aredia) and Zoledronic acid (Zometa).
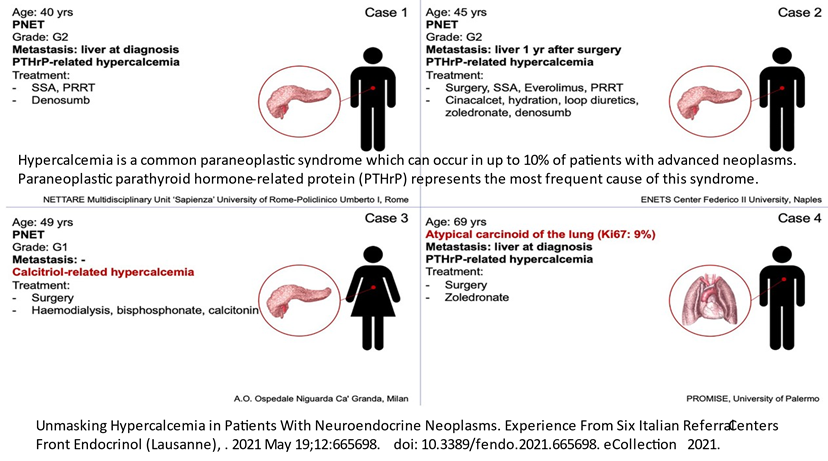
• Paraneoplastic syndromes associated with lung cancer: Hypercalcemia is a common paraneoplastic syndrome which can occur in up to 10% of patients with advanced neoplasms. Paraneoplastic parathyroid hormone-related protein (PTHrP) represents the most frequent cause of this syndrome. As the optimal therapy for hypercalcemia associated with cancer is one that is tailored both to the degree of hypercalcemia and to its underlying cause. Therapy is targeted accordingly. Most common are 1) humoral hypercalcemia of malignancy (HHM) in squamous cell carcinoma (incidence
23%) and 2) the syndrome of inappropriate antidiuretic hormone (SIADH) secretion in small cell lung cancer (SCLC).
There is no relation between the severity of symptoms and the size of the primary tumour, and in some cases, paraneoplastic syndromes are manifested before the diagnosis of cancer.
The incidence of hypercalcemia in patients with lung cancer ranges from 2%-6% initially to 8%-12% throughout the course of the disease.
The two major mechanisms of hypercalcemia in cancer patients are: (1) HHM; and (2) osteolytic activity at sites of skeletal metastasis.
HHM is considered a paraneoplastic syndrome and accounts for 46%-76% of hypercalcemia in lung cancers. Four mechanisms of HHM have been described; the majority of HHM cases are caused by the secretion of parathyroid hormone (PTH)-related protein (PTHrP) from the tumour.
SIADH manifests as euvolemic hypo-osmolar hyponatremia characterized by low serum osmolality and inappropriately high urine osmolality in the absence of diuretic treatment, adrenal insufficiency, heart failure, cirrhosis, or hypothyroidism. Clinical SIADH has been reported to occur in 7%-16% of SCLC cases. A paraneoplastic manifestation of SCLC was first reported in 1975, after an autopsy of a patient who had abdominal pain and obstipation revealed autonomic neuropathy limited to the gastrointestinal tract.
Currently, treatment for these syndromes fundamentally consists of direct therapies aimed at the underlying lung cancer. In the era of molecular-targeted therapy, newly developed drugs have resulted in favourable outcomes in some cases. Remarkable progress is occurring in the development of molecular-targeted therapies for paraneoplastic syndromes [14, 15, 16].
• Hypercalcemia due to Acute Kidney Injuries: Hypercalcemia is known to decrease the glomerular filtration rate and cause acute kidney injury causing AKI. Hypercalcaemic AKI with primary hyperparathyroidism is less common and the outcome is better, as compared to non-hyperparathyroidism-related causes. AKI is reversible in most cases.
The differential diagnosis of hypercalcemia consists of parathyroid hormone (PTH)-mediated hypercalcemia and non-PTH-mediated hypercalcemia. Causes of PTH-mediated hypercalcemia include primary hyperparathyroidism, familial hypocalciuric hypercalcemia, and ectopic PTH secretion. Causes of non-PTH-mediated hypercalcemia comprise vitamin D-mediated hypercalcemia (vitamin D intoxication, lymphoma, granulomatous diseases), vitamin A intoxication, hyperthyroidism, drug-induced hypercalcemia (hydrochlorothiazide, theophylline, and lithium), immobilization, milk-alkali syndrome, adrenal insufficiency, and humoral hypercalcemia of malignancy [13].
• Hypercalciuria due to Vitamin D intoxication Vitamin D deficiency exacerbates primary hyperparathyroidism and vice versa. With care, vitamin D supplementation can safely be given to selected patients with asymptomatic primary hyperparathyroidism and is suggested before deciding on medical or surgical management. Clinical conditions associated to vitamin D intoxication were scarcely reported a decade ago. The number of cases has recently increased because of more prescriptions of vitamin D to treat hypovitaminosis D. Hypercalcemia is suggestive of presumptive diagnoses of Vitamin D intoxication. The cases presented highlight the dangers of indiscriminate vitamin D usage, exposing patients to potentially life-threatening complications [8].
- Hypercalcaemia secondary to Tuberculosis / sarcoidosis: Hypercalcemia is seen in ~ 25 % cases of tuberculosis but ~ 7 to 12 % cases only are symptomatic. Hypercalcaemia is common among patients with newly diagnosed TB, but rarely symptomatic. Hypercalcemia in sarcoidosis is secondary to increased synthesis of 1, 25 (OH) Vitamin D3 by the activated macrophages [10]. 1. Conclusions
- Hypercalcaemia is a biomarker for detecting hyperparathyroidism currently with major morbidity and serious complications. Assessing ionized, calcium levels is the method of choice when hypercalcemia is suspected but costly and rarely available in smaller towns. If biochemical screening becomes a national norm, asymptomatic primary hyperparathyroidism will be the most likely form of hypercalcaemia to be unmasked.
- Incidentally detected hypercalcemia is most likely caused by primary hyperparathyroidism.
- In countries where vitamin D deficiency is prevalent and biochemical screening is not a feature of the health care system, and indiscriminate and rampant use of Vit D supplementation for diabetes management is leading to an increase in Vitamin D intoxication in the last decade in developing countries including India where symptomatic disease with skeletal abnormalities is likely to predominate.
- Physicians and Laboratory science in developing countries including India need to develop a high index of suspicion because PHT escapes diagnosis due to the subnormal calcium and PTH levels assessment facilities. If PTH levels are part of the evaluation for low bone mass, the normo-calcaemic variant is seen. In such situation Ca/P ratio is the best indicator for detecting Normocalcaemic hyperparathyroidism.
- Ca/P ratio is a valuable tool for the diagnosis and screening of PHPT in combination with serum Ca levels and is of superior value compared to serum Ca alone, especially in normo-calcaemic hyperparathyroidism cases (NCPHT). Ca/P is simple, inexpensive, and easily accessible worldwide, especially in laboratory/medical settings relying on limited resources.
- Not all hypercalcemia can be prevented but avoiding excess intake of calcium pills and calcium-based antacid tablets is recommended.
- Surgical removal of hyperfunctioning parathyroid tissue apply to all three clinical forms of the disease [17].
- Hypercalcemia a biomarker in a patient with cancer may be severe enough to warrant hospitalization, as it could be fatal. Hypercalcemia of malignancy is mostly mediated by tumoral production of parathyroid hormone–related protein or by cytokines activating osteoclast degradation of bone. Clinical features include polyuria, constipation, muscle weakness, confusion, and coma.
- Diagnosis is by measuring serum ionized calcium and parathyroid hormone concentrations.
- Treatment to increase calcium excretion and reduce bone resorption of calcium involves infusion of saline, sodium diuresis, and drugs such as zoledronate.
References
-
Silva B (2018) Best Practice & Research Clinical Endocrinology & Metabolism. 32(5): 593-607.
-
Alina G Sofronescu (2019) Serum Calcium levels.
-
Malignancy-Related Hypercalcemia.
-
2022 ICD-10-CM Diagnosis Code E83.52, Hypercalcemia.
-
Meena DS (2020) Hypercalcaemic Encephalopathy as an Initial Presentation of Multiple Myeloma. Case Rep Emerg Med 2020: 4746865.
-
Garg G (2012) Vitamin D toxicity presenting as hypercalcemia and complete heart block: An interesting case report. Indian J Endocrinol Metab 16(S2): S423-S425.
-
Sigvaldason H (2016) Hypercalcemia in metastatic breast cancer unrelated to skeletal metastasis, CMAJ 188(5): E91-E94.
-
Marins TA (2014) Vitamin D intoxication: case report, Einstein 12(2): 242-244.
-
Kumar R (1991) Vitamin D and calcium transport. Kidney Int 40(6): 1177-1189.
-
Kashinkunti M (2014) An Unusual Case of Constipation Unmasking Underlying Tuberculosis: Case Report. Sch J Med Case Rep 2(8): 578-580.
-
Medio B (2018) Serum Calcium to Phosphorous (Ca/P) Ratio Is a Simple, Inexpensive, and Accurate tool in the Diagnosis of Primary Hyperparathyroidism. JBMR Plus 2(2): 109-117.
-
Mackey R (2020) Dept. of Endocrinology, Sir Ganga Ram Hospital, New Delhi, India.
-
Aziz Bhat N (2018) Incidence, aetiology, and course of hypercalcemia-induced AKI in a tertiary care centre from northern India.
-
Bohra GK (2020) Hypercalcemic Encephalopathy as an Initial Presentation of Multiple Myeloma. Case Report. 2020: 4746865.
-
Kanaji N (2014) Paraneoplastic syndromes associated with lung cancer, World J Clin Oncol 5(3): 197-223.
-
Giannetta E (2021) Unmasking Hypercalcaemia in patients with neoplasms, Front Endocrinol (Lausanne). 12: 665698.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda