Exploratory Factorial Model of Work Commitment in the COVID-19 Era
Labor commitment is an observable process in crisis or labor instability. Since the structure of work commitment obeys a series of observable dimensions in the pandemic, the objective was to demonstrate its structure of mediating relationships. For this purpose, an exploratory, cross-sectional and psychometric work was carried out with a sample of 100 students. Once the factorial structure had been explored, a second study was carried out to confirm the structure with another sample of students. The selection criteria were related to inclusion in professional practices and social service in community centers. The results show that the adjustment and residual parameters suggest the non-rejection of the null hypothesis regarding the significant differences between the theoretical structure and the empirical observations. In relation to the paradigms, the relevance of extending the model in order to predict job performance is assumed.
Introduction
The COVID-19 pandemic strained labor relations to the point where health professionals were exposed to forced labor to reduce the number of intubated patients and guarantee the greatest possible availability [1]. In this sense, work commitment has been observed as an emerging variable in risk situations. In fact, the differences between health professionals are explained by the degree of exposure to risk.
The sociocultural approach indicates that values, norms and beliefs coexist and prevail among health professionals that generate significant observable differences in service quality indicators [2]. The values considered as principles that guide decisions and behavior are factors that foster a propensity for risk or high commitment to the profession or vocation.
However, the socioeconomic perspective has advanced towards the prediction of commitment, decision-making and behavior in risk scenarios [3]. While the work culture demands a climate of relationships, tasks and innovations in stable situations, socioeconomic theory has discovered that greater risk increases work commitment. In this sense, the factors of income, compensation, stimuli and benefits configure a system of extrinsic motivation that anticipates a propensity for risk.
Both risk and stability scenarios often converge in a sustainable system in finance [4]. The socio-psychological approach of perceptions, motivations, dispositions and intentions explains the risks and stabilities of a system that is neither sustainable nor bankable. This is the case of the health system that increased its hospitalization in the pandemic with limited financial and human capital. Work commitment observable in these systems and situations is distinguished by intrinsic motivation. That is, health professionals are exposed to risks for personal reasons rather than economic or cultural ones.
The origins of this intrinsic commitment are found in the organizational culture [5]. Even the intrinsic commitment alludes to an educational part because it derives from an academic legacy. In this way, the history of the health professions is littered with principles that guide the ethics and conduct of professionals. Another origin is found in family history. The socio-educational theory indicates that human capital is inherited. In this sense, if an ancestor instructed the talent, then the health professional will act in accordance with his family legacy.
The intrinsic commitment is also observed in the leadership exercised by the health professional in a union, organization, sector or team [6]. The hegemony of a knowledge or skill, transferred in professional practice, also suggests a scenario in which commitment emerges as a distinctive feature of collaborative work. In fact, this type of introspective commitment is combined with extrinsic motivation consisting of prizes and rewards for high performance or work efficiency.
However, the intrinsic commitment is appreciated in a risk scenario such as the pandemic [7]. Faced with the stigma towards health professionals that emerged after the increase in deaths from COVID-19, work commitment was replacing prejudice with recognition of health work. In this way, the balance of cases of contagion, disease and death can be explained by immunization, but also by intrinsic commitment.
Although intrinsic commitment has been identified as a job performance factor, the determinants have not been revealed [8]. Institutional leadership, understood as the influence of the State on the health sector, influences decisions and actions imposed by a vertical chain of command. The autocratic system explains the behavior of health professionals based on a guideline to the epidemic traffic light. Non-alignment to the institutional mandate implies a position of labor responsibility.
Institutional leadership is supported by the care climate in order to reinforce the institutional guidelines for social distancing [9]. Although the traffic light indicates a restriction or clearance of areas and resources, the welfare climate refers to a policy of openness to those who request public service. As institutional leadership and the care climate intensify, job satisfaction emerges. The demand for anti-COVID-19 tests, intubation and consultations means exhaustion due to overtime. In this risk scenario, institutional leadership relies on the healthcare environment to guide motivation towards those who are satisfied with their performance in the health crisis. In this way, the system of recognitions, stimuli and rewards are configured isomorphically.
Isomorphism alludes to the coupling between health professionals [10]. At the beginning of the pandemic, the lack of anti-COVID-19 devices such as masks led to a coupling of those who transport the infected, those who receive and care for them without due protection. The coupling between professions supposes additional training. Doctors who had to carry out transfer tasks, paramedics who had to supply oxygen to vulnerable groups or nurses who had to care for terminal cases indicate care-oriented training.
However, the exposed variables are insufficient without the family legacy from which the intrinsic commitment feeds [11]. The formation of human capital suggests that prior to entering the university, the future professional was influenced by a close relative. The family legacy materializes in medical, paramedical or psychological knowledge that defines exposure to risk. In addition to this process, intrinsic motivation or risk exposure decision for family or personal reasons, complement the structure of work commitment.
The seven variables exposed have been appreciated as determinants of labor collaboration in exceptional situations. The increase in institutional leadership, the care climate, job satisfaction and isomorphism.
Method
A cross-sectional, correlational and psychometric study was carried out with a sample of 100 students (M = 24.1 SD = 2.3 age and M = 8’906.00 SD = 453.45 monthly income) from a public university in central Mexico.
The determinants of commitment were measured with the Multifactorial Scale of Work Commitment [12]. The scale includes seven dimensions related to institutional leadership (“Management of COVID-19 requires strict commitment”), Care environment (“Caring for COVID-19 requires exceptional commitment”), Job satisfaction (“COVID-19 is an opportunity for personal growth”), Labor isomorphism (“The epidemiological traffic light will guide our efforts in the face of COVID-19”), Supplementary training (“COVID-19 will require learning preventive skills”), Family Legacy (“COVID-19 is an exceptional challenge that requires a supportive response”), Intrinsic motivation (“The recognition of those who overcome COVID-19 is what the pandemic leaves me”) and Collaboration (“I promote the use of anti-COVID-19 devices to attend a number greater than cases”). Each item includes five response options ranging from 0 = “not at all agree” to 5 = “quite agree”.
The psychometric properties of the instrument indicate a reliability ranging from .762 to .784 for the general scale and from .745 to .779 for the other subscales. The adequacy and sphericity suggest the validity that includes factorial weights which range from .465 to .672 Respondents were contacted through institutional mail indicating that they will not receive any payment for their responses, although confidentiality and anonymity are guaranteed. The guidelines of the American Psychological Association for studies with people in stressful situations were followed. The purpose of the study and those responsible for it were reported. Once the confidentiality agreement was signed, the questionnaire was sent via email. The homogenization of the concepts was established with a focus group prior to the pilot survey.
The data were captured in Excel and processed in JASP version 14. Cronbach’s alpha was estimated for the consistency of the instrument and the Bartlett KMO test for the sphericity and adequacy of the instrument to the exploratory factor analysis of principal axes with promax rotation. In a second study, the structure of eight factors that explained 78% of the variance was confirmed with a sample of 86 students (M = 24.3 DE 2.3 age and M = 7’982.00 DE = 456.45 monthly income). The model of mediating factors was estimated using the fit and residual coefficients with the same version of the software used in the first study.
Results
Figure 1 shows the relationships between the established factors. It can be seen that the sum of the direct and indirect effects indicate spurious relationships between the determinants of collaborative commitment. It means then that the sample surveyed seems to reflect a commitment focused on collaboration, but without connection to the determinants reported in the literature. In fact, the only value that suggests a low relationship is that of isomorphism with collaboration. In other words, the pandemic reduced to a minimum the commitment originated by the union, the academy or the organization and the collaborative commitment. In this sense, a consequence of the pandemic in the workplace is the reduction of work commitment. In its intrinsic dimension, work commitment supposes a disinterested response from health professionals to the exceptional situation.
However, work commitment is a complex process of extrinsic and intrinsic motivation. Due to such a structure, work commitment is affected by the health crisis in its intrinsic dimension more than in its extrinsic dimension. In the case of professional practices and social service, work commitment is an added value of the academy that was affected by COVID-19.
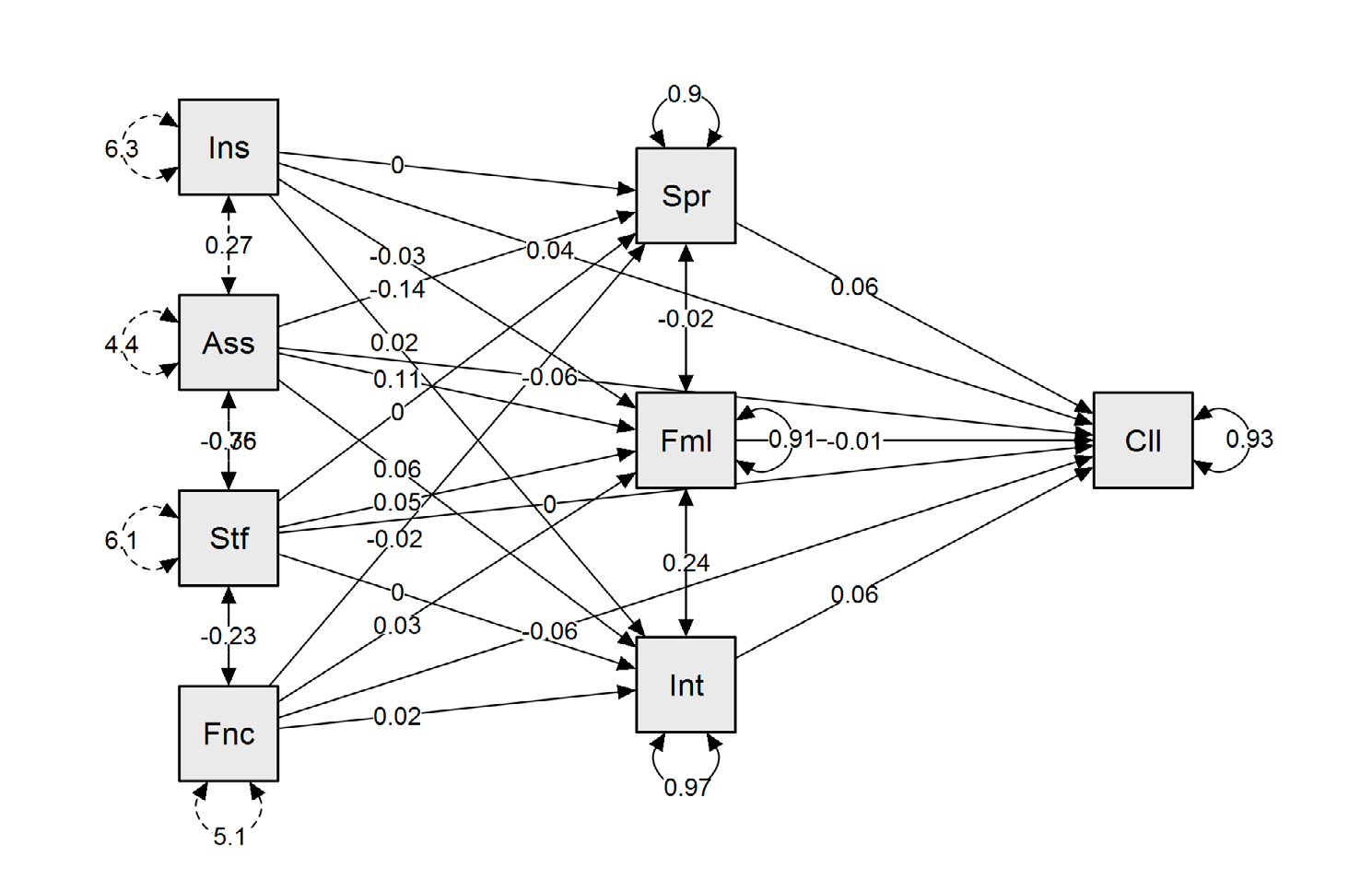
Ins = Institutional leadership, Ass = Care climate, Stf = Job satisfaction, Fnc = Job isomorphism, Spr = Additional training, Fml = Family Legacy, Int = Intrinsic motivation, Cii = Collaboration. Source Prepared with study data. Multivariate = 7,272; Bootstrap = .000; Alpha = .673; KMO = .875; X2 = 12,156; 11gl
; _ p = .000; Normality (kurtosis = 7.272), reliability (alpha = .673) and validity (KMO = .875; X 2 = 12.156; 11gl; p = .000) (β = .91) (GFI = .975; NFI = .975 , CFI = .985, RMSEA = .009).
The fit and residual parameters suggest non-rejection of the null hypothesis regarding the significant differences between the structure reported in the literature with respect to the observed reading. In other words, the work commitment reported in the literature indicates that the determinant of collaboration is intrinsic motivation, although in the present work the isomorphism had a greater impact on collaboration.
Discussion
The contribution of this work to the state of the art lies in the contrast of a factorial model of mediation where isomorphism affected collaboration. That is, the work commitment is anticipated by the asymmetric relations between management and students [13]. Labor isomorphism has been related to collaborative work in situations of stability, but in the present work a direct relationship was found between both variables.
Relative to studies that explain collaborative work with respect to sociocultural variables such as values, beliefs, and norms, the present study indicates that isomorphic beliefs explain collaborative engagement. The values or principles that guide decisions and behaviors, as well as the beliefs or surrounding information in socio-digital networks have been identified as determinants of collaboration [14]. It is recommended to extend the study towards sociocultural variables in order to predict behavior in risk scenarios.
The socioeconomic approach that alludes to extrinsic motivation as a dimension of work commitment indicates that greater compensation produces maximum dedication, even when the work involves exposure to significant risks [15]. In the present study, intrinsic motivation was associated with family legacy, but both variables do not explain collaboration. This finding makes it possible to establish that extrinsic motivation does not reflect work commitment in the sample.
Regarding the socio-educational perspective, where labor skills and supplementary training are predictors of collaboration, the present study indicates that both variables were decreased by the pandemic. In the case of additional training, the skills acquired during the pandemic indicate a scenario that inhibited the formation of human capital [16]. It is advisable to include the factor related to performance in the model in order to be able to identify the degree of impact of the pandemic where commitment is a mediating factor.
Conclusion
The objective of the study consisted in the demonstration of a factorial model of mediating relationships between the determinants of collaborative commitment. The results indicate that the relationships between the dimensions are significant so as not to reject the hypothesis of significant differences between the structures reported in the literature with respect to the structure observed in the present work. In relation to the sociocultural, socioeconomic and socio- educational frameworks that highlight determinants of collaborative commitment, the present study corroborates relationships that indicate a reduction in these dimensions due to the pandemic.
References
-
Carreón Guillén J, Bustos Aguayo J, Sánchez Sánchez A, Martínez Muñoz E, García Lirios C (2020) The structure of work stress. Borderless Academic Research Journal: Division of Economic and Social Sciences (32): 1-23.
-
Garcia Lirios C (2021) Occupational risk perceptions in the Post Covid-19 era. Know and Share Psychology 2(1).
-
Sánchez-Sánchez A, Bustos Aguayo JM, Hernández Vádés J, Carreón Guillén J, Martínez Muñoz E, et al. (2020) Factorial structure of the determinants of organizational bullying. Hispanic American Psychology Notebooks 18(1).
-
Athar HS (2020) The influence of organizational culture on organizational commitment post pandemic Covid-19. International Journal of Multicultural and Multireligious Understanding 7(5): 148-157.
-
Chanana N (2021) The impact of COVID‐19 pandemic on employees organizational commitment and job satisfaction in reference to gender differences. Journal of Public Affairs 21(4): e2695.
-
Chauhan RS, Howe DC, Nachmias S (2022) Organizational commitment: an ever-shifting concept forever changed by COVID-19. Human Resource Development International 26(2): 232-239.
-
Sokal L, Trudel LE, Babb J (2021) I’ve had it! Factors associated with burnout and low organizational commitment in Canadian teachers during the second wave of the COVID-19 pandemic. International Journal of Educational Research Open 2: 100023.
-
Li Z, Akouatcha HG, Akram U, Anaba OA (2021) Information and communication technology and organizational performance during the COVID-19 pandemic: the role of organizational commitment, growth mindset, and entrepreneurial orientation. Frontiers in Psychology 12: 752193.
-
Su L, Wichaikhum OA, Abhicharttibutra K (2023) Predictors of organizational commitment among Chinese nurses during the COVID‐19 pandemic. International Nursing Review 70(1): 111-116.
-
Son HS, Kim K, Cho IK, Lee J, Choi JM, et al. (2022) Healthcare Workers’ Resilience Mediates the Influence of Organizational Commitment and Anxiety Response to Viral Epidemic on Their Quality of Life in the COVID-19 Pandemic. Frontiers in Psychiatry 12: 2409.
-
Prasetyo YT, Montenegro LD, Nadlifatin R, Kurata YB, Ong AKS, et al. (2022) The influence of organizational commitment on the perceived effectiveness of virtual meetings by Filipino professionals during the COVID-19 pandemic: A structural equation modeling approach. Work 71(1): 19-29.
-
Aminizadeh M, Saberinia A, Salahi S, Sarhadi M, Jangipour Afshar P, et al. (2022) Quality of working life and organizational commitment of Iranian pre- hospital paramedic employees during the 2019 novel coronavirus outbreak. International Journal of Healthcare Management 15(1): 36-44.
-
Boonsiritomachai W, Sud-On P (2022) The moderation effect of work engagement on entrepreneurial attitude and organizational commitment: evidence from Thailand’s entry-level employees during the COVID-19 pandemic. Asia-Pacific Journal of Business Administration 14(1): 50-71.
-
Ingsih K, Suhana S, Ali S (2021) Transformational leadership style and organizational commitment in pandemic Covid-19. Accounting and Administration 66(5): 12.
-
To WM, Huang G (2022) Effects of equity, perceived organizational support and job satisfaction on organizational commitment in Macao’s gaming industry. Management Decision.
-
Faramawy MAEA, Abd El Kader AI (2022) COVID-19 anxiety and organizational commitment among front- line nurses: Perceived role of nurse managers’ caring behavior. Nursing Practice Today 9(1): 37-45.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda