Infection Prevention Control: First Cycle Audit Regarding Safe Fitting and Removal of Personal Protective Equipment among Health-Care Workers in Infectious Diseases Wards at Soba University Hospital
In the recent years the frequency of health emergences increased highlighted the importance of infection prevention control (IPC) measures especially personal protective equipment (PPE). This study assessed the compliance of the healthcare providers at Soba university hospital to IPCPPE and assessed the effectiveness of the IPC training center at the hospital. This descriptive cross-sectional, hospital-based study, used self-administered questionnaire to gather the data, and statistical program for social science (SPSS) version 28 to analyze it, frequency tables were used to show the results. The overall knowledge of healthcare providers was good, but only 69.6% agreed that they changed gloves between patients. They mentioned reasons for their poor adherence to PPE: PPE interference with work (69.6%), brought discomfort to the patient (50%), brought discomfort to them (47.8%). This result dictated the effectiveness of theoretical part of the training while the practical and supervision section needs improvement.
Introduction
Infection prevention and control is a practical, evidence- based approach preventing patients and health workers from being harmed by avoidable infections [1].
Personal protective equipment (PPE), as defined by the Occupational Safety and Health Administration (OSHA), is “specialized clothing or equipment, worn by an employee for protection against infectious materials”[2, 3], in the last decades the frequency of health emergences increased highlighted the importance of IPC measures especially PPE [4].
OSHA issued regulations for workplace health and safety, which requires use of PPE in healthcare settings to protect healthcare providers from exposure to blood borne pathogens and Mycobacterium tuberculosis. However, under OSHA’s General Duty Clause PPE is required for any potential infectious disease exposure. Employers must provide their employees with appropriate PPE and ensure that PPE is disposed or, if reusable, that it is properly cleaned or laundered, repaired and stored after use [2].
PPE includes gloves, medical/surgical face masks - thereafter referred as “medical masks”, goggles, face shield, and gowns, as well as items for specific procedures filtering face piece respirators (i.e. N95 or FFP2 or FFP3 standard or equivalent) - thereafter referred to as “respirators” - and aprons [5]. Hand hygiene should be performed immediately after removal of PPE [6].
Commonest reported PPE adherence defects related to improper hand hygiene and mask removal [7, 8, 9, 10], Other factors are a clear understanding of the guidelines, positive role of supervisors, communication about guidelines, sufficient resources, the perceived value of following guidance, the comfort of personal protective equipment (PPE), and availability of resources [11, 12, 13, 14, 15].
This study assessed the compliance of the healthcare providers at Soba university hospital to IPC\PPE and assessed the effectiveness of the IPC training center at the hospital.
Material and Methods
Study Design
A cross-sectional hospital-based study was conducted at Soba Teaching Hospital in Khartoum, Sudan, to assess the efficiency of Infection Prevention Control (IPC) Training among healthcare workers at Soba University Teaching Hospital. The study was the first cycle of a clinical audit. The guidelines on standard of IPC/ PPE usage, developed by Federal Ministry of Health, SD and Standard of IPC policy of the Hospital were used as references.
Study Population
The population of the present study includes healthcare workers who had direct contact with patients with potentially infectious diseases “Number 46”.
Study Area
Soba University Hospital is a Teaching Hospital belongs to University of Khartoum, consists of different departments and education and research centers. One of the centers is IPC training center in which regular training about IPC measures for the healthcare workers is held.
The first phase was observation of confirmed cases of COVID-19 among those who worked in contact with Confirmed and Suspected cases of COVID-19, despite the availability of Personal Protective Equipment, and the existence of IPC training center at the hospital as well as the availability of regular training programs for the healthcare workers.
Then, a questionnaire was developed and data was collected from all healthcare workers working in contacts with cases of potentially infectious diseases.
Total coverage of healthcare providers who were working in the wards and units of infectious diseases was chosen as sampling technique. Healthcare providers who unwilling to participate were excluded. Because the working shifts in the hospital were distributed by days, all the available healthcare providers were covered during the data collection period.
The efficiency of the training center was assessed using questionnaire developed by the authors for the presence of the following items:
Data were collected using questionnaire, filled out by healthcare providers. Data were analyzed using SPSS 28 version. Descriptive statistics such as percentages and frequencies describing the practice of the healthcare providers were used, and the results were illustrated in forms of figures and tables.
Ethical approval was obtained from the Research and Training Administration at Soba University Teaching Hospital. Informed consent was taken from each healthcare worker.
Results
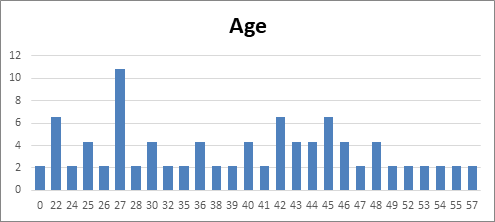
The Mean±SD (37±11.5) years
27 years had been the most frequent age among the healthcare providers in the study.
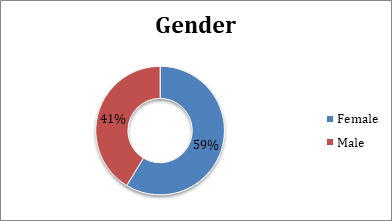
The majority of the healthcare providers were females this is matching with the recent study in medical sector statistics that concluded nearly two thirds of the medical staff in Sudan were females.
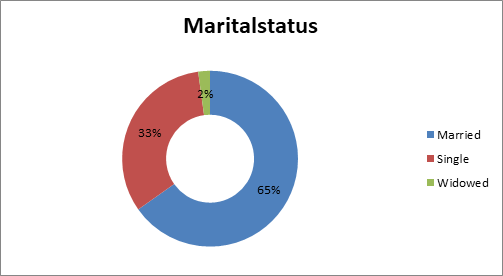
The majority (65%) were married.
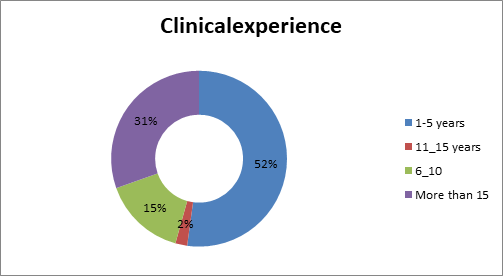
An appreciated percentage of the healthcare providers had experience of more than 15 years, 52% had experience (1-5) years.
| Frequency | Percentage | |
|---|---|---|
| Exposure to training | ||
| Yes | 26 | 56.50% |
| No | 20 | 43.50% |
| Exposure to guidelines | ||
| Yes | 21 | 45.70% |
| No | 25 | 54.30% |
| IPC policy of the hospital: | ||
| Yes | ||
| No | 39 | 84.80% |
| I do not know | 3 | 6.50% |
| 4 | 4.80% | |
| Supervisor criticism when not use proper precautions: | ||
| Yes | ||
| No | ||
| I do not know | 37 | 80.40% |
| 6 | 13% | |
| 3 | 6.50% | |
| Colleagues criticism when not use proper precautions: | ||
| Yes | ||
| No | ||
| I do not know | 32 | 69.60% |
| 11 | 23.90% | |
| 3 | 6.50% | |
| Availability of recommended PPE | ||
| Yes | ||
| No | 31 | 67.40% |
| I do not know | 12 | 26.10% |
| 3 | 6.50% |
Table 1: Exposure to PPE\IPC training and guides (n=46).
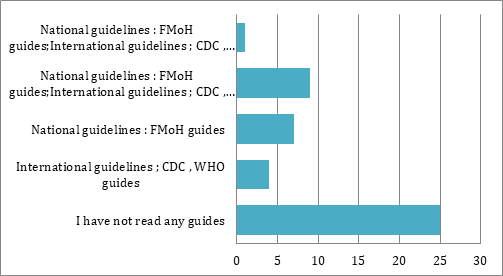
Only 45.7% of healthcare providers agreed that they read guides for safe donning and doffing of PPE
| Frequency | Percentage | |
|---|---|---|
| Knowledge of how to use PPE: | ||
| Yes | ||
| No | 44 | 95.70% |
| 2 | 4.30% | |
| PPE includes: | ||
| Face shield | 45 | 97.80% |
| Gowns | 45 | 97.80% |
| Goggles | 45 | 97.80% |
| Gloves | 45 | 97.80% |
| Aprons | 45 | 97.80% |
| Surgical mask | 46 | 100% |
| Surgical mask protective period\hours: | ||
| Less than 2 | ||
| 02-Apr | ||
| 05-Jun | 4 | 8.70% |
| 07-Oct | 32 | 69.60% |
| I do not know | 6 | 13% |
| 2 | 4.30% | |
| 2 | 4.30% | |
| Hand-washing is mandatory when manipulating PPE: | ||
| Yes | ||
| No | ||
| I do not know | 41 | 89.10% |
| 2 | 4.30% | |
| 3 | 6.50% | |
| Usage and elimination of PPE need hand hygiene; | ||
| Yes | ||
| No | ||
| 44 | 95.70% | |
| 2 | 4.30% | |
| Change PPE when get out and back again: | ||
| Yes | ||
| No | ||
| 44 | 95.70% | |
| 2 | 4.30% |
Table 2: Knowledge of healthcare providers regarding PPE\IPC (n=46).
| Frequency | Percentage | |
|---|---|---|
| Remove PPE immediately after end: | ||
| Yes | ||
| No | 44 | 95.70% |
| 2 | 4.30% | |
| Change gloves between patients; | ||
| Yes | ||
| No | 32 | 69.90% |
| I do not know | 11 | 23.90% |
| 3 | 6.50% | |
| Ability to wear and remove PPE: | ||
| Yes | ||
| No | 45 | 97.80% |
| 1 | 2.20% | |
| PPE interfere with your work: | ||
| Yes | ||
| No | 32 | 69.60% |
| I do not know | 10 | 21.70% |
| 4 | 8.70% | |
| Work with equipped PPE: | ||
| Yes | ||
| No | 43 | 93.40% |
| I do not know | 2 | 4.30% |
| 1 | 2.10% | |
| PPE brings discomfort to patient | ||
| Yes | ||
| No | 23 | 50% |
| I do not know | 22 | 47.80% |
| 1 | 2.20% | |
| Wearing PPE brings discomfort for you: | ||
| Yes | ||
| No | 22 | 47.80% |
| 24 | 52.20% |
Table 3: Healthcare providers practice regarding PPE\IPC (n=46).
Discussion
This study was cross-sectional, hospital-based study to assess the compliance of healthcare workers to IPC\PPE standards at Soba University Hospital, as well as to assess the efficiency of IPC training center at the hospital.
The healthcare workers in the study were ranged between 25.5 to 48.5 years and 59% of them were females, in contrary to Chinese study, where HCW age ranged from 25 to 33 and 76.3 were females Hu X, et al. Self-Reported Use of Personal Protective Equipment among Chinese Critical Care Clinicians during 2009 H1N1 Influenza Pandemic. PLoS ONE 7 [9]: e44723. doi:10.1371/journal.pone.0044723). One third of them had experience more than 15 years in clinical practice while 52% were less than 5 years’ experience, but different study found that 56.5% of the healthcare workers reported previous exposure to IPC\PPE training; Shigayeva, et al. found that recent infection prevention control training was a significant predictor of adherence to IPC measures [16]. Only 45.7% in our study reported exposure to IPC\PPE guidelines, three studies found that Knowledge of current guidelines was related to adherence to IPC measures [16, 17, 18, 19].
84.8% agreed that there is IPC policy at the hospital, in this study, 80.4% agreed upon supervisor role about their compliance to IPC\PPE practice at the hospital while only 69.5% agreed upon colleagues a positive role of their colleagues.
67.4% agreed that PPE were available, and this was the second unexpected result due to the availability of all recommended PPE.
97.8% named PPE components: face shield gowns, goggles, gloves, aprons, surgical mask. 69.6% agreed that protective period of surgical mask is 2-4 hours.
Healthcare workers mentioned some causes for their poor compliance: PPE interference with work (69.6%), brought discomfort to the patient (50%), brought discomfort to them (47.8%).
References
-
(2023) Infection prevention and control. World Health Organization.
-
(2023) Occupational Safety and Health Administration. Personal protective Equipment.
-
(2023) Personal Protective Equipment (PPE) World Health Organization.
-
Cittone GR (2023) Ciottone’s Disaster Medicine. In: 3rd (Edn.), Emergency Medicine.
-
Guidance for the use and selection of personal protective equipment in healthcare setting. CDC guidelines.
-
(2023) Personal Protective Equipment (PPE): Coaching and Training Frontline Health Care Professionals: CDC lecture.
-
Phan LT, Maita D, Mortiz DC, Weber R, Fritzen-Pedicini C, et al. (2019) Personal protective equipment doffing practices of healthcare workers. J Occup Environ Hyg 16(8): 575-581.
-
Mumma JM, Durso FT, Casanova LM, Erukunuakpor K, Kraft CS, et al. (2019) Common behaviors and faults when doffing personal protective equipment for patients with serious communicable diseases. Clin Infect Dis 69(3): S214-S220.
-
Okamoto K, Rhee Y, Schoeny M, Lolans K, Cheng J, et al. (2019) Impact of doffing errors on healthcare worker self-contamination when caring for patients on contact precautions. Infect Control Hosp Epidemiol 40(5): 559- 565.
-
Zhang H-L, Yang S, Luo H-X, You J-P (2021) The error-prone operational steps and key sites of self- contamination during donning and doffing of personal protective equipment by health care workers. Disaster Med Public Health Prep 16(6): 2486-2491.
-
(2021) Brooks SK, Greenberg N, Wessely S, Rubin GJ: Factors affecting healthcare workers’ compliance with social and behavioral infection control measures during emerging infectious disease outbreaks: rapid evidence review. BMJ Open 11(8): e049857.
-
Honda H, Iwata K (2016) Personal protective equipment and improving compliance among healthcare workers in high-risk settings. Curr Opin Infect Dis 29(4): 400-406.
-
Atkinson P, French J, Lang E, McColl T, Mazurik L (2020) Just the Facts: protecting frontline clinicians during the COVID-19 pandemic. CJEM 22(4): 435-439.
-
Wang J, Zhou M, Liu F (2020) Reasons for healthcare workers becoming infected with novel coronavirus disease 2019 (COVID-19) in China. J Hosp Infect 105(1): 100-101.
-
Cook TM (2020) Personal protective equipment during the coronavirus disease (COVID) 2019 pandemic - a narrative review. Anaesthesia 75(7): 920-927.
-
Okello TR, Kansime K, Odora J, Apio JA, Pecorella I (2017) Barriers and factors affecting personal protective equipment usage in St. Mary’s Hospital Lacor in Northern Uganda. East Cent African J Surg 22(1): 59-65.
-
Shigayeva A, Green K, Raboud JM, Henry B, Simor AE, et al. (2007) Factors associated with critical-care healthcare workers’ adherence to recommended barrier precautions during the Toronto severe acute respiratory syndrome outbreak. Infect Control Hosp Epidemiol 28(11): 1275-1283.
-
Yap J, Lee VJ, Yau TY, Pin Ng T, Tor P-C (2010) Knowledge, attitudes and practices towards pandemic influenza among cases, close contacts, and healthcare workers in tropical Singapore: a cross-sectional survey. BMC Public Health 10: 442.
-
Nour MO, Babalghith AO, Natto HA, Al-Amin FO, Alawneh SM (2015) Knowledge, attitude and practices of healthcare providers towards MERS-CoV infection at Makkah hospitals, KSA. Int Res J Med Med Sci 3(4): 103- 112.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda