An Observational Study on Prescription Pattern of Antibiotics Using WHO Indicators in Primary, Secondary, Tertiary Care–A Need for Antimicrobial Stewardship
Background: Antibiotics have revolutionized modern medicine, playing a pivotal role in treating infectious diseases and preventing life-threatening complications. However, antibiotic misuse and overuse have resulted in the emergence to antibiotic resistance, posing a hazard to global public health. As a result of the rising epidemic, it has become critical to investigate and correct antibiotic prescribing behaviors in primary and secondary care settings. This environment allows for an observational research that evaluates antibiotic prescribing trends using World Health Organization (WHO) indicators and emphasizes the critical need for Antimicrobial Stewardship Programs (ASPs). As assessment metrics, the WHO indicators such as the proportion of antibiotics prescribed by class, the percentage of antibiotics administered without a recognized diagnosis, and the percentage of antibiotics prescribed from the essential medications list were used. Aim: This observative study aimed to assess the prescription patterns of antibiotics in primary and secondary care settings using the World Health Organization (WHO) indicators and to highlight the pressing need for Antimicrobial Stewardship Programs (ASPs) to combat this critical issue. Methods: The study was conducted on total no of 351 patients were included and studied in which 176 patients from primary care setting and 185 patients from primary, secondary and tertiary care setting with their respective prescribed antibiotics for a period of 6 months at apollo hospitals, apex hospitals on those who had age above 20. All prescription records containing antibiotics within a defined time period of will be included in the sample. Results: The inferential statistics results showed that the A p-value of 6.4E-25 is an extremely small p-value in the context of a statistical test, such as a chi-square test. This value represents a highly significant result, which representing there is significant variance in the prescription of antibiotics. The analysis of inpatient antibiotic usage revealed that a substantial proportion of patients (89.3%) received antibiotic treatment during their hospital stay. However, when assessing the appropriateness of antibiotic prescriptions, it was found that only 74.1% of antibiotic-containing prescriptions met the criteria for proper use, suggesting a potential area for improvement in antibiotic prescribing practices within the inpatient and outpatient setting. Conclusion: This observative study sheds light on the suboptimal prescription patterns of antibiotics in primary and secondary care, emphasizing the critical role of Antimicrobial Stewardship Programs in addressing this issue. These programs are essential for preserving the effectiveness of antibiotics, safeguarding public health, and mitigating the looming threat of antibiotic resistance.
Introduction
Since their discovery in the early 20th century, antibiotics have been a remarkable and revolutionary class of pharmaceuticals that have changed the medical sector. These substances, which are either chemically produced or obtained from natural sources, have had a significant influence on global public health and have been essential in the treatment of bacterial diseases.
The term “antibiotics” is derived from the Greek words “anti,” meaning against, and “bios,” meaning life [1]. Indeed, antibiotics are agents designed to combat life-threatening bacterial infections by targeting the vital processes of bacteria, either killing them outright (bactericidal) or inhibiting their growth and reproduction (bacteriostatic). Since their discovery, antibiotics have transformed contemporary medicine by being essential in treating a broad range of bacterial illnesses and saving countless lives [2]. These amazing medications are vital weapons in the fight against bacterially-based infectious disorders. Antibiotic usage requires a well-thought-out plan in order to maximize their effectiveness, prevent antibiotic resistance from developing, and protect public health.
Understanding the multifaceted world of antibiotics is crucial for both healthcare professionals and the general public, as these medications continue to be integral in our ongoing battle against bacterial diseases and their evolving complexities.
Antibiotics are without a doubt essential to all healthcare settings and play a crucial role in global health systems. Despite the fact that antibiotics are a vital component of hospital healthcare and have saved many lives, up to 20–50% of prescription antibiotics are misused globally [3]. This raises the frequency of adverse medication events and has a significant impact on the treatment expenses and quality of the healthcare system. Antimicrobial resistance (AMR) occurs when bacteria, viruses, fungi and parasites change over time and no longer respond to previously recommended antibiotics. This makes it difficult to treat infections, thereby, increasing the risk of disease spread, severe illness and death. There are reports that suggest that Acinetobacter species, Pseudomonas species, Escherichia coli, Klebsiella pneumoniae, Salmonella enterica, Staphylococcus aureus and Streptococcus pneumonia have become resistant to commonly used antimicrobials [4].
Recent reports also suggest that some microorganisms have developed resistance to carbapenems, which are antibiotics often used as last resort for K. pneumonia infections. It is estimated that approximately 700,000 deaths occur annually as a result of AMR and deaths from AMR could rise to 10 million by 2050 if no concerted action is taken [5]. The association between antimicrobial use and resistance has been well documented in a number of individual healthcare facilities, communities and countries. There is sufficient data to suggest association between AMR and the levels of antimicrobial use [6]. Moreover, a general trend toward the usage of broad-spectrum and last-resort antibiotics has been shown by recent investigations. Antimicrobial stewardship (AMS) initiatives have changed globally in reaction to AMR. Among other things, these AMS programmed seek to increase health professionals’ ability, encourage the prudent use of antibiotics, and increase public knowledge of AMR.
Selective antibiotic pressure is an important determinant of emergence and dissemination of antibiotic resistance [7]. It is also one of the few variables that may be changed to increase the risk of antibiotic resistance. A number of common challenges may be discovered in studies assessing the relationship between antibiotic exposure and resistance, such as assessments of resistance outcomes, inadequate correction for significant confounding factors, control group selection, and the amount of prior antibiotic exposure [8]. Furthermore, the relationship between antibiotic exposure and antibiotic resistance has been assessed using a variety of research designs, units of analysis (either the group or the person), and methods for evaluating exposure and result. Studies are hard to compare because of their variability.
Currently, the Centre’s for Disease Control and Prevention (CDC) warns health professionals to work in improving antibiotic prescribing practice and use in human health care, and recommends the establishment of an Antibiotic Stewardship Program (ASP). Changing prescribing behaviors could be difficult, but there are proven, evidence- based methods to optimize antibiotic therapy for individuals while minimizing harm to the patient and reducing ABR in the community. Thus, the rational use of antibiotics is a major health need [9].
Primary Care and Secondary Care
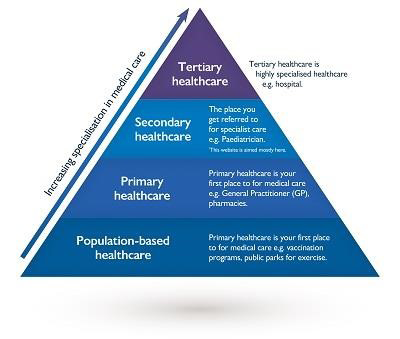
Primary Care and Secondary Care are two fundamental components of healthcare systems, each serving distinct roles in delivering medical services. These terms represent different levels of care and are essential for organizing and providing comprehensive healthcare services to individuals and communities. Primary Care: Primary care refers to the first point of contact for individuals seeking medical assistance within the healthcare system [10]. It is typically provided by general practitioners (GPs), family physicians, pediatricians, and nurse practitioners.
Key Characteristics
- Focuses on preventive care, health maintenance, and early intervention.
- Provides routine healthcare services, including check- ups, vaccinations, and screenings.
- Addresses common medical concerns and non- emergency health issues.
- Establishes a long-term patient-provider relationship for continuous care.
- Serves as a gateway to specialized care when necessary, referring patients to secondary care or specialty services.
Services Provided
- Management of chronic conditions (e.g., diabetes, hypertension).
- Diagnosis and treatment of common illnesses and injuries.
- Health promotion and education.
- Routine physical examinations.
- Immunizations and preventive care.
- Basic mental health support and counselling. Settings: Primary care is often delivered in outpatient settings, including clinics, family physician offices, community health centers, and urgent care facilities. Secondary Care: Secondary care refers to specialized medical services that are typically more focused and provided by specialists and healthcare professionals with specialized training and expertise [10].
Key Characteristics
- Addresses specific health conditions, diseases, or injuries requiring specialized knowledge and equipment.
- Involves consultation and treatment by specialists, such as cardiologists, orthopedic surgeons, dermatologists, and radiologists.
- Often requires referrals from primary care providers or emergency departments.
Services Provided
- Surgical procedures and interventions.
- Diagnosis and management of complex medical conditions.
- Specialized medical imaging (e.g., MRI, CT scans).
- Care for specific organs or systems (e.g., cardiology, neurology).
- Cancer treatment (oncology).
- Management of psychiatric and mental health disorders by psychiatrists. Settings: Secondary care services are typically delivered in hospitals, specialized clinics, and healthcare facilities equipped with advanced medical technology and specialized personnel.
Tertiary Care
It refers to a level of healthcare that involves specialized medical services and treatments that are often provided in hospitals or specialized medical centers [10]. This level of care is typically more complex and advanced than primary and secondary care.
Tertiary care includes services such as:
- Specialized Surgery: Complex surgical procedures that require specialized training and equipment, such as organ transplants, cardiac surgery, and neurosurgery.
- Cancer Treatment: Oncology services for the diagnosis and treatment of cancer, including chemotherapy, radiation therapy, and cancer surgeries.
- Cardiac Care: High-level cardiac care, including heart surgery, interventional cardiology, and cardiac rehabilitation.
- Neurological Care: Treatment of complex neurological conditions, including neurosurgery, stroke care, and management of conditions like Parkinson’s disease.
- Transplant Services: Organ transplantation, including kidney, liver, heart, and lung transplants.
- Burn Care: Specialized care for severe burns, often provided in burn centers.
- Trauma Care: Treatment of severe injuries resulting from accidents or emergencies, often in trauma centers.
- High-Risk Obstetrics: Management of high-risk pregnancies and complicated deliveries.
Tertiary care is typically delivered by highly specialized healthcare professionals, including surgeons, subspecialty physicians, and medical teams with advanced training and expertise. Patients are usually referred to tertiary care facilities by primary care or secondary care providers when they require specialized treatments or interventions that are not available at lower levels of car (Figure 1).
The World Health Organization (WHO) has published a list of essential medicines, which includes antibiotics recommended for use in primary care and secondary care settings. This list is periodically updated to reflect the latest evidence and treatment guidelines [11]. Keep in mind that specific recommendations may vary by region and local resistance patterns. As of my last knowledge update in September 2021, here are some antibiotics commonly used in primary and secondary care:
- Amoxicillin: A broad-spectrum penicillin antibiotic commonly used for treating a wide range of bacterial infections, including respiratory and urinary tract infections.
- Ciprofloxacin: A fluoroquinolone antibiotic effective against a variety of bacterial infections, including urinary tract and gastrointestinal infections.
- Trimethoprim-sulfamethoxazole (Co-trimoxazole): Used for respiratory tract infections, urinary tract infections, and as prophylaxis for opportunistic infections in certain immunocompromised patients, like those with HIV/AIDS.
- Doxycycline: A tetracycline antibiotic used for the treatment of various infections, including respiratory tract infections, acne, and some sexually transmitted infections.
- Erythromycin: A macrolide antibiotic used when penicillin is not suitable or for patients with penicillin allergies.
Secondary Tertiary Care Antibiotics
- Ceftriaxone: A broad-spectrum cephalosporin antibiotic often used in hospitals for serious bacterial infections like sepsis, meningitis, and complicated intra-abdominal infections.
- Vancomycin: An antibiotic primarily used for the treatment of serious Gram-positive bacterial infections, including methicillin-resistant Staphylococcus aureus (MRSA).
- Meropenem: A carbapenem antibiotic used to treat a wide range of serious bacterial infections, including Core competencies for antimicrobial prescribing: C1: Understands the patients and their clinical needs. C2: Understands treatment options and how they support the patient’s clinical needs. C3: Works in partnership with the patient and other healthcare professionals to develop and implement a treatment plan. C4: Communicates the treatment plan and its rationale clearly to the patient and other health. C5: Monitors and reviews the patient’s response to treatment.
Antimicrobials are indicated clinicians must prescribe the most appropriate drug at the right dose via right route of administration and for the most appropriate duration. Although the timing may differ in outpatient and inpatient first clinicians must make a clinical assessment by performing a history and physical examination [12]. Then they determine the further diagnostic is necessary and deciding the therapeutic decisions including the antimicrobials if indicated and other drugs that can provide the symptomatic relief intrinsic to this decision making process is the consideration of the local epidemiology such as national surveillance data and local antimicrobials susceptibility data relevant to patient’s presentation throughout the encounter clinicians provide patient education regarding their illness.
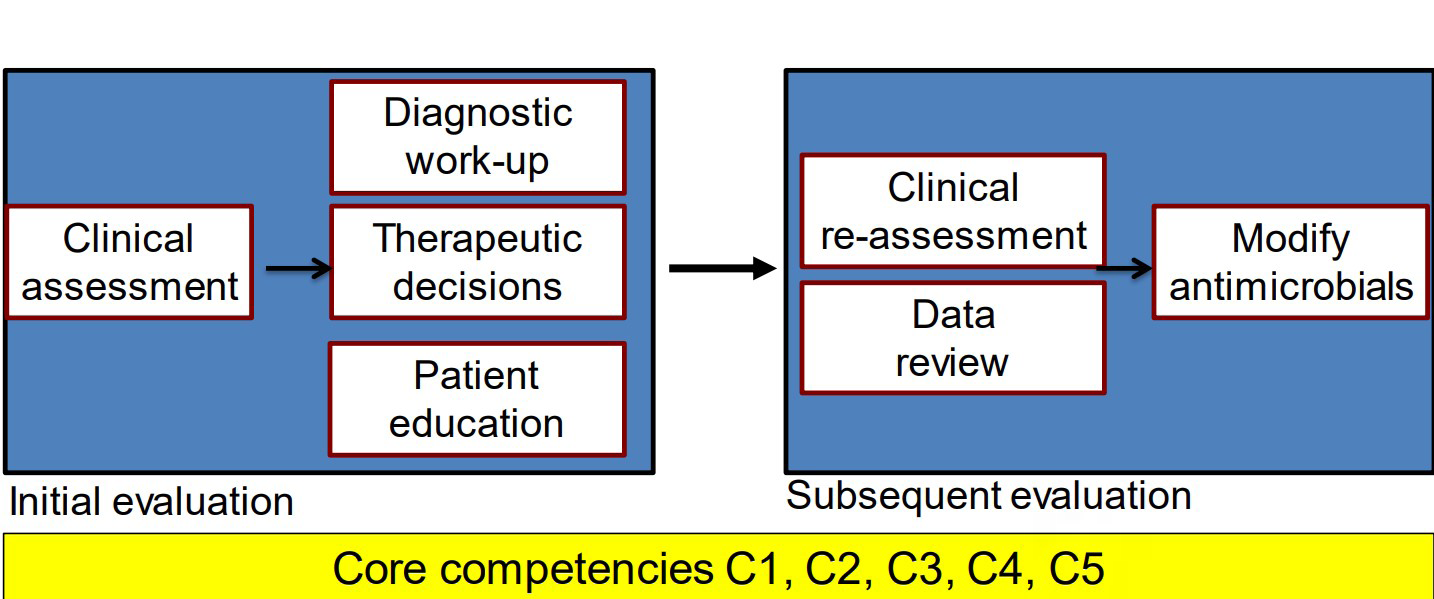
Clinicians will follow up on outcomes, including microbiological results, if diagnostics such a urine culture are performed at the initial visit. The turnaround time for results may vary based on the resources available. In certain cases, clinicians may also reevaluate their patient and, if necessary, modify their original decision-making regarding antimicrobials as directed by the microbiological data. Reassessment is necessary in the management of hospitalized patients, and it may also call for expert consultation with a clinical microbiologist pharmacist or infectious disease specialist, depending on the clinical situation and the patient’s trajectory. The identification of organisms and susceptibilities to antimicrobials from culture often take several days. [13].
Category Use of Antibiotics in Primary and Secondary Care Setting
Categories use of antibiotics is
- Prophylaxis
- Empiric
- Definitive
Prophylaxis: Prophylaxis include antimicrobials used to prevent opportunistic infections in immunocompromised patients and those administered to surgical site infections antimicrobial prophylaxis should only be used when supported by evidence based guidelines.
Empiric: Empiric antibiotics are given before the microbiological data to support this diagnosis available much of antimicrobial use in both inpatient and outpatient setting falls into empiric category.
Definitive: Antimicrobial therapy is considered definitive and also targeted when it is specifically including the results of susceptibility testing at this stage (Figure 3).
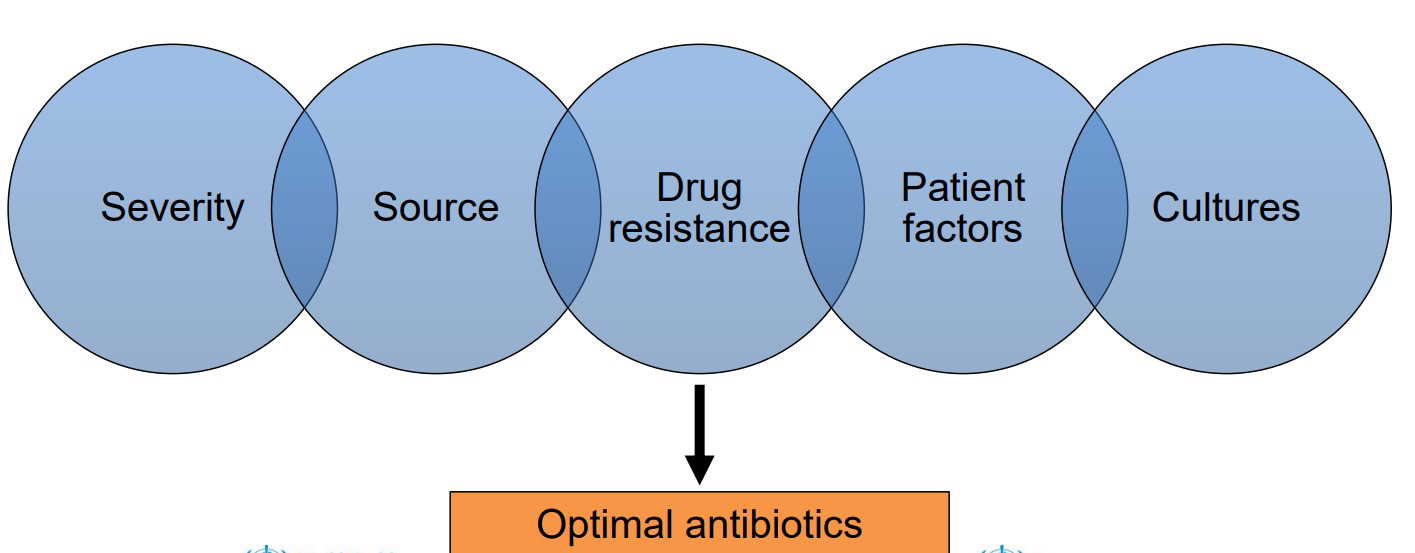
Epidemiological factors included for primary and secondary care setting: Figure 3: Epidemiological factors included in primary and secondary care.
• Severity Critical illness or stable outpatient. Timing, route and spectrum of antibiotic using. Since there is little margin of error when treating critically ill patients, a limited spectrum of antibiotic activity up front may result in significant morbidity or mortality; however, this is frequently not the case for stable outpatients, for whom an empiric narrow spectrum antibiotic regimen may be more appropriate. Critically ill patients require prompt decision- making and timely administration of antibiotics.
• Source → Likely source → Source control What is the most likely pathogen and where is the infection most likely to have originated? By responding to these inquiries, physicians can ascertain the range of antibiotic treatment that is required for a certain infection, such as an abscess, in order to promote clinical recovery. This is sometimes referred to as source control clinicians. To make this decision, we take into account the clinical presentation, which includes the patient’s history, physical examination, and, if necessary, laboratory and radiographic data [13].
• Drug resistance Recent antimicrobial use local cumulative susceptibility data. How likely resistant is this infection due to a drug organisms.
**
- Patient factors**
- Allergies: Clinicians should consider history of the doing allergies such as Anaphylaxis. The spectrum of antibacterial therapy you choose is also driven by the answer to this question.
- Renal on liver dysfunction. Clinician should access the Remodel. Mystery of Penal dysfunctions / Liver dysfunction Ex: Aminoglycosides should be used with Caution in pt’s with renal dysfunction drug penetration metabolism I excretion parameters dictate appropriate dosing intervals for many antimicrobials.
• Cultures Blood cultures should ideally be started before antimicrobials. When indicated, it’s important to obtain cultures prior to starting antimicrobials if the patient’s clinical condition allows for immediately life-threatening infections; however, treatment initiation should not be delayed for the purpose of obtaining cultures because doing so frequently reduces the sensitivity of the samples [14]. Ex: sputum sample blood cultures however, should ideally be obtained before antibiotic therapy is started.
Prescription pattern monitoring studies (PPMS) are used to assess how medicines are prescribed, dispensed, and distributed in a particular location. The goal of PPMS is to help ensure that medicines are used rationally.
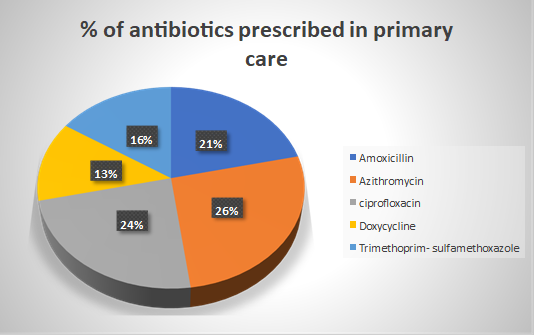
The most frequently prescribed antibiotics are: Metronidazole (25.9%) Amoxicillin with clavulanic acid (22.0%) Amoxicillin (16.4%) Ciprofloxacin (10.1%) According to the WHO “AWaRe” classification, the “access” group of antibiotics was the most prescribed (74%), followed by the “watch” group (24%). The majority of antibiotics (60.2%) were prescribed for more than 7 days.
In 2020, healthcare providers in the United States prescribed 201.9 million antibiotic prescriptions.
This is equivalent to 613 antibiotic prescriptions per 1,000 people [15].
There is an association between geographical location and higher antibiotic prescribing levels (Figure 4).
Prescription Practices of Antibiotics in India
In recent times, India’s antibiotic prescribing policies have attracted a lot of attention due to the country’s increasing prevalence of infectious illnesses and its dual- sector healthcare system. The abuse of antibiotics has far- reaching consequences in India, impacting the health of individual patients and adding to the worldwide problem of antibiotic resistance [16]. In India, medical professionals such as doctors, physicians, and pharmacists may administer antibiotics under specific circumstances. Although the prescription procedure adheres to accepted medical procedures and recommendations, there may be variances in practice based on the kind of infection, the healthcare facility, and the clinical judgement of the physician [17]. It’s critical to stress that the optimal use of antibiotics should be prioritized in order to avoid antibiotic resistance, and that prescriptions for antibiotics should be based on evidence-based guidelines. In order to tackle the rising issue of antibiotic resistance in India and throughout the world, overprescribing or prescribing antibiotics for viral diseases should be avoided [18]. In order to encourage responsible antibiotic usage and inform medical professionals and the public about reasonable antibiotic prescribing, healthcare providers and legislators are focusing more and more on antibiotic stewardship initiatives [19].
The most often given antibiotics in India might change depending on a number of variables, including prescribing patterns, prevalent infectious illnesses, geographical variations, and the kind of healthcare facility. However, because of their wide range of action and potency against common bacterial illnesses, a number of antibiotics are widely utilized in India [20]. The following are some of the antibiotics that are often administered in India: Metronidazole, Co-trimoxazole, Clarithromycin, Amoxicillin, Ciprofloxacin, Azithromycin, Cefixime, Doxycycline, Amoxicillin-Clavulanate, Ceftriaxone, and Cefixime [21].
In India, prescriptions for antibiotics are often written for a variety of infectious diseases and conditions [22]. The primary applications of antibiotics in India may vary depending on a variety of factors, such as patient demographics, medical procedures, and the prevalence of specific illnesses in the region. On the other hand, antibiotic prescriptions are frequently written for certain conditions and diseases in India [23].
Antimicrobial Resistance Requires a Global Solution
The World Health Organization (WHO) lists AMR among top 10 threats for global health. Antimicrobial resistance threatens human and animal health and welfare, the environment, food and nutrition security and safety, economic development, and equity within societies [24].
- Improve awareness and understanding of AMR through effective communication, education and training.
- Strengthen knowledge through surveillance and research.
- Reduce the incidence of infection.
- Optimize the use of antimicrobial medicines in human and animal health.
- Develop the economic case for sustainable investment (in AMR).
According to recent estimates, in 2019, 1.27 million deaths were directly attributed to drug resistant infections globally. By 2050, up to 10 million deaths could occur annually [25]. If unchecked, AMR could shave US$ 3.4 trillion off GDP annually and push 24 million more people into extreme poverty in the next decade [26].
Antimicrobial resistance in mycobacterium tuberculosis, malaria parasites, viruses, and HIV is becoming a reality that could increase human suffering [27]. It could also deal a huge blow to the world economy due to productivity losses, increased healthcare costs and a rise in poverty [28]. Even if it is a global crisis, poverty, lack of sanitation and poor hygiene make AMR worse. Also, AMR disproportionately impacts Low-Income Countries and Lower-Middle-Income Countries. AMR is thus an equity issue too [29] (Figure 5).
- Improve awareness and understanding of AMR through effective communication, education and training [30].
- Strengthen knowledge through surveillance and research.
- Reduce the incidence of infection
4. Optimize the use of antimicrobial medicines in human and animal health 5. Develop the economic case for sustainable investment (in AMR) [31].
Need for the Antimicrobial Stewardship Programme (ASP)
Antimicrobial stewardship is a coordinated program that promotes the appropriate use of antimicrobials (including antibiotics), improves patient outcomes, reduces microbial resistance, and decreases the spread of infections caused by multidrug-resistant organisms [32].
ASP is of the utmost importance as a way to optimize the use of antibiotics to prevent the emergence of resistance and improve patient treatment outcomes. Thus, the use of the term “antibiotic stewardship” has grown exponentially in recent years, typically referring to programs and interventions that aim to optimize antibiotic use [33]. ASP comprises interventions to prevent drug resistant bacterial infections, select antibiotic therapy targeted toward susceptible or resistant bacteria, and reduce unnecessary or inappropriate antibiotic administration and use [34]. 10,11 In clinical practice, ASP focuses on coordinated interventions designed to improve and measure the appropriate use of antibiotic agents by promoting the timely selection of the optimal antibiotic regimen of dose, duration of therapy, and route of administration [35].
AMS Competencies
Competencies are defined as the development of observable ability of a person (or individual health worker) that integrates knowledge, skills and attitudes in their performance of task. Competencies are durable, trainable and, through the expression of behaviors, measurable [36]. AMS competencies are the guiding set of knowledge, skills and attitudes that result in durable, trainable and measurable behaviors facilitating better prescribing of antibiotics [37].
Some of the key concepts to keep in mind when prescribing antibiotics include the following:
- Awareness of the health-care facility’s standard treatment guidelines [38].
- The importance and rationale for using recommended empirical antibiotic agents for patients, but also the potential immediate and long-term harm of broad- spectrum therapy [39].
- The benefit and safety of de-escalation antibiotic treatment after cultures.
- The opportunity and benefits of IV-to-oral switching [40].
All Healthcare Professionals Can Support AMS by Adhering to the 8 Principles of Good AMS
a. Recognize clinical evidence of infection. For example, consider the signs and symptoms and whether they might represent infection [41]. b. Avoid unnecessary antimicrobial use. For example, recommend symptom relief for self-limiting infections, with safety netting advice, and direct patients and carers [42]. c. Choose an antimicrobial that will have the most benefit and cause the least harm. For example, use best-practice treatment guidelines on using a ‘green’ antimicrobial in preference to a ‘red’ antimicrobial if an antimicrobial is needed [43]. d. Optimize the dosing regimen and route. For example, ensure patient is prescribed correct dose, frequency and route. e. Minimize the duration. For example, avoid unnecessary prolonged courses of antimicrobials. f. Assess response to treatment. For example, review any available microbiological sample results to guide treatment. g. Communicate effectively about antimicrobials. For example, discuss the issue of AMR with patients h. Prevent infection. For example, arrange vaccination and use IPC measures. Healthcare professionals can also engage in regular education relating to AMS and participate in local or national quality improvement audits for antimicrobial use [43]. i. Aim The aim of this project is to assess the prescription pattern of antibiotics in both primary and secondary healthcare settings using WHO indicators and to determine the necessity and feasibility of implementing an Antimicrobial Stewardship Programme (ASP) to optimize antibiotic use.
Objectives
- To Evaluate Antibiotic Prescription Practices • To examine the current antibiotic prescription patterns in primary and secondary care facilities. • To assess the types of antibiotics commonly prescribed. • To determine the dosages and durations of antibiotic courses prescribed.
- To Apply WHO Indicators • To calculate the Percentage of Prescriptions with Antibiotics (PPA) in the studied healthcare settings.
- To Compare Primary and Secondary Care Settings • To compare antibiotic prescription patterns between primary care and secondary care facilities. • To identify any significant differences in the types and quantities of antibiotics prescribed.
- To Evaluate Adherence to WHO Guidelines • To assess the extent to which antibiotic prescriptions adhere to WHO guidelines and recommendations. • To identify areas where antibiotic prescription practices may deviate from established guidelines.
- To Investigate Antibiotic Resistance Implications • To explore the potential implications of current antibiotic prescription patterns on antimicrobial resistance. • To assess the risk factors associated with the development of antibiotic resistance in the studied healthcare settings.
- To Assess the Need for Antimicrobial Stewardship Programme • To synthesize the findings to determine the necessity of implementing an Antimicrobial Stewardship Programme. • To evaluate the feasibility of establishing an ASP in the studied healthcare institutions.
- To Make Recommendations • To provide evidence-based recommendations for optimizing antibiotic prescription practices. • To suggest strategies for the development and implementation of an effective Antimicrobial Stewardship Programme.
8. To Contribute to Public Health Knowledge
- To contribute valuable insights and data to the field of antimicrobial stewardship and antibiotic resistance.
- To support public health efforts aimed at combating antimicrobial resistance.
Methods
Study Design
- This study will employ an Case control observational research design.
- Data will be collected by reviewing medical records and prescriptions.
Study Site
St. Theresa Hospital, Sanathnagar, Hyderabad.
Study Period
6 Months
Study Setting
The study was conducted in both primary care facilities (e.g., general practitioner clinics, community and secondary care facilities (e.g., hospitals, specialized clinics) within the selected region/area.
Sampling
- Sampling Technique: Stratified random sampling will be used to ensure representation from both primary and secondary care settings.
- Sample Size: The sample size will be determined based on the population of each type of healthcare facility within the study area, ensuring adequate representation.
- Inclusion Criteria: All prescription records containing antibiotics within a defined time period of will be included in the sample.
- Age group from 20-70 years old. Bothe male and females from primary and secondary care settings.
- Exclusion Criteria: Records with missing or incomplete information will be excluded. Age group below 20 Pregnancy patients
Data Collection
- Data Sources: Prescription records, medical charts, and electronic health records (EHRs) will be the primary sources of data.
- Data Collection Process: Trained research assistants will review and extract relevant data from the selected records.
- Data Variables: Data variables will include primary care and secondary with relevant inpatient and outpatient data and their respective antibiotic type.
Data Analysis
- WHO Indicators: The following WHO indicators will be applied: Percentage of Prescriptions with Antibiotics (PPA) for each healthcare setting.
- Comparative Analysis: Calculating the percentage of the inpatient and out patients data of prescribed antibiotics.
- Statistical Analysis: Antibiotic prescription patterns in primary and secondary care settings will be compared using appropriate statistical tests using the chi-square test is an inferential statistics.
- Ethical Considerations: Data will be anonymized and kept confidential to protect patient privacy.
Study Procedure
- Our study was an observational case control study conducted in the primary and secondary care setting of multi-specialty hospitals. Patients admitted between 23rd September 2022 to 1st March 2023.
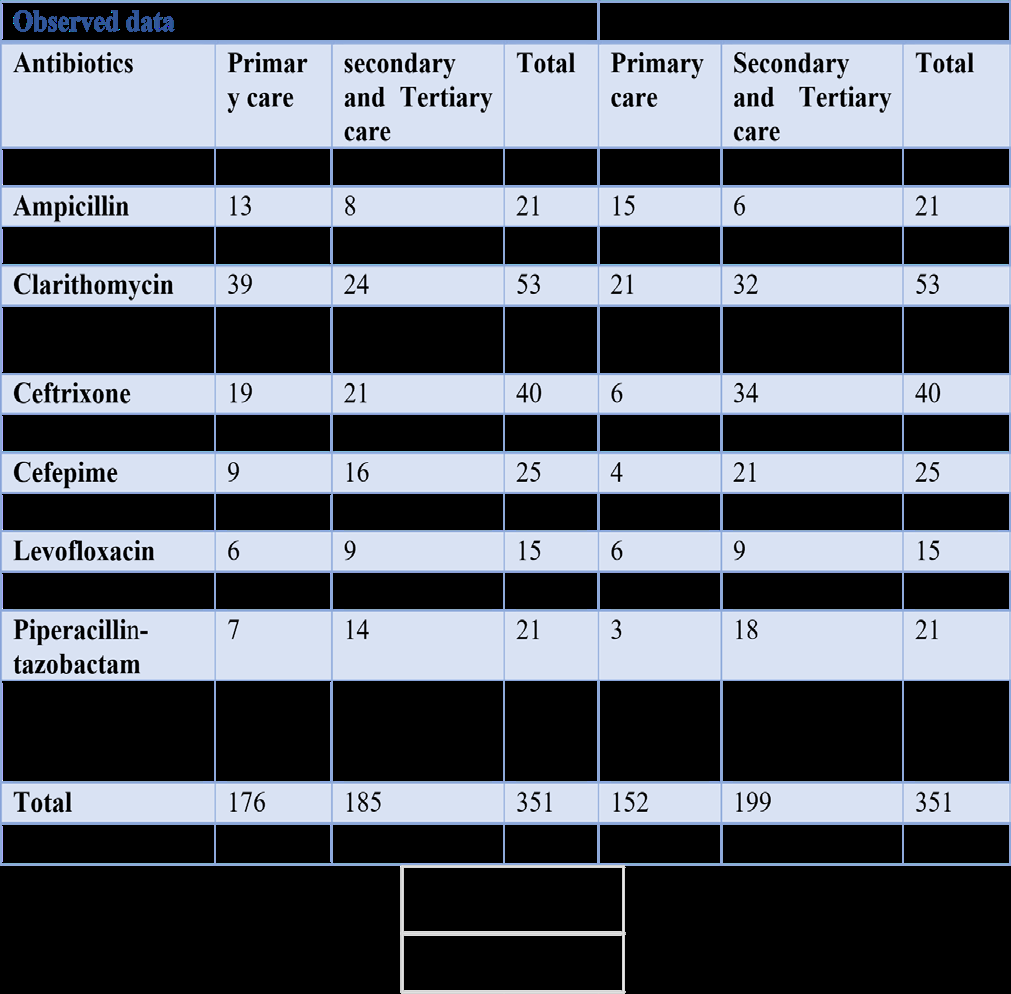
- A total no of 351 patients were included and studied in which 176 patients from primary care setting and
- 185 patients from primary, secondary and tertiary care setting with their respective prescribed antibiotics.
- An Inferential statistical analysis are done based on the observed data on a variables with the control data of WHO indicators (Table 1).
- Results
- Comparative Analysis
- As we conducted a study on the usage of prescribed antibiotics in both inpatients and outpatients and the percentage calculated by using:
- Percentage of antibiotics = (value / total value) × 100%
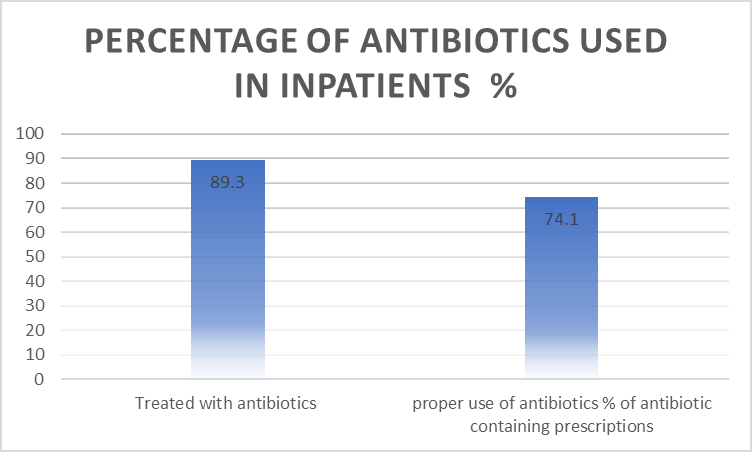
- Percentage of Antibiotics used in Inpatients
- CRETERIA
- %
- Treated with antibiotics
- 89 proper use of antibiotics % of antibiotic containing prescriptions
- 74
Table 1: Percentage of antibiotics used in inpatients.
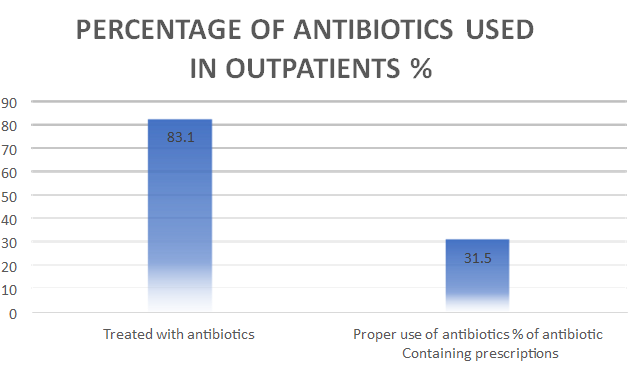
Outpatients
Based on the analysis of antibiotic usage among outpatients: • Approximately 83.1% of outpatients received antibiotic treatment.
• However, the adherence to proper use criteria for antibiotics among outpatients was notably lower, with only 31.5% of antibiotic-containing prescriptions meeting the criteria.
- Percentage of Antibiotics used in outpatients
- CRETERIA
- %
- Treated with antibiotics
- 83 proper use of antibiotics % of antibiotic containing prescriptions
- 32
Table 2: Percentage of antibiotics used in outpatients.
This data suggests a concerning gap in the appropriate use of antibiotics in the outpatient setting. There is a substantial need for interventions and initiatives aimed at improving antibiotic prescribing practices for outpatients to ensure the responsible and effective use of antibiotics and mitigate the risks associated with antibiotic resistance (Figure 8).
Statistical Analysis
Chi Square Test:
A p-value of 6.4E-25 is an extremely small p-value in the context of a statistical test, such as a chi-square test. This value represents a highly significant result (Figure 9).
In hypothesis testing, you compare the p-value to a significance level (alpha) to determine whether to reject the null hypothesis. If the p-value is smaller than alpha (commonly set at 0.05), you would typically reject the null hypothesis in favor of an alternative hypothesis.
With a p-value of 6.4E-25, it is safe to say that the result is statistically significant at even the most stringent significance levels. It indicates strong evidence against the null hypothesis, suggesting that there is likely a significant difference or association in the data being tested.
In statistical hypothesis testing, a “highly significant result” refers to a situation where the p-value associated with a statistical test is extremely small. The p-value is a measure that quantifies the strength of evidence against the null hypothesis.
When a p-value is very small (typically much smaller than the chosen significance level, such as 0.05), it indicates strong evidence against the null hypothesis. In practical terms, a highly significant result suggests that the observed data is very unlikely to have occurred by random chance under the assumptions of the null hypothesis (Figures 10-13).
Conclusion
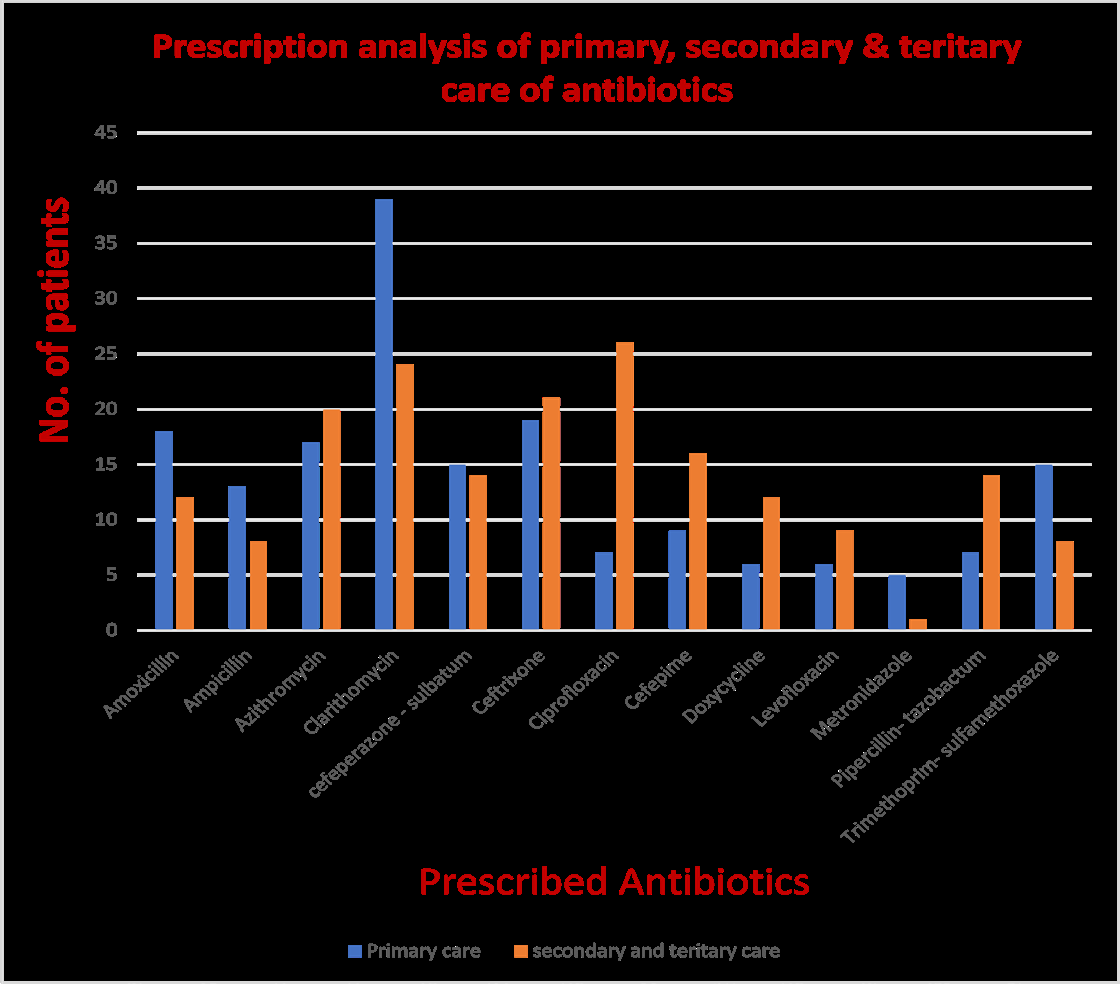
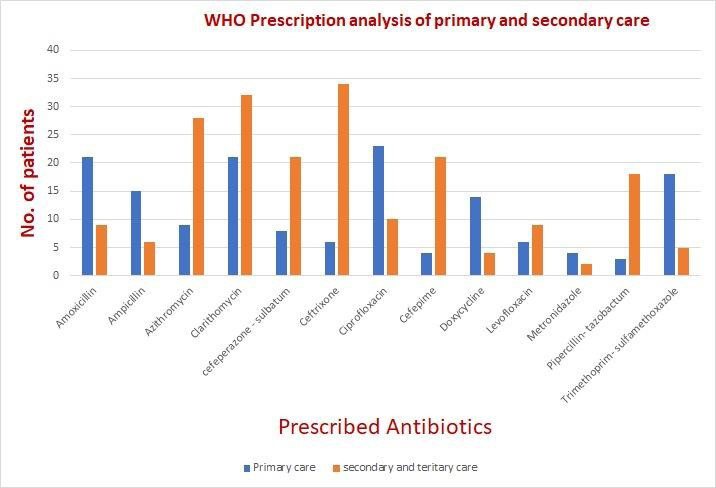
A p-value of 6.4E-25 is an extremely small p-value in the context of a statistical test, such as a chi square test. This value represents a highly significant result. It means significant variation in the prescription pattern of antibiotics in primary, secondary and tertiary care. The study reveals that the assessment of prescription patterns of antibiotics in primary and secondary care settings using WHO indicators has provided valuable insights into the current state of antibiotic utilization. This observational study has shed light on several critical aspects of antibiotic prescribing practices, revealing both strengths and areas for improvement within the healthcare system. One notable finding of this study is the frequent use of antibiotics in both primary and secondary care, highlighting the widespread reliance on these drugs in clinical practice. While antibiotics are essential tools in combating bacterial infections, their overuse and inappropriate prescribing have raised concerns regarding antibiotic resistance, adverse effects, and escalating healthcare costs. The WHO indicators have allowed us to quantitatively assess these issues and identify potential areas for intervention.
Another significant observation is the variation in antibiotic prescribing patterns between primary and secondary care facilities. This disparity suggests the need for targeted interventions and guidelines that address the specific challenges and complexities faced by different healthcare settings. Improving antibiotic stewardship programs and raising awareness among healthcare professionals regarding responsible antibiotic use can play a pivotal role in reducing inappropriate prescriptions.
Furthermore, this study has highlighted the importance of continuous monitoring and evaluation of antibiotic prescribing practices to ensure that interventions are effective and sustainable. By adhering to the WHO indicators and regularly assessing prescription patterns, healthcare systems can track progress over time and implement evidence-based strategies to enhance antibiotic utilization.
In conclusion, the assessment of prescription patterns of antibiotics in primary and secondary care settings using WHO indicators is a vital step toward promoting responsible antibiotic use, mitigating antibiotic resistance, and improving patient outcomes. It underscores the urgency of addressing the challenges posed by antibiotic overuse and provides a roadmap for optimizing antibiotic prescribing practices in healthcare. Moving forward, concerted efforts from healthcare providers, policymakers, and researchers are essential to implement meaningful changes that will safeguard the effectiveness of antibiotics for future generations.
References
-
Sulis G, Adam P, Nafade V, Gore G, Daniels B, et al. (2020) Antibiotic prescription practices in primary care in low- and middle-income countries: A systematic review and meta-analysis. PLoS medicine 17(6): e1003139.
-
Thomson K, Berry R, Robinson T, Brown H, Bambra C, et al. (2020) An examination of trends in antibiotic prescribing in primary care and the association with area-level deprivation in England. BMC Public Health 20: 1148.
-
Saha SK, Hawes L, Mazza D (2019) Effectiveness of interventions involving pharmacists on antibiotic prescribing by general practitioners: a systematic review and meta-analysis. Journal of Antimicrobial Chemotherapy 74( 5): 1173-1181.
-
Kumar A, Jain P, Upadhyaya P, Jain S (2014) A study monitoring prescription pattern of antibiotics in a tertiary care hospital in North India. Int J Basic Clin Pharmacol 3(6): 1006-1011.
-
Ajitha S, Shweta O (2016) Assessment of drug prescription pattern in children: A descriptive study. National Journal of Physiology, Pharmacy and Pharmacology 6(1): 74-80.
-
Olayemi SO, Akinyede AA, Oreagba AI (2006) Prescription pattern at primary health care centres in Lagos State. The Nigerian postgraduate medical journal 13(3): 220- 224.
-
Kumar JD, Rizwan M, Kothiyal P, Joshi Y (2017) Evaluation of prescription pattern of antibiotics for surgical prophylaxis in secondary care hospital. Int J Basic Clin Pharmacol 6(8): 1969-1976.
-
Albuhairi S, Farhan MA, Alanazi S, Althaqib A, Albeladi K, et al. (2021) Antibiotic Prescribing Patterns for Hospitalized children with Community-Acquired Pneumonia in a Secondary Care Center. Journal of Infection and Public Health 14(8): 1035-1041.
-
Akande TM, Ologe M, Medubi GF (2009) Antibiotic prescription pattern and cost at University of Ilorin teaching hospital, Ilorin, Nigeria. International Journal of Tropical Medicine 4(2): 50-54.
-
Auta A, Hadi MA, Oga E, Adewuyi EO, Abdu-Aguye SN, et al. (2019) Global access to antibiotics without prescription in community pharmacies: a systematic review and meta-analysis. Journal of Infection 78(1): 8-18.
-
Rossignoli A, Clavenna A, Bonati M (2007) Antibiotic prescription and prevalence rate in the outpatient paediatric population: analysis of surveys published during 2000–2005. Eur J Clin Pharmacol 63(12): 1099- 1106.
-
Pulia M, Kern M, Schwei RJ, Shah MN, Sampene E, et al. (2018) Comparing appropriateness of antibiotics for nursing home residents by setting of prescription initiation: a cross-sectional analysis. Antimicrob Resist Infect Control 7: 74.
-
Holstiege J, Schulz M, Akmatov MK, Kern WV, Steffen A, et al. (2020) The Decline in Outpatient Antibiotic Use. Deutsches Arzteblatt international 117(41): 679-686.
-
Demoz GT, Kasahun GG, Hagazy K, Woldu G, Wahdey S, et al. (2020) Prescribing Pattern of Antibiotics Using WHO Prescribing Indicators Among Inpatients in Ethiopia: A Need for Antibiotic Stewardship Program. Infection and drug resistance 13: 2783-2794.
-
Priyadharsini RP, Ramasamy K, Amarendar S (2022) Antibiotic-prescribing pattern in the outpatient departments using the WHO prescribing indicators and AWaRe assessment tool in a tertiary-care hospital in South India. Journal of family medicine and primary care 11(1): 74-78.
-
Kaur A, Bhagat R, Kaur N, Shafiq N, Gautam V, et al. (2018) A study of antibiotic prescription pattern in patients referred to tertiary care center in Northern India. Therapeutic advances in infectious disease 5(4): 63-68.
-
Boeckel TPV, Gandra S, Ashok A, Caudron Q, Grenfell BT, et al. (2014) Simon A Levin, Ramanan Laxminarayan, Global antibiotic consumption 2000 to 2010: an analysis of national pharmaceutical sales data. The Lancet Infectious Diseases 14(8): 742-750.
-
Laxminarayan R, Duse A, Wattal C, Zaidi AKM, Wertheim HFL, et al. (2013) Antibiotic resistance—the need for global solutions. Lancet Infectious Diseases 13(12): 1057-1098.
-
Augustin J, Mangiapane S, Kern WV ((2015) A regional analysis of outpatient antibiotic prescribing in Germany in 2010. The European Journal of Public Health 25(3): 397-399.
-
Hicks LA, Bartoces MG, Roberts RM, Suda KJ, Hunkler RJ, et al. (2015) US outpatient antibiotic prescribing variation according to geography, patient population, and provider specialty in 2011. Clinical Infectious Diseases 60(9): 1308-1316.
-
King LM, Bartoces M, Fleming-Dutra KE, Roberts RM, Hicks LA (2020) Changes in US outpatient antibiotic prescriptions from 2011–2016. Clinical Infectious Diseases 70(3): 370-377.
-
Deresinski S (2018) Inappropriate Outpatient Antibiotic Prescribing: The Need to Target Urgent Care Centers. Internal Medicine Alert 40(18).
-
Davey P, Brown E, Charani E, Fenelon L, Gould IM, et al. (2013) Interventions to improve antibiotic prescribing practices for hospital inpatients. Cochrane database of systematic reviews (4).
-
Livorsi D, Comer A, Matthias MS, Perencevich EN, Bair MJ (2015) Factors influencing antibiotic-prescribing decisions among inpatient physicians: a qualitative investigation. Infection Control & Hospital Epidemiology 36(9): 1065-1072.
-
Nabovati E, TaherZadeh Z, Eslami S, Abu-Hanna A, Abbasi R (2021) Antibiotic prescribing in inpatient and outpatient settings in Iran: a systematic review and meta-analysis study. Antimicrobial Resistance & Infection Control 10(1): 1-15.
-
Scarpato SJ, Timko DR, Cluzet VC, Dougherty JP, Nunez JJ, et al. (2017) An evaluation of antibiotic prescribing practices upon hospital discharge. Infection Control & Hospital Epidemiology 38(3): 353-355.
-
Remesh A, Salim S, Gayathri AM, Nair U, Retnavally KG (2013). Antibiotics prescribing pattern in the in-patient departments of a tertiary care hospital. Arch Pharm Pract 4(2): 71-76.
-
Yogo N, Haas MK, Knepper BC, Burman WJ, Mehler PS, et al. (2015) Antibiotic prescribing at the transition from hospitalization to discharge: a target for antibiotic stewardship. Infection Control & Hospital Epidemiology 36(4): 474-478.
-
Labi AK, Obeng-Nkrumah N, Sunkwa-Mills G, Bediako- Bowan A, Akufo C, et al. (2018) Antibiotic prescribing in paediatric inpatients in Ghana: a multi-centre point prevalence survey. BMC pediatrics 18(1): 391.
-
Kumar R, Indira K, Rizvi A, Rizvi T, Jeyaseelan L (2008) Antibiotic prescribing practices in primary and secondary health care facilities in Uttar Pradesh, India. Journal of clinical pharmacy and therapeutics 33(6): 625-634.
-
Ashiru-Oredope D, Budd EL, Bhattacharya A, Din N, McNulty CAM, et al. (2016) Implementation of antimicrobial stewardship interventions recommended by national toolkits in primary and secondary healthcare sectors in England: TARGET and Start Smart Then Focus. Journal of Antimicrobial Chemotherapy 71(5): 1408- 1414.
-
Curtis C, Marriott J (2008) Is there an association between referral population deprivation and antibiotic prescribing in primary and secondary care. International Journal of Pharmacy Practice 16(4): 217-222.
-
Tarrant C, Krockow EM, Nakkawita WD, Bolscher M, Colman AM, et al. (2020) Moral and contextual dimensions of inappropriate antibiotic prescribing in secondary care: a three-country interview study. Frontiers in Sociology 5: 7.
-
Tonna AP, Stewart D, West B, Gould I, McCaig D (2008) Antimicrobial optimisation in secondary care: the pharmacist as part of a multidisciplinary antimicrobial programme—a literature review. International journal of antimicrobial agents 31(6): 511-517.
-
Aldeyab MA, Harbarth S, Vernaz N, Kearney MP, Scott MG, et al. (2012) The impact of antibiotic use on the incidence and resistance pattern of extended‐spectrum beta‐lactamase‐producing bacteria in primary and secondary healthcare settings. British journal of clinical pharmacology 74(1): 171-179.
-
Adekanmbi V, Jones H, Farewell D, Francis NA (2020) Antibiotic use and deprivation: an analysis of Welsh primary care antibiotic prescribing data by socioeconomic status. Journal of Antimicrobial Chemotherapy 75(8): 2363-2371.
-
Devine P, Kane MO, Bucholc M (2021) Trends, variation, and factors influencing antibiotic prescribing: a longitudinal study in primary care using a multilevel modelling approach. Antibiotics 11(1): 17.
-
Hay AD (2019) Antibiotic prescribing in primary care. BMJ pp: 364.
-
Ashiru-Oredope D, Sharland M, Charani E, McNulty C, Cooke J (2012) Improving the quality of antibiotic prescribing in the NHS by developing a new Antimicrobial Stewardship Programme: Start Smart—Then Focus. Journal of antimicrobial chemotherapy 67(1): 51-63.
-
Krockow EM, Harvey EJ, Ashiru-Oredope D (2022) Addressing long-term and repeat antibiotic prescriptions in primary care: considerations for a behavioural approach. BMJ Quality Safety 31(11): 782-786.
-
Shively NR, Buehrle DJ, Clancy CJ, Decker BK (2018) Prevalence of inappropriate antibiotic prescribing in primary care clinics within a veterans affairs health care system. Antimicrobial agents and chemotherapy 62(8): e00337-18.
-
Parveen Z, Gupta S, Kumar D, Hussain S (2016) Drug utilization pattern using WHO prescribing, patient care and health facility indicators in a primary and secondary health care facility. National Journal of Physiology, Pharmacy and Pharmacology 6(3): 182-186.
-
Kotwani A, Chaudhury RR, Holloway K (2012) Antibiotic- prescribing practices of primary care prescribers for acute diarrhea in New Delhi, India. Value in health 15(1): S116-S119.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda