A Review of the Efforts Made by Several African Countries to Reach UNAIDS Targets and the Effects of the Covid-19 on People Living with HIV
Even though COVID-19 has spread faster than any other health problem in the last 100 years, it is not the first pandemic that the modern world has had to deal with. As countries try to deal with the COVID-19 pandemic, which is getting worse and worse, they are already using what they have learnt and invested in while dealing with HIV by putting systems to use, and figuring out what dynamic changes are needed to build a new way forward towards health systems that are optimally effective, accountable, inclusive, fair, and well-resourced, with services that are accessible, integrated, tailored, and people-centred. The COVID-19 pandemic has had a lot of terrible effects on people, communities, and societies all over the world. People with long-term health problems may be more likely to get COVID-19 or have complications from it. People who get the virus can get sick or die, and the physical distance needed to flatten the curve of new cases is hurting the economy. This hurts the economy in ways that affect mental health and other health problems, which particularly hurts marginalised communities. COVID-19 is affecting people with HIV (PWH) in unique ways, and it will continue to influence HIV research and treatment after the COVID-19 crisis is over. This is because HIV affects marginalised communities more than other groups.
Introduction
The pandemic of coronavirus (COVID-19) is a global public health emergency. On December 31, 2019, it first appeared in Wuhan, China, and has since spread around the world. Since the incidence of the first case of COVID-19 in Ethiopia on March 13, 2020, the virus has had a profound effect on all aspects of human life. The crisis is mostly attributable to failures in the health care delivery system (COVID-19) [1, 2, 3]. Until recently, chronic diseases such as HIV were the leading cause of morbidity and mortality worldwide. Sixty percent of all deaths globally are attributable to chronic illnesses. HIV/AIDS is one of the primary causes of death, accounting for over 690,000 deaths per year, worldwide. An estimated 37.6 million persons worldwide were infected with HIV in 2020, with an additional 1.3 million adults and 160,000 children being infected [4, 5]. Of those living with HIV/AIDS 16 percent were not even aware of their HIV status, 27 percent were unable to obtain antiretroviral therapy (ART), and 34 per cent of those on ART did not have viral suppression.
Of the HIV-positive individuals 55 percent live in Eastern and Southern Africa. Ethiopia is one of the countries in eastern Africa with an exceptionally high HIV/AIDS burden. Significant progress has been made in reducing the burden of HIV, in order to meet targets for reaching extremely low levels of HIV burden by 2030. Even though the Ethiopian government and its supporters have made significant efforts to reduce HIV related deaths and illnesses, HIV/ AIDS continues to be a significant problem in Ethiopia [5, 6]. Approximately 0.9 percent of individuals aged 15 to 49 have HIV, according to the Joint United Nations Programme on HIV and AIDS (UNAIDS) data from 2018.
Compared to the general population, HIV-positive people are twice as likely to die from the COVID-19 pandemic. UNAIDS has found that the COVID-19 pandemic has interrupted worldwide efforts to fight HIV/AIDS. COVID-19 poses a grave threat to HIV-positive individuals and the global response to the virus, including restrictions on population movement and the suspension of health services out of concern for the infection’s spread. It has been asserted that COVID-19 will disrupt up to 75 percent of HIV services in multiple regions [7, 8, 9]. The direct influence of COVID-19 on HIV prevention efforts could have led to catastrophic failures. During the COVID-19 outbreak, HIV related mortality may increase considerably if worst-case forecasts regarding HIV care delays are accurate. Ethiopia is attempting to adjust to the COVID-19 pandemic by emphasising the immediate and ongoing needs of HIV-positive individuals [10]. Ethiopia did a national inventory assessment in December 2020, and the results showed that 82 percent of Anti Retro Virals (ARVs) and all HIV test kits had more than six months of supply with no risk, and 14.2 percent had four to six months of supply with low risk. Out of the 308,522 adults who are eligible for ART, about 195,237 are enrolled on the first-line regimens as of September 2020 [11, 12, 13]. During the lockdown in Zambia, the number of HIV tests dropped by 35 percent. In the lockdown in Ethiopia, the HIV service was also severely disrupted. Since COVID-19 infection has been Ethiopia’s main focus since the first local cases were found, and as COVID-19 prevention measures became stricter, people were told to stay home and not go to the hospital. Public gatherings were also limited to stop the virus from spreading. Problems with key HIV supplies, logistics, and reporting systems made it harder to keep HIV related services going. In another area, governments cut funding for HIV programmes that got direct help because they needed to focus on COVID-19. This has had a direct effect on how HIV programmes are put into place [12, 13].
Impact of Covid-19 on HIV Care Delivery
The COVID-19 pandemic made HIV care delivery around the world face problems that have never been seen before, and threatened years of progress in HIV testing and treatment. In several countries, people living with HIV (PLWH) are less likely to get care because they are worried about getting COVID-19. The reasons for this is not surprising. People who have been stigmatised for decades because they have HIV and live with a chronic virus are reluctant to get care when there is a chance in the process, they could get infected with another, more deadly virus. Some people even wondered if it was safe to get ARTs from pharmacies because of this fear [14, 15, 16, 17]. Access to care was also greatly hampered by national lockdowns. In Uganda, the suspension of public and private transportation across the country made it nearly impossible for many people to get to clinics in faraway places.
Migrant workers in cities have moved back to the rural areas where they grew up, which means that they may no longer have access to HIV care in the cities where they lived. Even when people can get to clinics, losing their jobs makes it hard for them to pay for care [17, 18, 19, 20]. Lastly, physical distance rules can make it even harder for older people with HIV to connect with others. Even though there is no solid proof that PLWH have a higher chance of getting COVID-19, some people may worry that they do, which could cause them to come to care later than they should. Depression is the second most common mental health disorder among PLWH (after substance use), and it is another barrier to care. The ongoing pandemic is a big stressor that is likely to make PLWH’s already high rate of mental health problems even worse [21, 22, 23].
The pandemic is putting a lot of pressure on healthcare systems all over the world. In Eastern Europe, doctors who specialise in HIV have been asked to treat people with COVID-19, which has led to a shortage of staff. This has caused some clinics to stop letting people come in person, others to put off blood tests, and others to only focus on giving out ARTs. At the same time, PLWH who got care elsewhere but could not go home because of travel restrictions came to these already full clinics [24, 25, 26, 27].
These problems make it harder for clinics to find people with drug-resistance, quickly diagnose opportunistic infections, and do regular blood tests. This makes it harder to get high risk people who want to be tested for HIV connected to care, making it impossible to ‘test and treat’ in a timely manner. Studies using computer models show that even a three-month break in the supply of ARTs can cause half a million HIV/AIDS related deaths in Africa alone, reversing years of progress [28, 29]. The same problems that affect HIV care are also affecting tuberculosis (TB) care. TB is the leading cause of death among PLWH, and modelling studies show that even short-term problems with diagnosing and treating TB can increase the number of cases and deaths from HIV for many years.
One of the main ways to stop the spread of COVID-19 has been to encourage people to “shelter in place” or quarantine themselves at home. However, prolonged contact within a household can lead to the spread of TB, which has a long incubation period, so one might not see the effect on the number of TB cases for months or even years [30, 31].
Lastly, putting more focus on COVID-19 should not take away from giving PLWH their annual flu vaccine and pneumococcal vaccines on time, as recommended by guidelines. Even though there are so many big problems, this pandemic gives us a chance to speed up changes in care delivery that are very much needed. Multiple-month prescriptions are now common in several African and Eastern European countries. This has the obvious downside of making it harder to track viral load and CD4 counts, but it also gives point-of-care testing solutions a chance to improve [32, 33]. Going forward, countries should try to keep a steady supply of ARVs and anti-TB drugs, especially if they are only available through imports. Notably, South Africa did not increase the number of prescriptions for more than one month because they were worried about ART shortages. This was needed to protect health systems from shocks from the outside, especially in places where HIV/TB was common [34].
Lastly, solutions must be made for each location. For example, telemedicine visits help keep patients’ access to their doctors, who are then able to offer consistent assistance in places with a lot of resources. In places with few resources, spreading out HIV testing will make it easier for people to get care and will free up larger hospitals; thus allowing them to focus more on the sickest patients. In Spain, some non-governmental organisations collect medications for people and deliver them to their homes. This can be especially helpful for elderly people who are already at high risk of getting COVID-19. The rapid spread of SARS- CoV-2 around the world has created problems for health systems that have never been seen before. This means that the goal of fewer than 500,000 HIV/AIDS related deaths each year by 2020 will not be met, but if HIV/AIDS programmes are not given enough attention during the global pandemic, years of progress could be lost [34, 35, 36].
Impact of COVID-19 on Access to HIV Services
COVID-19 is not only directly causing a lot of illness and death. It is also messing up important health systems and hurting programmes that are trying to fight HIV and affecting other global health priorities. The global response to HIV depends a lot on generic medicine makers in India. In May 2020, India started to come out of a national lockdown that was put in place to stop the spread of COVID-19. As the Global Fund to Fight AIDS, TB, and malaria (Global Fund) said, COVID-19 control measures at the point of origin and destination for essential health commodities are already causing significant delays in the delivery of medicines and other health commodities [37, 38]. Repurposing HIV clinics and health care workers, limiting travel, sending messages that keep people away from services, new human rights abuses, and worsening social and economic conditions are also causing problems with providing continuity of services. Service interruptions caused by COVID-19 are hurting efforts around the world to end the HIV, TB, and malaria epidemics. According to simulations done by the HIV Modelling Consortium, in collaboration with the World Health Organisation (WHO) and UNAIDS, a 50 percent disruption in HIV treatment for six months could cause 300,000 more AIDS related deaths in sub-Saharan Africa over the course of a year [14, 39]. In 2019, 440, 000 people in this region died from AIDS related illnesses, so this brings us back to AIDS related mortality levels in 2011.
In high-burden countries, new HIV infections among children could rise by 40–80 percent if programmes to stop HIV from being passed from mother to child were to stop working for six months. This report shows how the HIV response can help jumpstart an accelerated, effective response to COVID-19 in ways that could help make sure that these efforts do not hurt other important health priorities. At the same time the world is working hard to stop the spread of COVID-19, it must redouble its efforts to make sure that HIV and other global health priorities always have access to essential goods and services [36, 40, 41].
To keep HIV services from being interrupted by the COVID-19 crisis, people will need to be flexible and committed. Partners who focus on HIV can learn important new lessons as they work to keep HIV responses going in the middle of a complex global health emergency that is always getting worse. Since current spending on HIV is much slower than what is needed to reach the Fast Track Targets to end the AIDS epidemic, the world needs to invest a lot more in fighting both HIV and COVID-19 [42, 43].
Implications of COVID-19 for HIV Treatment in the Short- and Long-Term
The global spread of COVID-19 has had a major impact on people’s daily routines. Major disturbances to everyday life resulted from the presence of the virus, which has led to the implementation of physical separation and the closure of schools and companies. Given that humans are social creatures, they are discovering new ways to live with COVID-19. Health care professionals (e.g., physicians, psychologists, social workers, case managers, etc.) must take into account not only the immediate consequences of COVID-19, but also the long-term implications for PWH and the provision of health care therapy [43]. Adjusting to COVID-19 may have far-reaching consequences for the physical, mental, and social health of PWHs [43, 44]. Individuals living with HIV who do not have their condition effectively controlled are at higher risk for developing COVID-19 and other HIV related co-morbidities. Since HIV is incurable, it is crucial that PWHs maintain consistent contact with their healthcare professionals and take their medication as directed. There is a risk that PWH’s therapy will be disrupted or altered if they are required to stay at home.
To meet federal regulations, many American doctors have switched to virtual visits with patients [44, 45]. It is possible that those who are currently living with HIV will not be able to get all the help they need due to the limitations of telehealth programmes. Lack of access to technology, poor knowledge of telehealth, etc. are all factors that may prevent certain PWH from using telehealth services, which might slow down their treatment. Opportunistic infections, such as pneumonia, TB, toxoplasmosis, and so on, are more common in PWH than in those with healthy immune systems. COVID-19 may cause therapy delays for PWH who are having co-morbidities. Overcrowding in hospitals contributes to this problem, especially in a healthcare system that is already stretched thin. Urgent care patients are at risk for catching COVID-19 and other diseases that are spread in hospitals [38, 46].
Since the COVID-19 epidemic is unlike any other, widespread fear has developed as a result. The Centres for Disease Control and Prevention also report that those living with chronic illnesses like HIV may have a more intense stress reaction. Having a weakened immune system makes you more susceptible to catching COVID-19, which triggers a severe stress reaction. Increased alcohol consumption is one example of a maladaptive coping mechanism that may emerge during a public health emergency. People living with HIV who use alcohol daily are at a higher risk of mortality and/or alcohol-related health problems than those who do not have HIV [43, 47, 48]. Due to the negative effects of alcohol on the immune system, it may be more difficult for PWH to fight off HIV and COVID-19.
The WHO also found that heavy alcohol use was associated with an increased chance of developing health issues. In addition to a cumulative rise in viral load, drinking alcohol by PWHs has the same effect. Because of this, drunk people are more likely to take chances in the bedroom, and in other ways, such as drinking and driving. PWH may spread the virus through condom-free intercourse if they engage in risky behaviours and their viral load rises. It is possible that Peer Health Workers (PHWs) whose viral load is not well maintained and who do not participate in protective behaviours (such as condom usage) or whose sexual partners are not utilising pre-exposure prophylaxis would have more difficulty maintaining their sexual health when isolated with a love partner (PrEP); and there’s evidence that drinking might make sadness and anxiety worse [49, 50].
A study found that those living with HIV are 2–4 times more likely to experience depression than those who do not have the infection. In addition, 40-42 percent of PWHs also suffer from depression as their primary mental health issue. As a result, the isolation caused by the necessity of geographical separation in the fight against COVID-19 may worsen pre-existing mood disorders. To add insult to injury, those who are poor are disproportionately affected by HIV, making it harder for them to get the help they need because of social isolation (e.g., cellphones, laptops, internet services) [51, 52].
Poor health outcomes, such as decreased immune response and death, have also previously been associated with depression symptoms that may not fulfil diagnostic criteria for a depressive illness in PWH. Research has found that depressive symptoms, such as loss of interest, feelings of worthlessness, and thoughts of death or suicide, may have negative effects on PWH’s desire to take their medications, or engage in the necessary medication management activities that are conducive to a healthy lifestyle; even though the relationship between depression and treatment adherence among PWH may not be causal [53]. As a result, health care clinicians working with depressed PWHs may have to exert more effort in the wake of COVID-19 to encourage patients to continue with prescribed therapies. Many mental health professionals have turned to telehealth in order to continue treating their patients and meet the growing demand for care in this area. Considering the potential benefits of telehealth in improving patient access to treatment and increasing regular appointment attendance, more healthcare providers may decide to maintain their telehealth service offerings in the future [54, 55, 56].
Although telehealth has many potential advantages it also has some drawbacks. For example, clients may be wary of sharing personal information over the internet. Poor internet connections could compromise the quality of the client’s audio and video, and the absence of direct eye contact could hinder the development of a trusting therapeutic relationship. Furthermore, there may be an increase in the number of PWH who seek mental health treatments in the wake of the COVID-19 pandemic, due to the possible implications of psychological problems (e.g., anxiety, depression, PTSD), COVID-19, and health-related concerns among PWH [57, 58, 59]. It is worth noting, though, that not everyone will feel the mental health consequences of COVID-19 right away when the epidemic ends. Therefore, it is probable that in years to come, the number of people in need of physical and mental health treatment to mitigate the financial and emotional fallout from COVID-19 will grow. Short- and long-term global health initiatives should prioritise the prevention, detection, and treatment of mental health disorders [60].
Since both time and distance appear to affect exposure to COVID-19, most international health bodies have introduced guidelines about physical proximity, with many recommending that people stay at least two metres (six feet) apart in public settings. However, some governments have recommended that one metre is sufficient in fast-moving public settings. American rules could include staying home as much as possible and only going out for absolutely necessary errands (like going to work or the supermarket) during the early stages of the epidemic [61, 62].
While several nations have issued obligatory stay at home orders, it is vital to keep in mind that criteria have changed and are always being updated, depending on which nation is being considered. Guidelines for maintaining physical distance can be helpful to a person’s physical health, but they can also be harmful to their mental and social wellbeing. As it is, PWHs may already be hesitant to be in physical contact with others. This may be especially true for PWH who have just received their HIV diagnosis and may not yet know all the ways the virus might be spread. Similarly, it might be difficult for PWH, who lack access to digital communication with friends to keep such friendships alive. Some research suggests that PWHs, like the general public, are spending increasing time on social media platforms [63].
Many people who are homeless or poor are also members of marginalised groups, which has severe societal consequences. Those who are unemployed, underemployed, or furloughed as a result of COVID-19; those who are homeless or have unstable housing as a pre-existing situation or as a result of COVID-19; and those who may need to resort to food banks are at a higher risk of contracting HIV. People in rural and isolated places, whose access to the internet is spotty or weather-dependent, or whose budgets necessitate limited data plans also feel the social effects. Furthermore, COVID-19 has a disproportionately harmful impact on PWHs who were separated from spouses or family when international borders closed and who now face protracted separations from their key social supports [64]. Finally, COVID-19 has social and political consequences for PWH. Despite a generally positive political response to COVID-19 in many nations, certain responses have been controversial. Access to services and resources connected to COVID-19 has been hampered for PWHs because of confusion or delays caused by the lack of uniform public messaging in several countries. The social effects of COVID-19 on HIV therapy are obvious and varied, and their long-term effects are mostly unpredictable [65, 66].
Effect of Covid-19 on UNAIDS Targets
The Joint United Nations Programme on HIV/AIDS (UNAIDS) initiated the 90-90-90 objectives in 2014 [67, 68]. The UNAIDS “90-90-90” policy seeks for 90 percent of HIV- infected people to be diagnosed by 2020, 90 percent to be on antiretroviral medication (ART), and 90 percent to achieve sustained virologic suppression [67, 68]. However, most nations were significantly behind at that time, and the 2020 deadlines were unrealistic globally as most countries missed those [67, 68, 69].
The UNAIDS targets for 2025, which were amended in December 2020, called for 95 percent of individuals living with HIV to know their status, 95 percent of those who knew their status to be on treatment, and 95 percent of those on treatment to have viral suppression [70, 71]. The HIV targets (cascade) has increasingly been used to direct and assess programmes to improve population antiretroviral treatment (ART) coverage, a vital element of treatment prevention strategy [72]. Figure 1 illustrates further Southern African Development Community (SADC) countries and how they compared with other countries regarding the percentage of HIV infection of people living with HIV on antiretroviral therapy in 2020.
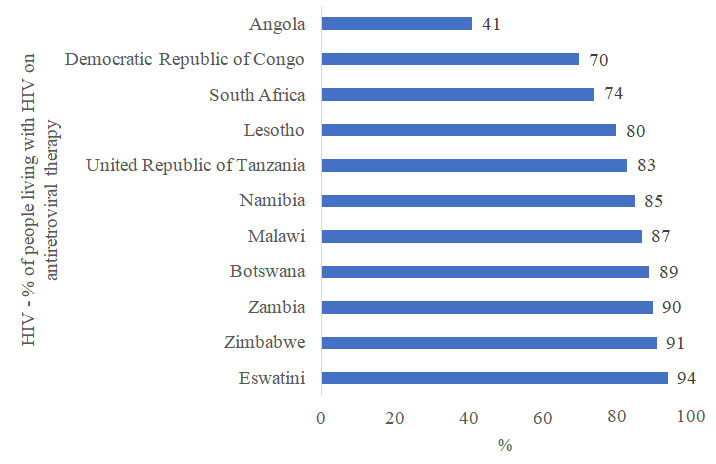
Source: The Global Fund [73]. Figure 1: HIV-percentage of people living with HIV on antiretroviral therapy: 2020.
![Figure 2: The status of selected African countries to achieve the HIV 95-95-95 cascade levels by 2025 as of September 2022 [77-79].](/fulltextimages/9651/fig_2.png)
Several studies have shown that COVID-19 has an impact on the Joint United Nations Programme on HIV/AIDS (UNAIDS) 90-90-90 objectives. For instance, researchers compared the 90–90–90 targets for people with HIV in 2020, during the COVID-19 pandemic, to the targets for the period 2017–2019 and discovered a big decrease in HIV care or access to HIV-related services in 2020, compared to 2017–2019 [74]. South Africa, which has one of the largest HIV programs and is one of the countries with the highest HIV infection rates, is transitioning to the National Strategic Plan (NSP) targets of 95/95/95 for HIV, TB, and sexually transmitted infections (STIs) [75]. Comparatively to neighbouring nations such as Lesotho and Botswana [75, 76], South Africa is projected to fall far short of its 2023–2028 ambitions. According to the World Health Organization (WHO), just nine countries are on track to fulfil the 95/95/95
targets by 2025 [76, 77]: Botswana, Cabo Verde, Kenya, Lesotho, Malawi, Nigeria, Rwanda, Uganda, and Zimbabwe (Figure 2).
HIV Related Deaths
The table below depicts the effect of HIV prevention strategies or ARVs on related deaths on select Southern African Development Community (SADC) countries. The data shows that prevention strategies results in saving of lives where the change in the numbers of deaths ranges between 33 and 84 percent; except for Angola which is still experiencing a high number of HIV related deaths. Countries such as South Africa would have seen deaths increasing by almost 800 percent if there had been no prevention strategies or ARVs administered while Eswatini which has done well in terms of HIV cascades would have seen death rising by 352 percent. The table further illustrates the significant positive effect of prevention strategies and the effect of ARVs in preventing HIV deaths.
| If no prevention or ARVs (2002-2021) | Actual change (2002-2021) | |
|---|---|---|
| Angola | 397 | 82 |
| Botswana | 192 | -75 |
| Democratic Republic of Congo | -7 | -76 |
| Eswatini | 352 | -72 |
| Lesotho | 119 | -71 |
| Malawi | 11 | -84 |
| Namibia | 204 | -72 |
| South Africa | 791 | -77 |
| United Republic of Tanzania | 172 | -75 |
| Zambia | 161 | -73 |
| Zimbabwe | 34 | -84 |
Table 1: Trends in AIDS related deaths – Select countries. Source: Adapted from The Global Fund [73] COVID-19 and HIV Vaccines.
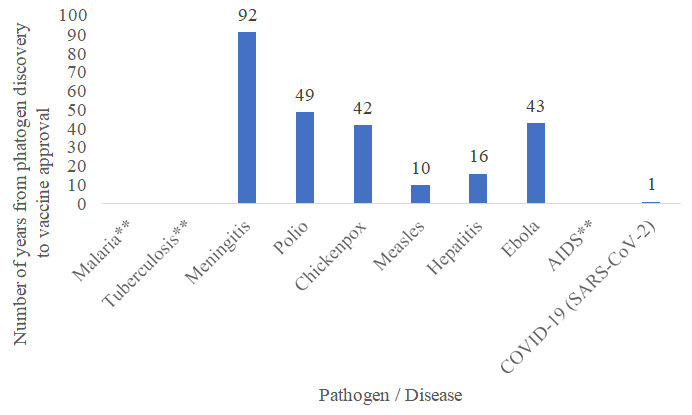
Source: Vanderslott, Dadonaite, Spooner, and Roser [80]. ** None/NA or No vaccine Figure 3: Number of years from pathogen discovery to vaccine approval.
In nearly four decades of research, scientists have not been able to develop an effective vaccine against HIV. Figure 3 illustrates vaccine innovations for ten pathogens / diseases [80]. Since the late 1980s, several potential vaccines against HIV have been produced, but none of them demonstrated effective prevention [81, 82]. In particular, one Thai study reported a 31 percent lower HIV infection rate in vaccinated individuals than in the placebo group, representing the only HIV vaccine experiment that has shown promising findings [82]. Since vaccine licensure requires an efficacy of at least 50 percent, the challenge still remain in exploring the virus’s complexity [81].
Conclusion
Healthcare delivery has had to change due to the COVID-19 epidemic. Due to their need for routine medical treatment, people living with HIV are especially vulnerable to pandemic- related interruptions in the healthcare system. There is evidence to suggest that these novelties may increase access to and utilisation of these services and hence should be preserved after the epidemic has passed. There were significant differences in the severity of the pandemic’s effects on HIV healthcare services between different groups, which might raise morbidity and death. Providers and systems of care for people living with HIV must recognise the challenges these communities experienced if they are to make policy and practice adjustments that will result in better and sustained access to care. In countries with high HIV prevalence, where there are now over 24 million COVID-19 cases and where numbers are rising quickly, preventative methods to slow the spread of this virus are crucial. Despite no apparent differences in the clinical course of COVID-19 in PLWH in the general population, elevated inflammatory states from both disorders are a cause for worry because they can lead to consequences. Any reaction to the COVID-19 pandemic must take into account the virus’s distinct modes of spread, incubation and infectiousness time, and health impacts. Lessons learnt from the HIV response, however, provide useful insight for combating COVID-19; particularly in the areas of bolstering political commitment, engaging communities, prioritising research and accountability, galvanising innovation in service delivery, mobilising sectors outside of health, and grounding responses in the principles of human rights and equality. The health effects and long- term viability of COVID-19 interventions may be maximised with the help of strategic, planned use of HIV infrastructure.
Although the majority of countries survived and thrived during the epidemic despite disruptions in the provision of health services, HIV care decreased in a number of African nations. The majority of nations are far from achieving the HIV cascade targets of 95/95/95 by 2025. Botswana, Eswatini, and Zimbabwe are spearheading these initiatives and reaching the 2025 goals, acting as models for other nations. This study also emphasized the impact of HIV preventive measures and how they have lowered mortality and saved millions of lives through initiatives such as providing treatment to patients.
References
-
Malik JA, Maqbool M (2020) COVID-19: An overview of current scenario. Cellmed 10(3): 21.1-21.8.
-
Yuki K, Fujiogi M, Koutsogiannaki S (2020) COVID-19 pathophysiology: A review. Clinical Immunology 215: 108427.
-
Yang L, Liu S, Liu J, Zhang Z, Wan X, et al. (2020) COVID-19: immunopathogenesis and Immunotherapeutics. Signal Transduction and Targeted Therapy 5(1): 128.
-
Brown LB, Spinelli MA, Gandhi M (2021) The interplay between HIV and COVID-19: summary of the data and responses to date. Current Opinion in HIV and AIDS 16(1): 63-73.
-
Jiang H, Zhou Y, Tang W (2020) Maintaining HIV care during the COVID-19 pandemic. The lancet HIV 7(1): e308-e309.
-
Ssentongo P, Heilbrunn ES, Ssentongo AE, Advani S, Chinchilli VM, et al. (2021) Epidemiology and outcomes of COVID-19 in HIV-infected individuals: a systematic review and meta-analysis. Scientific reports 11: 6283.
-
Logie CH (2020) Lessons learned from HIV can inform our approach to COVID‐19 stigma. Journal of the International AIDS Society 23(5): e25504.
-
Vizcarra P, Pérez-Elías MJ, Quereda C, Moreno A, Vivancos MJ, et al. (2020) Description of COVID-19 in HIV-infected individuals: a single-centre, prospective cohort. The lancet HIV 7: e554-e564.
-
Etienne N, Karmochkine M, Slama L, Pavie J, Batisse D, et al. (2020) HIV infection and COVID-19: risk factors for severe disease. AIDS (London, England) 34(12): 1771- 1774.
-
Nagarakanti SR, Okoh AK, Grinberg S, Bishburg E (2021) Clinical outcomes of patients with COVID‐19 and HIV coinfection. Journal of Medical Virology 93(3): 1687- 1693.
-
Mesfin Y, Argaw M, Geze S, Zewdu BT (2021) Factors associated with intention to receive COVID-19 vaccine among HIV positive patients attending ART clinic in Southwest Ethiopia. Patient preference and adherence 15: 2731-2738.
-
Desta AA, Woldearegay TW, Gebremeskel E, Alemayehu M, Getachew T, et al. (2021) Impacts of COVID-19 on essential health services in Tigray, Northern Ethiopia: A pre-post study. Plos one 16: e0256330.
-
Adugna A, Azanaw J, Melaku MS (2021) The Effect of COVID-19 on Routine HIV Care Services from Health Facilities in Northwest Ethiopia. HIV/AIDS (Auckland, NZ) 13: 1159-1168.
-
Budak JZ, Scott JD, Dhanireddy S, Wood BR (2021) The impact of COVID-19 on HIV care provided via telemedicine-past, present, and future. Current HIV/ AIDS Reports 18(2): 98-104.
-
Qiao S, Yang X, Sun S, Li X, Mi T, et al. (2021) Challenges to HIV service delivery and the impacts on patient care during COVID-19: perspective of HIV care providers in Guangxi, China. AIDS care 33(5): 559-565.
-
Hogan AB, Jewell BL, Sherrard-Smith E, Vesga JF, Watson OJ, et al. (2020) Potential impact of the COVID-19 pandemic on HIV, tuberculosis, and malaria in low- income and middle-income countries: a modelling study. The Lancet Global Health 8(9): e1132-e1141.
-
Celestin K, Allorant A, Virgin M, Marinho E, Francois K, et al. (2021) Short-term effects of the COVID-19 pandemic on HIV care utilization, service delivery, and continuity of HIV antiretroviral treatment (ART) in Haiti. AIDS and Behavior 25(5): 1366-1372.
-
Grimsrud A, Wilkinson L (2021) Acceleration of differentiated service delivery for HIV treatment in sub‐Saharan Africa during COVID‐19. Journal of the International AIDS Society 24(6): e25704.
-
Edelman EJ, Aoun-Barakat L, Villanueva M, Friedland G (2020) Confronting another pandemic: lessons from HIV can inform our COVID-19 response. AIDS and Behavior 24(7): 1977-1979.
-
Lancet T (2020) Maintaining the HIV response in a world shaped by COVID-19. Lancet 396(10264): 1703.
-
Musuka G, Dzinamarira T, Madziva R, Herrera H, El Sadr W (2022) Protecting HIV service delivery for key populations in southern Africa in the context of the COVID-19 pandemic. IJID Regions 3: 114-116.
-
Pollard R, Gopinath U, Reddy YA, Kumar BR, Mugundu P, et al. (2021) HIV service delivery in the time of COVID‐19: focus group discussions with key populations in India. Journal of the International AIDS Society 24(S6): e25800.
-
Izzo I, Carriero C, Gardini G, Fumarola B, Chiari E, et al. (2021) Impact of COVID- 19 pandemic on HIV viremia: a single-center cohort study in northern Italy. AIDS Research and Therapy 18(1): 31.
-
Jewell BL, Smith JA, Hallett TB (2020) Understanding the impact of interruptions to HIV services during the COVID-19 pandemic: a modelling study. E Clinical Medicine 26: 100483.
-
Ridgway JP, Schmitt J, Friedman E, Taylor M, Devlin S, et al. (2020) HIV care continuum and COVID-19 outcomes among people living with HIV during the COVID-19 pandemic, Chicago, IL. AIDS and Behavior 24(10): 2770- 2772.
-
Abdela SG, Berhanu AB, Ferede LM, Griensven JV (2020) Essential healthcare services in the face of COVID-19 prevention: experiences from a referral hospital in Ethiopia. The American Journal of Tropical Medicine and Hygiene 103(3): 1198-1200.
-
Keene C, Mohr-Holland E, Cassidy T, Scott V, Nelson A, et al. (2020) How COVID-19 could benefit tuberculosis and HIV services in South Africa. The Lancet Respiratory Medicine 8(9): 844-846.
-
Jewell BL, Mudimu E, Stover J, Ten Brink D, Phillips AN, et al. (2020) Potential effects of disruption to HIV programmes in sub-Saharan Africa caused by COVID-19: results from multiple mathematical models. The lancet HIV 7(9): e629-e640.
-
Nachega JB, Kapata N, Sam-Agudu NA, Decloedt EH, Katoto PD, et al. (2021) Minimizing the impact of the triple burden of COVID-19, tuberculosis and HIV on health services in sub-Saharan Africa. International Journal of Infectious Diseases 113(S1): S16-S21.
-
Lodge W, Kuchukhidze S (2020) COVID-19, HIV, and migrant workers: the double burden of the two viruses. AIDS patient care and STDs 34(6): 249-250.
-
Stover J, Kelly SL, Mudimu E, Green D, Smith T, et al. (2021) The risks and benefits of providing HIV services during the COVID-19 pandemic. Plos one 16: e0260820.
-
Patel P, Kerzner M, Reed JB, Sullivan PS, El-Sadr WM (2022) Public Health Implications of Adapting HIV Pre-exposure Prophylaxis Programs for Virtual Service Delivery in the Context of the COVID-19 Pandemic: Systematic Review. JMIR Public Health and Surveillance 8(6): e37479.
-
Dorward J, Khubone T, Gate K, Ngobese H, Sookrajh Y, et al. (2021) The impact of the COVID-19 lockdown on HIV care in 65 South African primary care clinics: an interrupted time series analysis. The Lancet HIV 8(3): e158-e165.
-
Mi T, Yang X, Sun S, Li X, Tam CC, et al. (2021) Mental health problems of HIV healthcare providers during the COVID-19 pandemic: the interactive effects of stressors and coping. AIDS and Behavior 25(1): 18-27.
-
Armstrong WS, Agwu AL, Barrette EP, Ignacio RB, Chang JJ, et al. (2021) Innovations in human immunodeficiency virus (HIV) care delivery during the coronavirus disease 2019 (COVID-19) pandemic: policies to strengthen the ending the epidemic initiative-a policy paper of the Infectious Diseases Society of America and the HIV medicine association. Clinical Infectious Diseases 72(1): 9-14.
-
Muhula S, Opanga Y, Oramisi V, Ngugi C, Ngunu C, et al. (2021) Impact of the first wave of the COVID-19 pandemic on HIV/AIDS programming in Kenya: evidence from Kibera informal settlement and COVID-19 hotspot counties. International Journal of Environmental Research and Public Health 18(11): 6009.
-
Linnemayr S, Wilson LJ, Saya U, Wagner Z, MacCarthy S, et al. (2021) HIV care experiences during the COVID-19 pandemic: mixed-methods telephone interviews with clinic-enrolled HIV-infected adults in Uganda. AIDS and Behavior 25(1): 28-39.
-
Santos GM, Ackerman B, Rao A, Wallach S, Ayala G, et al. (2021) Economic, mental health, HIV prevention and HIV treatment impacts of COVID-19 and the COVID-19 response on a global sample of cisgender gay men and other men who have sex with men. AIDS and Behavior 25(2): 311-321.
-
Gabster A, Erausquin JT, Michielsen K, Mayaud P, Pascale JM, et al. (2022) How did COVID-19 measures impact sexual behaviour and access to HIV/STI services in Panama? Results from a national cross-sectional online survey. Sexually Transmitted Infections 98(5): 332-340.
-
Pinto RM, Park S (2020) COVID-19 pandemic disrupts HIV continuum of care and prevention: implications for research and practice concerning community- based organizations and frontline providers. AIDS and Behavior 24(9): 2486-2489.
-
Jardim CGR, Zamani R, Akrami M (2022) Evaluating the Impact of the COVID-19 Pandemic on Accessing HIV Services in South Africa: A Systematic Review. International Journal of Environmental Research and Public Health 19(19): 11899.
-
Weerasuria M, Ko C, Ehm A, O’Bryan J, McMahon J, et al. (2021) The impact of the COVID-19 pandemic on people living with HIV in Victoria, Australia. AIDS Research and Human Retroviruses 37(4): 322-328.
-
Winwood JJ, Fitzgerald L, Gardiner B, Hannan K, Howard C, et al. (2021) Exploring the social impacts of the COVID-19 pandemic on people living with HIV (PLHIV): a scoping review. AIDS and Behavior 25(12): 4125-4140.
-
Millett GA (2020) New pathogen, same disparities: why COVID‐19 and HIV remain prevalent in US communities of colour and implications for ending the HIV epidemic. Journal of the International AIDS Society 23(11): e25639.
-
Coker M, Folayan MO, Michelow IC, Oladokun RE, Torbunde N, e al. (2021) Things must not fall apart: the ripple effects of the COVID-19 pandemic on children in sub-Saharan Africa. Pediatric Research 89: 1078-1086.
-
Tamuzi JL, Ayele BT, Shumba CS, Adetokunboh OO, Uwimana-Nicol J, et al. (2020) Implications of COVID-19 in high burden countries for HIV/TB: A systematic review of evidence. BMC infectious diseases 20(744): 1-18.
-
Sanchez TH, Zlotorzynska M, Rai M, Baral SD (2020) Characterizing the impact of COVID- 19 on men who have sex with men across the United States in April, 2020. AIDS and Behavior 24(7): 2024-2032.
-
Peluso MJ, Bakkour S, Busch MP, Deeks SG, Henrich TJ, (2020) A High Percentage of People with HIV on Antiretroviral Therapy Experience Detectable Low- Level Plasma HIV-1 RNA Following COVID-19. Clin Infect Dis 73(9): e2845-e2846.
-
Vasylyeva TI, Smyrnov P, Strathdee S, Friedman SR (2020) Challenges posed by COVID‐19 to people who inject drugs and lessons from other outbreaks. Journal of the International AIDS Society 23(7): e25583.
-
Peprah P, Gyasi RM (2021) Stigma and COVID‐19 crisis: A wake‐up call. The International Journal of Health Planning and Management 36(1): 215-218.
-
Mitchell KM, Dimitrov D, Silhol R, Geidelberg L, Moore M, et al. (2021) The potential effect of COVID-19-related disruptions on HIV incidence and HIV-related mortality among men who have sex with men in the USA: a modelling study. The Lancet HIV 8(4): e206-e215.
-
Enane LA, Apondi E, Aluoch J, Bakoyannis G, Lewis Kulzer J, et al. (2021) Social, economic, and health effects of the COVID-19 pandemic on adolescents retained in or recently disengaged from HIV care in Kenya. Plos one 16: e0257210.
-
Wion RK, Miller WR (2021) The Impact of COVID-19 on HIV self-management, affective symptoms, and stress in people living with HIV in the United States. AIDS and Behavior 25: 3034-344.
-
El Moussaoui M, Lambert N, Maes N, Fombellida K, Vaira D, et al. (2021) Impact of the COVID-19 pandemic situation on HIV care in Liège, Belgium. HIV Research & Clinical Practice 22: 63-70.
-
Ogunbodede OT, Zablotska-Manos I, Lewis DA (2021) Potential and demonstrated impacts of the COVID-19 pandemic on sexually transmissible infections. Current Opinion in Infectious Diseases 34: 56-61.
-
Zhou A (2021) Limits of neoliberalism: HIV, COVID-19, and the importance of healthcare systems in Malawi. Global Public Health 16: 1346-1363.
-
Schmidt-Sane M, Leach M, MacGregor H, Meeker J, Wilkinson A (2021) Local Covid-19 syndemics and the need for an integrated response.
-
Leach M, Meeker J, MacGregor H, Schmidt-Sane M, Wilkinson A (2020) COVID-19: Key considerations for a public health response.
-
Kawohl W, Nordt C (2020) COVID-19, unemployment, and suicide. The Lancet Psychiatry 7: 389-390.
-
Riley T, Sully E, Ahmed Z, Biddlecom A (2020) Estimates of the potential impact of the COVID-19 pandemic on sexual and reproductive health in low-and middle- income countries. International perspectives on sexual and reproductive health 46: 73-76.
-
Garcia PJ, Cabrera DM, Cárcamo PM, Diaz MM (2022) HIV and COVID-19 in Latin America and the Caribbean. Current HIV/AIDS Reports 19(1): 1-9.
-
Hall A, Joseph O, Devlin S, Kerman J, Schmitt J, et al. (2021) That same stigma... that same hatred and negativity: a qualitative study to understand stigma and medical mistrust experienced by people living with HIV diagnosed with COVID-19. BMC infectious diseases 21(1): 1066.
-
Alene KA, Wangdi K, Clements AC (2020) Impact of the COVID-19 pandemic on tuberculosis control: an overview. Tropical medicine and infectious disease 5: 123.
-
Becker AD, Grantz KH, Hegde ST, Bérubé S, Cummings DA, et al. (2021) Development and dissemination of infectious disease dynamic transmission models during the COVID-19 pandemic: what can we learn from other pathogens and how can we move forward?. The Lancet Digital Health 3: e41-e50.
-
Barocas JA, Savinkina A, Lodi S, Epstein RL, Bouton TC, et al. (2022) Projected Long-Term Impact of the Coronavirus Disease 2019 (COVID-19) Pandemic on Hepatitis C Outcomes in the United States: A Modeling Study. Clinical infectious diseases 75: e1112-e1119.
-
Saeed F, Mihan R, Mousavi SZ, Reniers RL, Bateni FS, et al. (2020) A narrative review of stigma related to infectious disease outbreaks: What can be learned in the face of the Covid-19 pandemic?. Frontiers in psychiatry 11: 565919.
-
UNAIDS (2020) 90-90-90 treatment target.
-
Gisslén M, Svedhem V, Lindborg L (2017) Sweden, the first country to achieve the Joint United Nations Programme on HIV/AIDS (UNAIDS)/World Health Organization (WHO) 90-90-90 continuum of HIV care targets. HIV Med 18(4): 305-307.
-
UNAIDS (2020) HIV Prevention 2025. Getting on track to end AIDS as a public health threat by 2030.
-
Samuel K (2021) Getting to 95-95-95: global use of HIV generics would result in large reductions in spending, new infections and deaths.
-
Frescura L, Godfrey-Faussett P, Feizzadeh AA, El-Sadr W, Syarif O, et al. (2022) Achieving the 95 95 95 targets for all: A pathway to ending AIDS. PLoS ONE 17(8): e0272405.
-
Refeletswe L (2021) To achieve 95-95-95 targets we must reach men and youth: High level of knowledge of HIV status, ART coverage, and viral suppression in the Botswana Combination Prevention Project through universal test and treat approach. PloS one 16: 8e0255227.
-
The Global Fund (2022) HIV: State of the Fight.
-
Guaraldi G, Borghi V, Milic J, Carli F, Cuomo G, et al. (2021) The impact of COVID-19 on UNAIDS 90-90-90 targets: calls for new HIV care models. Open Forum Infect Dis 8(7): ofab283.
-
South African Government. Minister Joe Phaahla: SA satellite on 90-90-90 progress and recovery from Covid-19.
-
World Health Organization (2021) Africa cuts HIV infections, deaths but key targets still elusive.
-
U.S. Department of State (2022) Eswatini surpasses UNAIDS fast-track targets for treatment andviral suppression.
-
Joint United Nations Programme on HIV/AIDS. Fact sheet 2022.
-
Willie MM, Kabane S (2022) Impact of COVID-19 on HIV Care in Africa. World Medical Journal 3(70): 10-14.
-
Vanderslott S, Dadonaite B, Spooner F, Roser M (2013) Vaccination.
-
Dutton J (2022) Can mRNA technology help scientists produce a viable HIV vaccine?.
-
Vaccari M, Poonam P, Franchini G (2010) Phase III HIV vaccine trial in Thailand: a step toward a protective vaccine for HIV. Expert Rev Vaccines 9(9): 997-1005.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda