Server Illness Scale Based on the Disability-Adjusted Life Year Method (Daly=Yll+Yld): Monitoring to Prevent Risks and Reduce Incidents
Worker's health has shown to be an increasingly ascendant theme, in view of the epidemiological data that culminate in the progressive illness of those worked within their work environment. Currently, federal public servants have a system that takes care of their health and illness, performing from preventive measures to a medical board, but this system is still flawed in terms of monitoring illness and giving priority to care to reduce injuries. Therefore, this study aimed to carry out an epidemiological profile and design an illness scale based on this epidemiological profile. It was a quantitative, descriptive study, carried out with employees of IFAM - Campus São Gabriel da Cachoeira, following all ethical precepts. For the statistical analysis, SPSS 28.0 was used. As a result, an epidemiological profile was made based on 36 servers, male (26/61.5%), assume a leadership position (18/50%), have a preexisting disease (20/53.8%) and do not follow up health (33/88.5%). As for the scale, it was described with 3 variations (little urgent, urgent and emergent), 4 domains and 26 variables. From conclusions, it can be observed that the worker's health needs to be widely studied and worked on within a care network, this scale will subsidize a follow-up of the server's illness, but only when it is validated by a specialist, for now it is just a scale design.
Introduction
The field of Worker’s Health (ST) in Brazil is the result of an accumulated heritage of struggles and claims within the scope of Collective Health, with roots in the Latin American Social Medicine movement. The scientific and technological advancement of Preventive, Social and Public Health Medicine, during the 1960s/70s, expanded the interpretative framework of the health-disease process, including its articulation with work. At the same time, the concept of health was broadened, bringing an even greater basis for workers’ health, such as physical, psychological and social well-being [1].
This new way of apprehending the work-health relationship and intervening in the world of work introduces, in Public Health, health care practices for workers, in the set of proposals of the Brazilian Health Reform. A new paradigm is configured which, with the incorporation of some Social Science references, expands the vision of Occupational Medicine and Occupational Health, with the Marxist ideals being the precursors of these proposals [2].
The appropriation of the concept “work process” as an analysis tool makes it possible to reformulate still hegemonic conceptions that, by establishing simplified articulations between cause and effect, in a single or multicausal perspective, disregard the social and historical dimension of work and the health/disease binomial. Thus, workers’ health is configured as a field of interdisciplinary practices and strategic knowledge - technical, social, political, human- multiprofessional and interinstitutional, aimed at analyzing and intervening in work relationships that cause diseases and injuries [3]. Its benchmarks are those of Collective Health, that is, promotion, prevention and surveillance.
When we translate the TS into quality of life at work, the concepts and actions of health promotion and disease and injury prevention become more emergent. Linking health to work is instigating, considering that the worker transcends 60% of his life at work. This worker often falls ill due to intrinsic or extrinsic aspects, which may be linked to the work process. These illnesses generate physical, psychological and social exhaustion for the worker, which culminates in the reduction of years lived [4].
Analysis of the burden of disease is important for the development of indicators that support the planning, execution and evaluation of health actions. This is when the concept of estimating disability-adjusted life years (Disability Adjusted Life Years [DALY]), a composite indicator that integrates premature death (Years of Life Lost [YLL]) and damage caused by disease, sequelae or disability, considering different levels of severity of one or several diseases at the same time time (Years Lost due I’m Disability [YLD]) [5].
Using illness scales and the DALY method, we can concretely delve into health policies, which must adapt to the constant changes in the health profile of populations. In Brazil, the demographic and epidemiological transition has been designing a new scenario for the action of the Unified Health System (SUS), with the configuration of a triple burden of disease manifested by the concurrence of chronic diseases, infectious diseases and external causes [6]. There is a greater occurrence of causes related to circulatory and respiratory problems and neoplasms, especially in older age groups. The nutritional transition brought new challenges, with reduced physical activity and overeating overcoming malnutrition as a major risk factor for disease. In turn, regional inequality is still relevant, and for our reality of the IFAM, even more so, given that there are IFAM in less developed regions and poorer populations presenting a slower transition.
A point to exemplify is with regard to mental disorders, CID more concentrated in the removal of federal public servants, the DALY method is no different, one in every ten years of life lost due to death or disability – DALY – correspond to these causes. It is estimated that 30 million Brazilians had some mental disorder in 2010, which is equivalent to a prevalence of 15%. In a recent systematic review of population-based studies, a prevalence of depressive symptoms was observed between 13 and 16%, and of major depression between 12 and 19% of Brazilian adults [7]. However, there are few established strategies for detection, monitoring and treatment, as well as trained human resources at all levels of care for these illnesses. Interventions for prevention and control are multidisciplinary and multisectoral, and the health system must be a catalyst for these actions and not a passive recipient of the consequences of these injuries. One of the most important contributions of the burden of disease study is the estimation of the burden attributable to exposure to risk factors. In this sense, the objective of this study was to carry out an institutional epidemiological profile and design a scale to monitor the illness of servers.
Materials and Methods
It was a descriptive study, with a quantitative and qualitative approach in the Research Project modality. For Gil [8], research is defined as a rational and systemic procedure and aims to provide answers to proposed problems. According to Oliveira [9] the descriptive study describes a reality, through opinion polls, evaluation scales, market research and epidemiological data. The study was divided into two well-designed stages, the assembly of the illness profile of the IFAM server – CSGC and the elaboration of the illness scale based on the DALY method.
The entire project was developed at the Federal Institute of Science and Technology of Amazonas (IFAM) campus São Gabriel da Cachoeira. Where the population consisted of effective servers crowded on campus and the sample was 36 servers. The inclusion criteria applied to this project are: to be a servant of IFAM - CSGC, to be over 18 years of age and to accept to be part of the research. The research does not fit into Resolutions CNS nº 466/12, CNS nº. 510/16, bearing in mind that we will only carry out an epidemiological profile based on the diseases of the servers and after that we will elaborate the illness scale and no data used for scientific questions, only to design the scale questions, a waiver was requested, analyzed and approved TCLE by CEP, based on protocol: 64043522.1.0000.8119.
The elaboration of the scale was based on existing scales in the literature for assessing health and illness. It is noteworthy that there are many scales, but very specific to the psychic issue and these scales do not use Kanban. The scale was elaborated based on the Disability-Adjusted Life Year method (DALY=YLL+YLD), in order to verify how much is lost in years of life from a time of illness of the server.
The scale is composed of variables related to health and quality of life at work based on the DALY method, with a score for each type of leave and illness response. Statistical analysis of sociodemographic data was performed using the SPSS 28.0 statistical program, with categorical and continuous data described in tables and frequencies and a CI of 95% and a p< 0.5
Results and Discussion
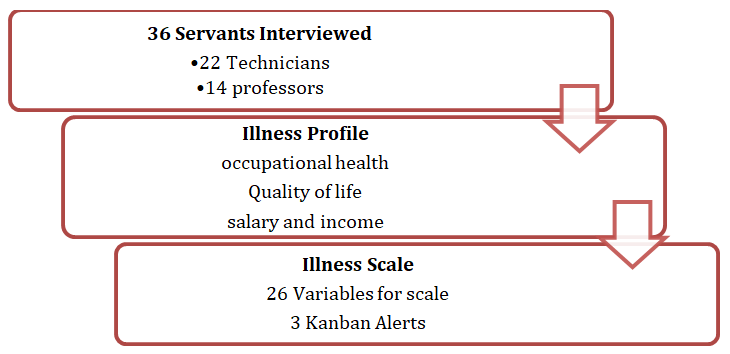
The entire trajectory of the study took place at IFAM – CSGC, where the target audience was the effective servant. The objective of the study was to draw an illness profile and later, based on this profile, to develop the server’s illness scale, with the purpose of monitoring the health of the server using the DALY and Kanbans method. The initial design of the study is shown in Figure 1, with details of the sample and how the other steps were followed until reaching the scale description.
The servants interviewed are all assigned to the IFAM – CSGC and their occupational health data served to support the scale variables. The data to assemble the illness profile focused on occupational health, quality of life and salary and income factor. Based on these data, an illness scale was described with 26 variables and 3 Kanban alerts for each variable, green (non-urgent), yellow (urgent - intervention within 48 hours) and red (emergent - needs immediate intervention).
During the interviews, the servers’ Vital Signs (SSVV) were also measured. Servers, before being interviewed, were informed that their data would only be used to draw a profile in order to have an epidemiological basis for preparing the illness scale. Of the participants, 26 (61.5%) are male and 10 (38.5%) are female, all residing in São Gabriel da Cachoeira - AM, but 48.2% are from another state. Other social data are described in Table 1.
| social characteristic | n = 26 (CI: 95%) p <0.05 |
|---|---|
| Age | 42 ± 10 |
| Catholic religion | 28 (69.2%) |
| leadership position | 18 (50%) |
| Service time | 7.3 ± 4.5 |
| Salary range (number of minimum wages) | 4.8 ± 1.7 |
| loan acquisition | 29 (80.8%) |
Table 1: Socio-epidemiological data of the participants (n=36) that may interfere with their physical and mental health. São Gabr
Source: SMSL, Montenegro, 2023. Table 1: Socio-epidemiological data of the participants (n=36) that may interfere with their physical and mental health. São Gabriel da Cachoeira – AM, 2023.
In Table 1, what draws our attention is the issue of acquiring loans by public servants, where 80.8% of the servants interviewed so far have some type of loan, which reflects a national estimate. As it is an Interior Institute, the vast majority of employees have already assumed a leadership position, but at the moment 50% of them are assuming a leadership position. The salary range is around 5,800.00 reais, even for those servants who occupy some position with gratuity.
Seynaeve, et al. [10] spoke in a survey conducted with 17 civil servants, from 2009 to 2013, who were removed from their work activities due to illness. Of that sample, 10 employees were removed from work due to illness, in the mentioned period, of these: 04 make up the group of managers and 01 health professional (psychology). In addition to 01 representative of DSO/SEAD and 01 representative of the Union of Public Servants of the State‐SINPUB. The 15 civil servants surveyed occupied mid-level, higher-level positions and managers of the boards that make up the institution. This study is consistent with the data presented in Tables 1 & 2, therefore, we worked with a small but representative population. As for health data, pre-existing diseases and evaluation of vital signs in order to confirm the reports of the servers, we can check the data described in Table 2.
| Feature | n = 26 (CI: 95%) p <0.05 |
|---|---|
| Have pre-existing disease | 20 (53.8%) |
| Does not have health insurance | 34 (92.3%) |
| No health monitoring | 33 (88.5%) |
| Year of last medical examination | 2020 |
| Year of last visit to the doctor | 2020 |
| No psychological follow-up | 34 (92.3%) |
| Systolic Blood Pressure (SBP) | 122.5 ± 16.3 |
| Heart Rate (HR) | 76 ± 11 |
| Saturation | 98% ± 0.8 |
| Body Mass Index (BMI) | 24 ± 2.9 |
| Glycemia | 102 ± 38.5 |
Table 2: Health data, pre-existing diseases and evaluation of partial signs of the participants (n=36). São Gabriel da Cachoeira,
Source: SMSL, Montenegro, 2023. Table 2: Health data, pre-existing diseases and evaluation of partial signs of the participants (n=36). São Gabriel da Cachoeira, 2023.
Table 2 calls our attention because 46.2% (n=12) of the participants say they do not have a pre-existing disease, but the mean blood pressure was type I hypertension and the blood glucose doctor was pre-diabetic, in addition the BMI was very borderline and close to the overweight value. Heart rate remained within normal adult standards. The pre-existing diseases most cited by the servers are diabetes mellitus and systemic arterial hypertension. No infectious disease was cited. During the interview, the servants were asked about their vaccination card, which made the researchers very excited, given that the servants’ vaccination cards are up-to-date for immunobiologicals related to the occupational environment.
The health condition of the servers during the recruitment process was evidenced in the performance of vital signs, it is worth pointing out that there is no periodicity for the health evaluation of the servers, despite the Labor Laws obliging this practice, in the Federal scope the periodic evaluation of the servers’ health is still scarce. As the health of federal servers does not have a periodicity for evaluation, this demands a higher risk of diseases and a higher score on the Daly scale, considering that the more diseases, the more time of life lost.
Silva [11] reports in his study that at the time of their hiring, civil servants were submitted to an expert medical examination of admission, having been considered able to join the public service. However, it is instigating the fact that civil servants considered able to work, in less than five years, became sick due to work, which has constituted a significant demand. In this study, we did not perform an illness analysis, given that the purpose of the scale is to prevent illness, but we can observe that in the measurement of the vital data of the servants, we had an altered value for blood glucose and blood pressure, even for servants who do not have comorbidities.
After verifying these data and studying existing scales in the field of health, such as the fugulin scale , morse scale , braden scale , quality of life assessment scale, in addition to studies on quality of life, we determined that the developed scale would have 4 domains: biological domain (10 variables), socioeconomic domain (6 variables), psychosocial domain (5 variables) and organizational domain (5 variables). In Brazil, there is a validated and tested quality of life scale [12]
for adults, with 23 variables distributed in two domains, behavioral (9 variables) and psychological (14 variables), with some variables being equivalent to those determined in this scale, as shown in Table 3.
| Domain | Variables | Kankan | ||
|---|---|---|---|---|
| little urgent | Urgent | emerging | ||
| Biological | Age | 20 – 40 years | 40 – 60 years | Over 60 |
| Preexisting Disease | 1 | two | more than 2 | |
| medical follow-up | 1 year ago | 2 years ago | More than 2 years ago | |
| vaccines | Lack of reinforcement | incomplete schemes | there is no vaccine | |
| Continuous medication use | 1 | two | more than 2 | |
| Withdrawal in the last year | two | 4 | more than 4 | |
| Illness in the last year | two | 4 | more than 4 | |
| Hospitalization in the last year | No | Up to 2 | more than 2 | |
| Deficiency | No | Yes | yes, disabling | |
| Allergy | No | Yes | Yes | |
| Socioeconomic | religiosity | have and practice | Yes, but don’t practice | It does not have |
| Salary range | More than 4 minimum wages | 3 - 4 Minimum wages | 2 Minimum wages | |
| Laser | 2 activities | 1 activity | It does not have | |
| Loan | No | Up to 2 | more than 2 | |
| Service time | 0 – 3 years | 45 years | More than 5 years | |
| Home | Own home | Rented house | Rented house | |
| Psychosocial | mental health monitoring | No | Yes | Yes |
| Use of psychotropic | No | Up to 2 | more than 2 | |
| Mental illness in the last year | No | Yes | Yes | |
| family tie | Yes | Little | ||
| Social isolation | No | Little | Very | |
| Organizational | professional satisfaction | Yes | Few | No |
| workload | 20 hours | 40 hours | 60 hours | |
| Occupational health activity | Yes | Sometimes | Never | |
| leadership position | No | Yes | Yes | |
| Number of team members | 0 - 5 | 06-Oct | more than 10 |
Table 3: Server illness scale domains and variables. São Gabriel da Cachoeira-AM, 2023.
Source: SMSL, Montenegro, 2023. Table 3: Server illness scale domains and variables. São Gabriel da Cachoeira-AM, 2023.
Conclusions
This study concludes that the worker’s health theme still needs to be widely worked on so that we can have robust data, in addition, when we deal with the federal sphere, we still have an educated and built structure of health care for the server, but when it comes to the health of the server in states and municipalities, the deficiency is even greater. As servers are in a constant process of becoming ill, working with a scale that prevents this illness is fundamental, in this sense this scale will be reassessed, validated and restructured by specialist judges in later projects so that we have a system that monitors the process of illness of the server public.
It is also concluded that the scale proposed in this study will be validated, restructured, applied and validated by expert judges in future projects, therefore it is not yet ready for use, given that scales to be used need to be validated by judges in the area. For this study, only a situational diagnosis was made and determination of the variables and domains necessary for the scale, so the scale was described as shown in Table 3. Kanbans are painful for each domain, regardless of the final value, considering that each variable adds up to the domain, but this domain does not have interference of minimum or maximum values, therefore the scores must be verified by variables.
We were not able to verify absenteeism in order to cross-reference data with the Daly scale, since the system that works with the health of public servants in the federal network and establishes the absenteeism rate cannot be accessed p It is also in this sense that we need a scale to monitor illness, so that we have robust data for monitoring and quality of life.
References
-
(1994) DIAS EC Health Care for Workers in the Health Sector (SUS) in Brazil: reality, fantasy or utopia. Campinas: State University of Campinas.
-
Joseph B, Joseph M (1994) Health Reform and Worker’s Health. Health and Society 3(1): 41-59.
-
Minayo-Gomez CM, Thedim-Costa SMF (1997) The construction of the field of workers’ health: route and dilemmas. Cad Public Health 13(S2): 21-32.
-
Minayo-Gomez CM, Vasconcellos LCF, Machado JMH (2018) Occupational health: historical aspects, advances and challenges in the Unified Health System. Ciência & Saúde Coletiva 23(6): 1963-1970.
-
Murray CJL, Ezzati M, Flaxman AD, Lim S, Lozano R, et al. (2010) GBD 2010: design, definitions , and metrics . Lancet 380(9859): 2063-2066.
-
Mendes EV (2010) Health care networks. Science Collective Health 15(5): 2297-2305.
-
Silva MT, Galvao TF, Martins SS, Pereira MG (2014) Prevalence of depression morbidity among Brazilian adults : a systematic review and meta- analysis . Rev Bras Psiquiatr 36(3): 262-270.
-
Gil CA (2007) How to design research projects. Sao Paulo: Atlas.
-
Oliveira MM (2007) How to do qualitative research. Petropolis, Voices.
-
Seynaeve CVMS, Gomes VLB (2018) Work Management and Illness of Public Servants in JUCEPA1: reflections on the work of the social worker. 20(2): 45‐64.
-
Silva E (2011) Work and mental exhaustion: the right to own oneself. São Paulo: Cortez.
-
Soares I, Silva A, Chariglione I, Formiga N, Melo GF (2019) Quality of life scale (eqv): psychometric evidence of measurement in adults. Psicologia, Saúde & Diseases 20(2): 328-347.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda