Bacterial Settlement and Bacteriological Contamination of Mobile Devices
Objective. Determine the relationship between knowledge about bacterial settlement and bacteriological contamination of mobile devices of the Emergency Service. Method: Documentary, Survey technique . Instruments a questionnaire of bacterial settlement and a technical sheet of bascteriological contamination. Hllazgos. 87.5%(28) of mobile devices had positive biochemical analysis (+) (Escherichia Coli 21.9%(7), Staphylococcus Epidermidis 18.8%(6) and Klebsiella Pneumoniae 9.4%(3) cover the highest percentages) for the presence of some type of bacteria, of which 56.3%(18) of nurses who own mobile devices have knowledge of deficient bacterial settlement. (p calculated = 0.013 < constant p of 0.05). Conclusion. The results show a large percentage of nursing professionals who underestimate the impact of bacterial settlement that their mobile devices house, and that many of these bacterial agents are potentially harmful to the professional, the user and the family, and can trigger chronic degenerative diseases.
Introduction
The performance of nursing work in critical services such as the emergency service denotes a scenario of tension, stress, and an arduous commitment in the timely execution of invasive procedures and in the vast majority of cases, these procedures of direct or indirect contact with users are consistent, in that sense the frequency of the use of biosafety standards goes unnoticed optimally for specific situations, that is, in some way, nursing professionals make use of their mobile devices for communication with plant staff, family, friends, etc. This means being the potential transmitter of a number of bacteria that begin to adhere to contact with the hands of the nursing professional, but when analyzing this situation on the one hand, there may be host bacteria in mobile devices brought from contexts outside the hospital, on the other hand, the environment can be a host of bacteria from direct contact with users or some body fluids, including from the same infrastructure of the hospital context.
This situation in the end triggers the potential damage that we could bring to the user and to the health professionals themselves, who in compliance with their timely work in many cases do not perform a continuous asepsis of the hands being susceptible to being potential carriers of different types of bacteria from the easiest to eradicate to the most resistant bacterial communities causing various chronic diseases.
The fact is that not only is there a risk of infection of the user-nurse binomial, but that the relatives of the user and the nursing professional, each of them are potentially susceptible when they come into contact on their return home.
While it is true that there is a great risk of using cellular devices in these critical services, and sometimes it is suggested not to use them or use them as little as possible and with optimal biosecurity measures. (Applying techniques such as hand washing, glove shoes, etc.); However, even only for the attention of the user the practice of hand washing is infrequent and less before using cell phones.
In the study of Mendoza K, et al. [1], it shows that 61% of nurses perform correct hand washing practice, while 39% present an incorrect hand washing practice [1]. These results show the inadequate practice of key procedures that could help prevent the spread of bacteria by direct contact with communication devices.
Also in the analysis of Chincha O, et al. [2] explains that, in a study in Peru, in 2000 conducted in 70 hospitals with more than 1500 discharges per year with projection for the next decade, a prevalence of 3.7% of hospital-acquired infections was evidenced, with the most affected areas being the ICU and neonatology. In addition, another study conducted in a level four Social Security hospital presented a prevalence of 7.5%, being mostly patients of intermediate care and critical services such as the emergency service [2].
As can be seen in the results of the studies measuring bacteriological contamination is evaluated by the number of hospital-acquired infections originating in the hospital context, cave rescue that the incidence and prevalence of these rates are increasing due to various factors; However, there are few studies that address the origin of hospital- acquired infections and their genesis approach that determine how important it is to know the type of bacteria that the host contracts when repeatedly contacted by their mobile devices inside critical hospital spaces considered highly contaminated by the frequency of multiple cases of users with various diagnostic pathologies.
This reality is not alien to the emergency service of Félix Mayorca Soto in times of Pandemic, Tarma, scenario where simulation studies have not been addressed without however, direct observation shows a population of nursing professionals in constant use of mobile devices within critical services before and after contact with users and with infrastructure of the emergency service context, The study aims to analyze what types of bacteria are being hosted on your mobile devices and are vastly underestimated in the face of the potential damage they can trigger on your health.
Theoretical Foundations
Background of study
Buelvas PE, et al. [3] entitled “Microbial characterization of mobile phones belonging to students of Dentistry of the University of Cartagena”, shows that, of 90 samples taken, microbial growth was observed in 69, of which 54 were Gram positive and 11 Gram negative. The microorganisms with the highest growth were Staphylococcus sp. There was also evidence of growth of Candida albicans, Escherichia coli and Pseudomona aeruginosa. 100% of participants said they transport their phone to the clinic, 96% interrupt patient care, 77.8% handle it with gloves on, 85.5% do not wash their hands at the end of care and 93.3% do not perform any type of mobile disinfection [3].
Cedeño A [4] in its study entitled “Identification of the bacterial flora present in the telephone mobiles of personnel working in the area of microbiology and the relationship with the report of their results”, shows that the reports of results of the Microbiology area are not affected by contamination due to telephone mobiles because it was found in the 74 reports, Streptococcus pneumoniae corresponding to 25.7%, Staphylococcus aureus by 10.8%, Escherichia coli by 24.3%, Klebsiella sp by 18.9%, Citrobacter by un.4%, P. mirabillis by 2.7%, Neisseria catarrhalis by 8.1%, Klebsiella pneumoniae by 8.1%. The bacteria that were identified in the telephone mobiles were enterobacteriaceae and fecal coliforms, considered as contaminants due to poor hygiene after occupying the bathroom [4].
Cobos LD, et al. [5] in his study entitled “Bacterial contamination and antibiotic resistance in the cell phones of the medical staff of the “Vicente Corral Moscoso” hospital, shows that 93.84% of cell phones were found contaminated, of these, the telephones of the treating physicians showed an intense level of contamination, mainly by Staphylococcus aureus, Staphylococcus epidermidis, Enterobacter aerogenes. Male staff show intense contamination by Enterobacter aerogenes. The resistance to Oxacillin in Staphylococci aureus is 40.7%. In the isolated Enterobacteriaceae, a high degree of resistance to third-generation cephalosporins was found, suggesting the presence of ESBL strains [5].
Martínez EN, et al. [6] in his study entitled “Bacterial load before and after disinfection of mobile phones with 70% isopropyl alcohol”, shows that the bacterial prevalence of Staphylococcus spp. was 17.4% while for Enterobacteriaceae it was 14.4%. An average pre-disinfection bacterial load of 66.77 SE (±142) colony-forming units was found. While after disinfection was 39.75 SE (±110) [6].
Escobedo MJ, et al. [7] in its study entitled “Pathogenic bacteria isolated from cell phones of the staff and students of the Multidisciplinary Clinic (CLIMUZAC) of the Academic Unit of Dentistry of the UAZ”, shows that 63% of respondents do not clean the phone. Use in the clinical work area is 81%. The bacteria identified were: Staphylococcus sp. 16.7%, Staphylococcus aureus 38.7%, Klebsiella sp. 11.6%, Klebsiella pneumoniae 0.6%, Shigella sp. 10.3%, Streptococcus sp.
8.3%, Streptococcus pneumoniae 1.2%, Micrococcus sp. 0.6%, Pseudomonas sp. 1.9%, Pseudomonas aeruginosa 0.6%, Enterococcus sp. 0.6%, Enterococcus faecalis 3.2%, Salmonella sp. 1.9%, Bacteroides vulgaris 0.6%, Escherichia coli 1.9% [7].
Vázquez CM, et al. [8] its study entitled “Frequency of contamination of cell phones and stethoscopes of personnel working in the Emergency Department”, shows that 14.8% of respondents did not clean the devices and 91.4% said they did not have relevant information. We found no association between the variables and the development of pollution [8].
Orlando O [9] in his study entitled “Contaminating bacteria isolated from cell phones of Medical Interns and Resident Physicians and susceptibility to antibiotics”, shows that 95.35% of cases showed bacterial growth, found Staphylococcus aureus Metcilina – Sensitive: 22.66%, Staphylococcus aureus Methcilin – Resistant: 28.13%, Staphylococcus aureus Vancomycin – Resistant: 0.78%, Staphylococcus aureus Coagulase – Negative: 37.5%, Streptococcus spp: 26.56%, Enterobacteria: 20.31% and Pseudomonas aeruginosa: 7.81% [9].
Espinoza A [10] in his study entitled “Contamination of pathogenic bacteria in cell phones of health personnel of the Daniel Alcides Carrión Hospital - Huancayo”, quantitative research, as a data collection technique, the culture of surface swabs was carried out, the study sample was made up of 86 cell phones, reaching the representative conclusion that: 84.88% of the phones are contaminated with pathogenic bacteria and opportunistic pathogenic bacteria, of these doctors and interns, technicians showed an intense level of contamination, 57.39% corresponds to bacteria of the genus Staphylococcus and Streptococcus, 42.61% corresponds to Enterobacteria [10].
Miranda H, et al. [11] in his study entitled “Cell phones as a source of contamination of pathogenic bacteria in the health personnel of the Hospital de los Valles, Cumbayá, Ecuador in November 2014”, shows that to demonstrate that the bacteria that developed in cell phones are the cause of nosocomial infections, it is necessary to do a phylogenetic and cytogenetic study. In this work, St aureus and E coli are within the group of microorganisms with the highest percentage of occurrence (in more than 90% of study objects) both in the culture of mobile devices and in the group of bacteria causing nosocomial infections [11].
Oliva J, et al. [12] in his study entitled “Contamination with pathogenic bacteria of stethoscopes of medical personnel in a level III hospital in Lima, Peru”, observational research, shows that: of the 124 stethoscopes studied; 114 (91.9%) were contaminated; 123 bacterial strains were isolated:
coagulase-negative Staphylococcus spp 106 (86.1%), Staphylococcus aureus 5 (4.0%), Enterobacter aerogenes 4 (3.2%), Acinetobacter spp 2 (1.6%), Pseudomonas aeruginosa 4 (3.2%), Klebsiella pneumoniae 1 (0.8%) and Escherichia coli 1 (0.8%) [12].
Problem Formulation and Objectives
It was Presented as a General Problem: What is the relationship between the knowledge about bacterial settlement and bacteriological contamination of mobile devices of the Emergency Service of the Félix Mayorca Soto Hospital in times of Pandemic, Tarma – 2021?
The general objective of the research was to determine the relationship between knowledge about bacterial settlement and bacteriological contamination of mobile devices of the Emergency Service of the Félix Mayorca Soto Hospital in times of Pandemic, Tarma – 2021.
Theoretical Framework
Theoretical Basis, Bacterial Settlement: Pirez M, et al. [13] report that “bacteria are unicellular microorganisms that reproduce by binary fission. Most are free-living, except for some that are obligatory intracellular life, such as Chlamydias and Rickettsias. They have the energy-producing mechanisms and genetic material necessary for their development and growth”[13]. We can appreciate then that bacteria as a whole are prokaryotic unicellular beings, being the large groups involved eubacteria and archeobacteria. The latter being bacteria that lack peptidoglycan wall. They generally live in the depths of the sea, in salty waters and in acidic sources. On the other hand, eubacteria live on external surfaces such as soil, in water and in living organisms; this group of bacteria is the most studied by medical expertise.
Structure of Bacteria
On the bacterial structure Catalina M (2002), describes the structure of bacteria as a set of components that will allow the bacterial cell to fulfill its internal physiological processes of survival in that sense the bacterial structure is governed by permanent and variable structural components: [14]
- Permanent structures: Cell membrane, Ribosomes, Genetic material.
- Variable structures: Cell wall - Flagellum - Fimbria or pilis - Capsule - Spores. [15]
- Permanent structures: They are strictly present in all bacterial structures.
- Cell membrane: It corresponds to a thin structure that surrounds the cell 8nm thick, being of special vitality for the cell. It is composed of a double phospholipid layer, unlike the eukaryotic cell it does not have sterols. (except mycoplasmas), as the main function delimits the interior of the cell exterior, so mimo is a membrane with selective permeability.
- Ribosomes: Cellular structures where proteins are synthesized, found in the bacterial cytoplasm, are composed of a large subunit (50S) and a small subunit (30S), which together form the ribosome (70S).
- Genetic Material: Composed of DNA and specific RNA, in addition many cells have in addition to extra- chromosomal DNA, also circular and closed, which is called plasmid DNA, because it is contained in plasmids, being the genetic composition of nucleic acids the same for each bacterial cell.
- Variable structures: They are present in some bacteria, not all, these structures are not necessary for the survival of the bacterial cell.
- Cell Wall: It forms a rigid structure that is located outside the cytoplasmic membrane, if it is destroyed or prevents its formation, the cell loses its viability. Peptidoglycan is its main constituent formed by: two carbohydrate derivatives, N-acetyl Glucosamine and N-acetyl Muramic (N-Ac.G, NAc.M), linked by beta 1-4 bonds and associated with short peptide chains through N-acetyl Muramic. On the cell wall of bacteria we find two sub groups according to the amount of peptidoglycan that we find in their layers as reported by Mora X [16] “its differentiation and identification is very important for the pharmaceutical approach and therapeutic management of the user who houses one of these types of bacteria in relation to its type of cell wall “ [16].
- Wall of Gram Negative bacteria: Its outer membrane exerts a notable influence on resistance to several antibiotics, especially the active ingredient of many antibiotics that reflect their active ingredient directly in the peptidoglycan wall, this being the weak point of Gram + bacteria.
- Wall of Gram Positive Bacteria: Generally more susceptible to the active ingredient of antibiotics because they have a layer of peptidoglycan of greater volume, this layer being the central axis for compliance with the active ingredient of antibiotics [17].
- Flagellum: Mobile whip-shaped appendage present in many unicellular organisms and in some multicellular cells, providing mobile capacity and adhesion for those who possess it.
- Fimbria or pilis: They are protein filamentous structures very similar to flagella, they are related to the ability of bacteria to adhere to inert or living surfaces. They play a major role in the process of bacterial colonization.
- Capsule: Envelope located outside the cell wall, forming a gel that attaches to the cell. They can be produced by both Gram Positive and Negative bacteria. It greatly influences the virulence capacity of the cell.
• Spores: Some bacteria produce it as spores or endospores. They are quite resistant to heat, desiccation, radiation, acids and chemical disinfectants. These structures are impervious to dyes and are observed as unstained regions.
Morphology of Bacteria
Vargas T, et al. [18] describe the morphology of bacteria at the base to the following classification, which based on the rigidity of the cell wall the most important of them are: [18] Cocci: Bacteria that are nearly spherical in homogeneous clusters. Its size ranges from 0.8 to 1.0 and can present and take various forms, product of its tendency to stay together, within this type of bacteria we can find: Diplococci: After their division they remain in pairs. Example the Neisseria. (Meningococcus) Tetrades: They tend to divide in perpendicular directions forming square groupings. Sarcinas: Their division ends in three perpendicular directions, usually forming a cubic arrangement. Streptococci: Divided into a single plane, forming sequences quite similar to a chain. Staphylococci: Irregular grouping of four or more coconuts, resembling bunches of grapes. Irregular shapes: They have lanceolate shapes, flattened coffee bean shape (Cocobacilli). Bacilli: Bacteria that form heterogeneous structures by presenting a variety of morphological subtypes can be cylindrical, rod, long and thin, small and thick, may also present variations in their ends being straight, sharp or rounded. In this regard, based on the groups that make up we can find: Diplobacilos: Bacilli grouped in pairs. Streptobacilli: Grouping of four or more bacilli. Palisade: Bacilli grouped in straight lines like phosphorus chopsticks. Filamentous forms: Bacilli shaped like fibers of irregular bonding. Spiriles: Group of bacteria that in their form present from one to different curves, some evidence helix shape. Vibrions: Rather short, comma-shaped spyrils. Spyrils: Helical bacteria, moving through flagella with movements around their own axis. Spirochetes: They have a helical shape, have a flexible body, their movement is by means of axial filaments that respond to periplasmic flagella. Other Forms: Star-shaped bacteria known as genus Stella may occur, we also find rectangular and flat bacteria of the genus Haloarcula, others pear-shaped belonging to the genus Hyphomicrobium and finally bacteria that form non-cellular peduncles [19].
Importance of Bacteria
On its importance, Molina J, et al. [20], mention that “members belonging to the domains Bacteria and Archaea are the most abundant forms on the planet. Bacteria constitute a significant proportion in terms of the body weight of the different hosts (from 0.5 k to about 2.5 k). Its total biomass was estimated at 3.5 × 1014 kg of carbon. However, in 2008 only ~7,000 microbial species were accepted, versus 300,000 plant species and 1,250,000 animal species, which does not reflect the total biodiversity of bacteria” [20].
In this sense, bacteriology emerges as a discipline of microbiology, to address the potential damage of countless bacteria to people’s health and why not say it of every living being. Being responsible for millions of deaths worldwide many times by bacteria identified but that cause severe potential damage when not treated in a timely manner, other types of bacteria still being studied that cause systemic damage that degenerates the homeostasis of the organism causing its early or late death.
By way of reflection we can cite some bacterial infectious diseases that cause major epidemics over time are diphtheria, cholera, tuberculosis, syphilis, tetanus, whooping cough, and typhoid fever.
Likewise there is a smaller number of associated bacteria in less frequency as a cause of death, they are today in boom problem for underdeveloped countries called undervalued bacteria in emerging populations.
On the other hand, Gonzales R, et al. [21], mention the importance to take into consideration the participation of bacteria in the human microbiota, referring to the fact that “In a healthy person, microbial cells outnumber the cells of the body by a ratio of ten to one (10:1). In the intestine alone there are approximately 1×1012 microbes that form a consortium that is closely related to the human organism: it interacts with it through different mechanisms and influences its development, physiology, immunity and nutrition. This consortium is composed mainly of bacteria and, to a lesser extent, fungi, archaea and viruses” [21].
Cave rescues in this fragment the importance of the scientific community to determine this abundant community of microorganisms that initially developed in laboratories, being the strategy for its detection the development of specific culture media that could contribute to its construction and respective classification.
However, even in the present century, they have not been able to generate all the culture media for identification, which is why to date the field of study of microorganisms called Metagenomics arises more specifically, according to Rodríguez L [22], “covers the study of gnomic DNA obtained from uncultivated microorganisms” [22].
Fact that summarizes that for our century the world does not live the age of man but the age of bacteria and their constant resistance, mutation and degree of pathogenicity to the human being.
In this sense, the bacterial intestinal flora fulfills a number of participations within the host, involving biochemical reactions of various kinds such as changes in the intestinal epithelium, immune modulation, intestinal movement and the metabolism of some drugs, being also involved in the metabolism of nutrients, degradation of toxins and carcinogens, fermentation of food, absorption of lectrolites and minerals; Finally and most importantly this human microbiome prevents the colonization and pollution of pathogenic bacteria such as: Escherichia Coli, Salmodella, Clostridiem, Shigella, among others that are being studied more specifically in view of the degenerative process they develop in the host and its potential damage to the organism, these can be captured in any context hence the importance of implementing measures of self-protection and protection towards others in Given that the degree of pathogenicity of these bacteria does not respect the lines of horizontality or verticality.
Laboratory Techniques to Determine the Type of Bacteria
Differential Gram Stain: Santambrosio E, et al. [23] describes this stain based on the one called by the Danish bacteriologist Christian Gram, who developed it in 1844. Based on their reaction to Gram staining, bacteria can be divided into two groups, gram-positive and gram-negative (in this case, the terms positive and negative have nothing to do with electric charge, but simply designate two distinct morphological groups of bacteria). Briefly described, the sequence of staining is as follows: the heat-fixed smear is stained 1 min with Crystal Violet, washed with water, covered with iodized solution for 1 - 2 min. and washed again with water, discolored with ethyl alcohol/acetone mixture. Drain and cover with Safranin (contrast color) for 1 – 2 min. Wash and dry.
Gram-positive and gram-negative bacteria stain differently due to constitutive differences in the structure of their cell walls. The wall of the bacterial cell serves to give the organism its size and shape, as well as to prevent osmotic lysis. The bacterial cell wall material that confers rigidity is peptidoglycan. The gram-positive cell wall is thick and consists of several interconnected layers of peptidoglycan as well as some teichoic acid. Generally, 80%-90% of the gram-positive cell wall is peptidoglycan. The gram-negative cell wall, on the other hand, contains a much thinner layer of peptidoglycan only and is surrounded by an outer membrane composed of phospholipids, lipopolysaccharides, and lipoproteins. Only 10% - 20% of the gram-negative cell wall is peptidoglycan [23, 24].
Bacteriological Analysis of Surfaces Using the Swab Method
Minsa [25] mentions that the objective of this practice is to check the hygienic state of the workplace or reveal the presence of microorganisms on some type of surface of any kind.
There are several methods to carry out this type of analysis, and here we are going to perform the swab method, which is appropriate for any type of surface, whether flat or not. This method is the oldest of those used in the microbiological analysis of surfaces, especially of devices and utensils. It is especially recommended to study very contaminated surfaces, since it allows decimal dilutions of the sample. The procedure to follow is as follows: Delimit the surface to be analyzed by means of a sterile aluminum foil template, with an opening of known dimensions (for example, 9cm2). Wet the sterile swab in a tube of saline solution with 4.5 ml sterile and scrub several times on the delimited surface of the template. Put the swab back into the saline tube and leave the swab inside the tube for 15-30 minutes so that the microorganisms are released from the cotton ball into the liquid. Seed 0.1 ml of the liquid into a plate with TSA media. Incubate the plate at 37ºC for 24-48 h and perform the count, expressing it as CFU per unit area. If what you want is to know the different types of microorganisms present on a certain surface (for example, skin or human mucous membranes) it will be enough to take the sterile swab without moistening and touch in the study area. Next, a TSA plate is seeded making stretch marks with the swab directly on the surface of the agar and will be incubated at 37ºC for 24-48 hours [25].
Bacteriological Contamination of Mobile Devices
The article Elika [26] refers that “bacterial pollution or contamination is the presence of bacteria on a given surface. (Salmonella, Listeria, Escherichia coli, etc.)” [26].
Now, this contamination can exert potential direct damage to its host agent, being marker the type of bacteria that has been carried by direct contact with contaminated surfaces, is the case of cell phones, which because they are an indispensable tool for communication in many cases are used without having performed the due asepsis within critical services, being a potential risk factor for both health professionals, users and family members.
As analyzed in the study background it is these devices that harbor a number of mostly manageable bacteria; However, it is not ruled out to come into contact with a type of bacteria resistant and highly harmful to health.
Main Pathogenic Bacteria at the Integumentary and Other Respiratory Levels
In the graph we observe the main bacteria that cause disease from the most controllable to the triggers of chronic diseases [27].
Bacteriological Contamination and Antimicrobial Resistance
PAHO [28], in its monthly analysis cites the importance of the impact of bacteria and other parasites to generate resistance over time against antibiotics, in that sense it is necessary to rescue how human beings contribute to it, the key axis is self-medication and vulnerability in the management of transitability of pathogenic bacteria from receptor agents (The same people, cell phones, keys, etc.) that harbor these pathogenic microorganisms which by direct contact find a host, this may or may not develop the disease depending on various factors. (Age, health status, etc.) [28]; However, these bacteria are transmitted to vulnerable groups who develop the disease and in most cases receive incomplete treatment or self-medicate corroborating the problem that falls on a group of bacteria that currently the active ingredient of antibiotics can not fight.
Base Conceptual
Dorothand Johnson “Behavioral Systems Model” Johnson D cited by CisnerosF [29] in one of the essences of his theory mentions that [29] “The individual tries to maintain a balanced system, but environmental interaction can cause instability and health problems.” That is, the nurse must be the strength of the user to maintain the balance of their health, foreseeing the control of external factors that may cause disease (adequate scenarios free of contaminants), this through the organization of appropriate behaviors of the same professional as those of the user, this axis being the primary to put into practice to avoid potential damage by direct contact with bacteria from the device to the health professional and the latter. to the user and vice versa.
Materials and Methods
The Type of Study
It was correlaconal, prospective of transversal type, whose design was descriptive correctional responds to the following scheme:
Where: M: Sample O1: Knowledge about bacterial settlement. O2: Bacteriological contamination of mobile devices. r: Relationship between variables Sample Hernandez R [30] the sample is a representative part of the population, after a simple sampling for finite population with a confidence level of 95%. A sample of 32 nursing professionals from the Emergency Department of the Félix
Results
Mayorca Soto Hospital was obtained [30].
Technique and Instruments
The technique used was the survey and the documentary. A questionnaire on knowledge about bacterial settlement and a technical sheet of laboratory analysis results.
The validity of the instrument was by means of the coefficient of the Binomial Test of 0.02 less than 0.05. Regarding the reliability analysis, the questionnaire reached a cronbach’s alpha of 0.921 (Excellent reliability). Kendall’s Tau B Statistical Test was used to test the hypothesis. A reliability of 95.0% was used for statistical significance. SPSS version 27.0 was used throughout the data processing (Tables 1 & 2; Figues 1 & 2).
| Level of Knowledge about bacterial settlement | Positive Biochemical Analysis (+) | Positive Biochemical Analysis (-) | TOTAL | |||
|---|---|---|---|---|---|---|
| f | % | f | % | f | % | |
| Very efficient | 0 | 0.00% | 4 | 12.50% | 4 | 12.50% |
| Deficient | 18 | 56.30% | 0 | 0.00% | 18 | 56.30% |
| Very deficient | 10 | 31.30% | 0 | 0.00% | 10 | 31.30% |
| TOTAL | 28 | 87.50% | 4 | 12.50% | 32 | 100.00% |
Table 1: ** Knowledge about bacterial settlement and bacteriological contamination of mobile devices of the nursing professionals
Source: Knowledge questionnaire on bacterial colonization – Technical sheet applied to nurses of the Emergency Service of the Félix Mayorca Soto Hospital, Tarma – 2022. Table 1: Knowledge about bacterial settlement and bacteriological contamination of mobile devices of the nursing professionals of the Emergency Service of the Félix Mayorca Soto Hospital, Tarma – 2022.
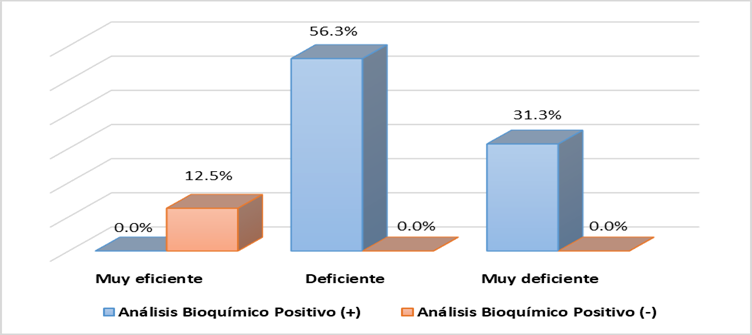
Of the 100% (32) of nursing professionals and their mobile devices under study, 87.5%(28) of mobile devices had positive biochemical analysis (+) for the presence of some type of bacteria, of which 56.3% (18) of nurses who own mobile devices had knowledge of deficient bacterial settlement and 31.3% (10) very deficient. 12.5% (4) of mobile devices had negative biochemical analysis (-) for the presence of some type of bacteria and nurses who own mobile devices had knowledge of very efficient bacterial settlement. In addition, we can statistically conclude that after applying Kendall’s Tau b test, a p value of 0.013 ≤ 0.05 was obtained, which indicates that there is a relationship between the variables under study.
| f | % | |
|---|---|---|
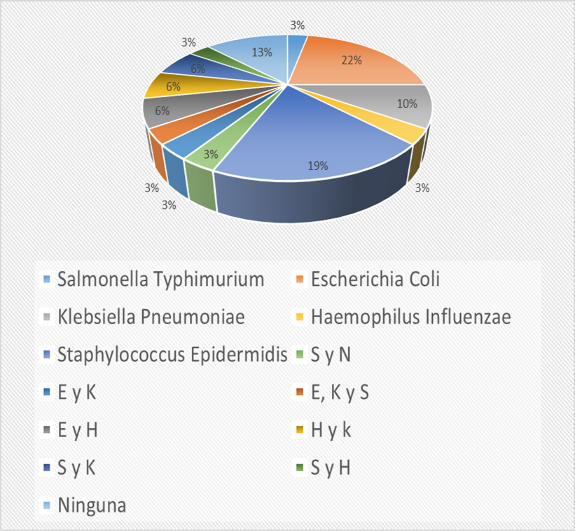
| Salmonella Typhimurium - Neisseria gonorrhoeae | 1 | 3.10% |
| Escherichia Coli | 7 | 21.90% |
| Klebsiella Pneumoniae | 3 | 9.40% |
| Haemophilus Influenzae | 1 | 3.10% |
| Staphylococcus Epidermidis | 6 | 18.80% |
| Sy N | 1 | 3.10% |
| E and K | 1 | 3.10% |
| E, K and S | 1 | 3.10% |
| E y H | 2 | 6.30% |
| H y k | 2 | 6.30% |
| Sy K | 2 | 6.30% |
| Sy H | 1 | 3.10% |
| No | 4 | 12.50% |
| TOTAL | 32 | 100.00% |
Table 2: Bacteria isolated from mobile devices of nursing professionals of the Emergency Service of the Félix Mayorca Soto Hospit
Discussion
The multidisciplinary team and specifically the nursing professionals are responsible for the care of their own health and that of the users, in this aspect it is important to analyze how the professionals underestimate the bacterial pollution present in critical services such as the emergency service for housing in their scenarios users considered potentially contaminated, Likewise, the free use of communication devices such as mobile devices are hosts of a number of bacterial pathogens harmful to health, hence the importance of addressing the issue for its identification and taking strategies against the case. Therefore, the general objective of the study responds to determine the relationship between knowledge about bacterial settlement and bacteriological contamination of mobile devices of the Emergency Service of the Félix Mayorca Soto Hospital in times of Pandemic, Tarma -2022.
The results showed that 87.5% (28) of mobile devices had positive biochemical analysis (+) for the presence of some type of bacteria, of which 56.3% (18) of nurses who own mobile devices had knowledge of deficient bacterial settlement.
As shown in the results, nursing professionals are not aware of bacterial settlement; However, the professionals who obtained an acceptable average in the evaluation, also underestimate the damage to health that can trigger the use of mobile devices in critical services and even more so when it is not practiced as specific biosecurity should be to control cross-infections.
This is also demonstrated by the study of Magdaleno C, et al. [8] that in its results shows that 14.8% of respondents did not clean the appliances and 91.4% said they did not have relevant information.
On the other hand, in the study of Delgado L [9] analyzes in his results that 93.84% of cell phones were found contaminated, of these, the telephones of the treating physicians showed an intense level of contamination, mainly by Staphylococcus aureus, Staphylococcus epidermidis, Enterobacter aerogenes.
These results with those of the study show that the multidisciplinary team and in them the nursing professionals underestimate the damage of bacteria to their own health and that of the users, by not analyzing the appropriate and in the best of cases restricted use of mobile devices, given that the results show that a good percentage of nursing professionals know about bacterial contamination; However, laboratory results include bacterial pathogens potentially harmful to your health.
On the other hand, in the specific results during the measurement of the variables under study, we find in their results that 56.3% (18) of nurses present a level of knowledge about deficient bacterial settlement and 31.3% (10) very deficient.
28.1% (9) of nurses have a general level of knowledge about deficient bacterial settlement and 56.3% (18) very deficient.
Likewise, 65.6% (21) of nurses present a level of recognition of clinical cases of deficient bacterial settlement and 21.9% (7) very deficient.
Finally, 87.5% (28) of mobile devices had positive biochemical analysis (+) (Escherichia Coli 21.9% (7), Staphylococcus Epidermidis 18.8% (6) and Klebsiella Pneumoniae 9.4%(3) cover the highest percentages) and 12.5% (4) of mobile devices had positive biochemical analysis (-).
These results are not alien to the problems studied nationally and internationally, for example in the Muñoz J, et al. [7] analyzes in its results that 63% of respondents do not clean mobile devices. Use in the clinical work area is 81%. The bacteria identified were: Staphylococcus sp. 16.7%, Staphylococcus aureus 38.7%, Klebsiella sp. 11.6%, Klebsiella pneumoniae 0.6%, Shigella sp. 10.3%, Streptococcus sp. 8.3%, Streptococcus pneumoniae 1.2%, Micrococcus sp. 0.6%, Pseudomonas sp. 1.9%, Pseudomonas aeruginosa 0.6%, Enterococcus sp. 0.6%, Enterococcus faecalis 3.2%, Salmonella sp. 1.9%, Bacteroides vulgaris 0.6%, Escherichia coli 1.9%.
As we can converge with the results of the study, many of the bacteria identified are potentially harmful to the health not only of nursing professionals but also puts the entire multidisciplinary team at risk and even more, puts family members at potential risk given that health professionals return to their daily life contexts and carry with them the bacteria hosted on their mobile devices. can trigger cross- infections at the in-hospital and out-of-hospital levels, which gives impact to the issue to be addressed in an emergent way, even more so in these times of COVID-19 pandemic.
Conclusions
In summary, we can point out that 56.3% (18) of nurses have a level of knowledge about poor bacterial settlement and 31.3% (10) are very deficient.
It is important to reflect that28.1% (9) of nurses have a general level of knowledge about deficient bacterial settlement and 56.3% (18) very deficient.
Thus, 65.6% (21) of nurses also present a level of recognition of clinical cases of deficient Bactrian settlement and 21.9% (7) very deficient.
It is alarming to find that 87.5% (28) of mobile devices had positive biochemical analysis (+) (Escherichia Coli 21.9% (7), Staphylococcus Epidermis’s 18.8% (6) and Klebsiella Pneumoniae 9.4% (3) cover the highest percentages) and 12.5% (4) of mobile devices had positive biochemical analysis (-).
It should be noted that87.5% (28) of mobile devices had positive biochemical analysis (+) for the presence of some type of bacteria, of which 56.3% (18) of nurses who own mobile devices had knowledge of deficient bacterial settlement.
In addition, the study reveals that 45.3% (24) of itinerant providers present economic factors that hinder undergoing the unfavorable state of emergency due to COVID-19 and high risk of Coronavirus infection, a fact that demonstrates that the economic need with which itinerant providers take prevails the care they must have in front of their health in these times of pandemic.
References
-
Mendoza Meregildo K, Sandoval Casana R (2016) Level of knowledge and practice of hand washing in nurses, of the Regional Institute of Neoplastic Diseases of the North 2016.
-
Chincha O, Comelio E, Valverde V, Acevedo M (2013) Hospital-acquired infections associated with invasive devices in intensive care units.
-
Buelvas Polo E, Crmona Lorduy M (2018) Microbial characterization of mobile phones belonging to students of Dentistry of the University of Cartagena.
-
Cedeño Moreira A (2017) Identification of the bacterial flora present in the telephone mobiles of the personnel working in the area of microbiology and the relationship with the report of their results.
-
Cobos LD, Brito JG, Garate MH (2016) Bacterial contamination and antibiotic resistance in the cell phones of the medical staff of the hospital “Vicente Corral Moscoso”.
-
Martínez EN, Fuentes JM, Florentino GM (2013) Bacterial load before and after disinfection of mobile phones with 70% isopropyl alcohol.
-
Escobedo JM, Castillo VL, Romero PC (2021) Pathogenic bacteria isolated from cell phones of staff and students of the Multidisciplinary Clinic (CLIMUZAC) of the Academic Unit of Dentistry of the UAZ.
-
Vázquez CM, Castellanos JL, Mendez NH (2011) Frequency of contamination of cell phones and stethoscopes of personnel working in the Emergency Service.
-
Delgado O (2021) Contaminating bacteria isolated from cell phones of Medical Interns and Resident Physicians and susceptibility to antibiotics.
-
Mallama AE (2017) Contamination of pathogenic bacteria in cell phones of health personnel of the Daniel Alcides Carrión Hospital - Huancayo.
-
Maldonado HM, Morales DP (2015) Cell phones as a source of contamination of pathogenic bacteria in the health personnel of the Hospital de los Valles, Cumbayá, Ecuador in November 2014.
-
Menacho JO, Hjarles MG, Candela JO (2021) Contamination with pathogenic bacteria from stethoscopes of medical personnel in a level III hospital in Lima, Peru.
-
Pírez M, Mota M (2008) Morphology and bacterial structure.
-
Catalina Pírez M (2002) Morphology and Bacterial Structure.
-
Types of bacteria. Tiposde Online.
-
Mora X (2012) Direncciando Bacterias Gram + y Gram.
-
Science in the PIC (2021) Difference between Gram Positive and Gram Negative bacterial cell.
-
Flores TV, Vargas AK (2014) Bacterial Morphology. Revista de Actualización Clínica 49(2): 2594-2598.
-
Suazo JA (2012) Estrutura y morfología de las bacterias.
-
López JM, Berrueta TU (2017) Generalidades sobre las bacterias.
-
Cervantes RG, Sánchez GR (2017) La microbiota del humano. 60(2): 1-14.
-
Ribera LR (2010) Metagenomics: Sequencing the unknown.
-
Santambrosio E, Ortega M, Garibaldi P (2021) Cátedra de Biotecnología.
-
Biotechmind (2015) La tinción de Gram / Gram stain.
-
MINSA (2015) Bacteriological analysis of surfaces using the swab method.
-
Elika (2014) Bacterial contamination.
-
Lemelin MJ (2019) General Classification of Bacteria.
-
Pan American Health Organization (2019) Top 10 Health Threats 2019.
-
Cisneros F (2005) Theories and Models of Nursing. Pp: 1-15.
-
Hernández S (2008) Research Methodology. In: Grwaul MC (Ed.), In: 10th (Edn.), Mexico.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda