Quality of Life in People Living With Chronic Kidney Disease and Renal Replacement Therapy
Chronic kidney disease is a pathology with fatal outcome in the short and medium term, affecting diverse body structures; it is directly associated with a reduced quality of life; given its irreversible nature, it generates a series of complicated conditions in matters of care and treatment, producing a negative impact on the patient’s quality of life, which implies changes in their lifestyle that have repercussions in the familial, work and social spheres. A proper assessment in quality of life makes it possible to estimate the impact that Chronic Kidney Disease represents in the daily life of people and the consequences it implies over their physical, emotional and social wellbeing; thus, it is fundamental to design effective interventions that guarantee integral health care measures according to the needs of each person. Objective: Evaluate the quality of life in people living with Chronic Kidney Disease undergoing Renal Replacement Therapy through hemodialysis in a second- level hospital in Tepic, Nayarit, Mexico in 2022. Methods and Materials: A descriptive, cross-sectional study with a quantitative approach and simple random sampling, the recollection of data were conducted using a scale to evaluate quality of life, with a Chronbach alfa of 0.86, a prior written informed consent was employed. The statistical analysis was conducted using descriptive and inferential statistics, a statistical significance value of p <0.05 and a reliability of 95% were adopted. Results: The global evaluation in quality of life unveiled that 50.3% of the people interviewed considered their quality of life as good, followed by 40.5% who conveyed having a regular quality of life and in a lower frequency of 9.2% the people who expressed having a poor quality of life. Conclusion: After relating quality of life to each of the dimensions that constitute it, it can be inferred that the most affected dimensions were: physical, psychological and emotional well-being.
Abbreviations
WHO: World Health Organization; ESRD: End Stage Renal Disease; CKD: Chronic Kidney Disease; GFR: Glomerular Filtration Rate; KD: Kidney Disease; QOL: Quality of Life; HRQoL: Health Related Quality of Life.
Introduction
According to the World Health Organization (WHO) non-communicable diseases tend to be of long term and result from the combination of genetic, physiological, environmental and behavioral factors; today, they are the cause behind the majority of deaths and disabilities worldwide. These types of diseases are a serious public health problem that affects most nations, having a greater impact on populations dealing with vulnerable situations in the economic and social spheres [1]. Currently, they stand as the main cause of morbidity and mortality in developing countries, showing a significant increase in incidences and prevalence in population, becoming one of the greatest challenges for the health system at the international level [2].
Currently the adult population, along with the risks related to poor lifestyles are on the rise, increasing the presence of chronic non-communicable diseases, such as the End Stage Renal Disease (ESRD) which creates the necessity to design and implement strategies for health promotion, prevention, and risk-disease control that generate a shift in focus of the culture, a shift aiming for healthier lifestyles that enhances their quality of life [2].
Chronic Kidney Disease (CKD) is a condition that has been increasing at an alarming rate in the adult population around the world; given its irreversible nature, it generates a series of complicated conditions for its care and treatment, producing negative impacts in multiple areas of life including quality of life, which imply significant changes in the lifestyle of people which lead to repercussions in the familial, work and social areas. CKD is a condition that requires permanent health cares; in addition, it demands a complex, exigent and restrictive treatment which is linked to high social and financial costs for health care systems, a situation that sets boundaries on the quantity and quality of care that people require [3].
According to epidemiological studies, CKD is considered a serious health problem of the first order, not just because people with ESRD require significant health resources, but also because of the high rates of cardiovascular disease, hospitalization and premature death inherent in its diagnosis [4]. This condition is the final manifestation of diverse comorbidies presented by people, such as type 2 diabetes and high blood pressure, which represent the gradual and irreversible loss of renal function; therefore, patients must undergo renal replacement therapies such as kidney transplantation, and dialysis in its two modalities: hemodialysis and peritoneal dialysis [5]. It is necessary to keep into account that ESRD is generally easy to recognize, although the clinical diagnosis of the cause or the intrinsic pathologic alteration is usually not clearly established. Chronic Kidney Disease (CKD) in adults is defined as the presence of a structural or functional renal alteration (by sediment, imaging, or histology) which persists for more than three months, with or without the deterioration of renal function; or glomerular filtration rate (GFR) <60 ml / min / 1.73m2 without other signs of kidney disease. According to the KDIGO guidelines, high proteinuria, urinary disturbances, tubular-origin alterations and histological structural changes are considered markers of kidney damage [6, 7].
The severity of CKD is classified into 5 categories or grades based on GFR and three categories of albuminuria [6]. This is because proteinuria stands out as the most powerful prognostic factor of progression for CKD [8]. Deterioration of GFR is characteristic of grades 3-5, without other signs of kidney damage. However, categories 1 and 2 require the appearance of other signs of kidney damage. It is a dynamic classification under constant revision [9]. This classification, which undergoes slight and subtle changes over time, has the advantage of unifying the language concerning the definition and magnitude of the problem, previously defined as CKD [10]. Therefore, the methodology to measure GFR and determining proteinuria are key tools for the diagnosis and management of CKD [7, 11].
Currently, Kidney Disease (KD) is defined as a group of heterogeneous diseases that affect kidney structure and function. It is classified according to stages of severity, measured by Glomerular Filtration Rate (GFR), in addition to clinical diagnosis; there are treatments that can prevent its quick development and delay its progression to terminal stages [12]. Renal diseases have an increasing trend, similar to that of other chronic diseases such as Type 2 Diabetes (T2D) and High Blood Pressure (HBP). In order to evaluate and determine the causes of kidney disease in people, clinical settings must be examined, including personal and family history, along with social and environmental factors, drug therapy, physical examination, blood testing, diagnostic imaging and pathological diagnosis [6].
Kidney Disease: Improving Global Outcome (KDIGO) developed a clinical practice guideline on the evaluation, management and treatment of Chronic Kidney Disease (CKD); with the aim of proposing a new classification that encompasses the cause and severity of the disease. It is essential to identify the cause of CKD to predict progression and guide the choice of treatment. Severity is expressed by levels of Glomerular Filtration Rate (GFR) and albuminuria, and it is related to the risk of adverse outcomes, including kidney failure and death [6]. According to various studies, the highest incidence is observed in men with a 2:1 ratio in respect to women, and it is more frequent in adults over 60 years of age [13]. Nevertheless, predominance has recently been taking place in young adults of active working age, which implies a rapid progression towards End-Stage Kidney Disease, this not only negatively influences the quality of life of patients, but it also has repercussions on their economic situation [14]. Nowadays, non-communicable diseases have serious consequences that substantially affect the quality of life of people, this is due to the presence of higher financial repercussions coming directly from the expenses arising from the treatments and care requirements of specific health cares, which kindles an increase in the health care needs of the patient, and such increasing complexity of health cares is what results as the increasing need to talk about quality of life.
According to the WHO, quality of life (QOL) is defined as the individual’s perception of their position in life in the context of the culture and value systems where he lives in relation to his goals, expectations, standards and concerns. It is, indeed, colored by physical health, psychological state, level of independence, social relationships, environmental factors, and personal beliefs [15]. The QOL is an eminent human notion that relates to the person’s degree of satisfaction according to his physical condition, emotional state, love and social life, family relationships, as well as his own life meaning, among other things [16]. This is determined by the individual’s perception of his position in life within the context of the culture and value system in which he lives, and it is related to his goals, expectations, standards and interests [17].
The Health Related Quality of Life (HRQoL) is defined as the person’s subjective assessment of the impact his pathological condition and treatment have on his health through the person’s physical, mental and social perception, such perceptions could be affected by clinical manifestations, side effects of treatment and even through the relationships with their family and health professionals. CKD provides information about the physical and mental dimension of the patient, acting as a marker for the development of associated health problems. According to several studies, hemodialysis patients with lower levels in QOL are associated with a higher risk of hospitalization, complications, and death [18]. In this sense, QOL is closely related to the conditions that favor different ways of life, where being rather than having is privileged, given that it is closely related to the sense of the person, as an individual perspective and with a feeling of existential fulfillment. Therefore, in order to determine the attention provided by the family and those close to the patients, a resolution based on the quality of life must be carried on, for QOL is considered a human activity whose objective goes beyond the disease.
The concept of Health Related Quality of Life (HRQOL) essentially includes the patient’s perception as a necessity in the evaluation of health outcomes [19]. Authors such as Patrick and Erickson, define the health-related quality of life (HRQOL) as the measure in which the value assigned to the duration of life is modified according to the perception of physical, psychological and social limitations, along with the reduction of opportunities due to the disease, its long-term effects, treatments and health policies [20]. For Schumaker and Naugton, it is the subjective perception, influenced by the current state of health, the ability to perform those activities that are important to the individual [21]. The study was constituted using a descriptive and cross- sectional research design with a quantitative approach; the sampling size was determined through simple random sampling and it was composed by 131 patients. The information was collected using a scale to assess the QOL with a Cronbach’s Alpha of 0.86, prior written informed consents were employed for each person [22]. According to the inclusion criteria, people over 18 years of age with CKD who attended their hemodialysis replacement treatment and agreed to participate in the study signing the informed consent form were included, patients who presented any complications which interfered with their ability to answer the instrument were excluded along with patients who decided to withdraw from the research, Incomplete questionnaires were eliminated.
The information was collected through an instrument called Quality of Life Evaluation Scale (QOLES) the scale was made for the present research, it consists of 46 items distributed in ten dimensions with a Likert-type scale and five response options: excellent (5), very good (4), good (3), fair (2), and bad (1). The first dimension refers to the perception regarding quality of life and health status, the second subscale corresponds to psychological well- being; and the remaining eight involve dimensions of the quality of life model (Schalock and Verdugo, 2002/2003): physical, emotional and material well-being, interpersonal relationships, personal development, self-determination, social inclusion and rights [23].
Regarding the statistical analysis of socio-demographic categorical variables, descriptive statistics with frequency distribution and measures of central tendency were used. Furthermore, student’s t-test statistics were used for comparison of means; and lastly, the Pearson correlation coefficient and the Shapiro–Wilk test were also employed to determine the relationship between variables. A statistical significance value of p< 0.05 and a reliability of 95% were adopted. The data were processed with the SPSS IBM Statistics package version 23.
Ethical Considerations
This research work complies with the criteria and ethical standards of Belmont Report Declaration, the international ethical guidelines for biomedical research on human subjects. The present study was developed following the regulations of the General Health Law on Research for Health in Mexico. It was submitted for evaluation to the Ethics and Research Committee of the participating institution.
Results
According to the results, chronic kidney disease is the result of several factors that come together at a precise moment to govern and define the characteristics and living conditions of the patients who suffer from it, this implies that each particular individual lives his disease in a very specific way, even when the general situations that define this pathological condition can be shared with other individuals.
With regards to socio-demographic variables, the results from the age of the patients studied showed that the range of 60 to 69 years, occupied the highest percentage with 21.4%, however, the rest of the groups are not as distant as one might expect, as a matter of fact, those aged 30-39 years reached 18.3%, followed by the group of 40-49 years scoring 14.5%, which coincides with the result obtained from those aged 50-59 years, thus, according to the results previously mentioned it is possible to state that chronic kidney disease is found in all age groups, which is extremely important due to its impact on the lives of people of productive age due to their reduced life expectancies and complex treatments.
With respect to gender of the people surveyed, results showed an almost identical percentage between both genders, the female gender was positioned at the top with a score of 52.7%, quickly followed by the male gender reaching 43%. Regarding marital status, married people greatly predominated with a total of 53.4%, then, in a lower amount, those who said they were single scoring 25.2%, and lastly, to an even lesser degree, those in common law/civil union with 9.9%, the widowed with 7,6% and the divorced with 3.8%. Regarding the education of patients, a higher percentage of 57.2% belonged to the basic education level, the rest were distributed as 32.8% for people who completed elementary school, 24.4% for people who completed junior high school,
16% for people who completed high school, and lastly, 14.5% for people who obtained an Associate’s degree. (Table 1)
| Variable | Indicators | Frequency | % | |
|---|---|---|---|---|
| 20 – 29 | 19 | 14.5 | ||
| 30 – 39 | 24 | 18.3 | ||
| 40 – 49 | 19 | 14.5 | ||
| Age (years) | 50 – 59 | 19 | 14.5 | |
| 60 – 69 | 28 | 21.4 | ||
| 70 – 79 | 17 | 13 | ||
| 80 – 89 | 5 | 3.8 | ||
| Gender | Male | 62 | 47.3 | |
| Female | 69 | 52.7 | ||
| Single | 33 | 25.2 | ||
| Married | 70 | 53.4 | ||
| Marital Status | Common-law/civil union | 13 | 9.9 | |
| Divorced | 5 | 3.8 | ||
| Widowed | 10 | 7.6 | ||
| Illiterate | 10 | 7.6 | ||
| Elementary school | 43 | 32.8 | ||
| Middle School | 32 | 24.4 | ||
| Education | High School | 21 | 16 | |
| Associate’s degree | 5 | 3.8 | ||
| Bachelor’s degree | 19 | 14.5 | ||
| Master’s degree | 1 | 0.8 |
Table 1: Socio-demographic variables (age, gender, marital status, and education) of CKD patients undergoing Renal Replacement Th
Table 1: Socio-demographic variables (age, gender, marital status, and education) of CKD patients undergoing Renal Replacement Therapy. Source: Scale to Evaluate the Quality of Life of CKD Patients on Hemodialysis. According to the occupation of the participants, 33.6% reported not having any occupation, followed by those who reported being retired/pensioned with 20.6%, those who are currently employed amounted to 28.3%, this last percentage score summarizes every category in which participants carry out work activities, ranging from professional services to trades; the lesser percentages belonged to housewives with 9.9% and students with 7.6% respectively.
The above data are important to identify what proportion of patients has a work situation, the results showed that those who reported being productive were the 39.7%, while those who reported not working were the 60.3%. It is clear that CKD causes some type of disability that interferes with the patient’s ability to carry out work activities, which is reflected in a significant loss of work productivity, therefore, it is strongly recommended that patients continue with their professional activities or employment as much as possible, there is enough evidence showing the favorable impact that activity has in the physical, psychological and socioeconomical aspects of patients, furthermore it helps to maintain the system of social and medical benefits that guarantee the continuity of treatment and the stability of patients.
According to the income perceived by patients as wage of their work, the results showed that 47% of patients does not have any income, because they do not perform any work in which they could receive a financial remuneration, however, 20.6% expressed they are currently working and their biweekly financial income (expressed in US dollars) ranges from $110 to $149 dollars, followed by 25.9% which reported perceiving an average of $150 to $249 dollars, and lastly a proportion of 6.3% for the income average of $300 to $500 dollars, as it could be inferred, the economic situation in Mexico sets boundaries on the purchasing power of the Mexican people, limiting their possibilities and having a negative impact on the integral development of families, health and the nation.
Another important aspect are the questions that explored the financial dependence of respondents, where 48.1% indicated they were financially self- sufficient and able to provide for themselves and their basic needs, a high contrast for the 20.6% of patients, who stated to depend from their partners (wife/husband), furthermore, with a similar percentage, the 16.9% assured to be dependent from their sons/daughters and finally, the 3.7% who were dependent on another family member, such as brothers or uncles.
| Indicators | Frequency | % | |
|---|---|---|---|
| 44 | 33.6 | ||
| Retired/pensioned | 27 | 20.6 | |
| Occupation | Work activities and/or functions | 37 | 28.3 |
| Occupation | Housewife | 13 | 9.9 |
| Student | 10 | 7.6 | |
| Employment | Yes | 52 | 39.7 |
| Employment | No | 79 | 60.3 |
| Employment | 62 | 47.3 | |
| Income (Biweekly) | 27 | 20.6 | |
| From $150 to $249 dlls. | 34 | 25.9 | |
| From $300 to $500 dlls. | 8 | 6.3 | |
| Self-sufficient | 63 | 48.1 | |
| Parents | 14 | 10.7 | |
| Source of income | Husband/wife/partner | 27 | 20.6 |
| Source of income | Sons/daughters | 22 | 16.9 |
| Source of income | Other family members | 5 | 3.7 |
| Source of income | With parents | 23 | 17.6 |
| With nuclear family | 82 | 62.6 | |
| Housing | Alone | 4 | 3 |
| With relatives | 12 | 9.2 | |
| With sons/daughters | 10 | 7.6 | |
| Familial relationships | Good | 104 | 79.4 |
| Familial relationships | Regular | 27 | 20.6 |
Table 2: Socio-demographic variables (occupation, employment, income, source of income, housing and familial relationship) of pat
Regarding the questioning to identify who lives with the patient, 62.6% indicated that they lived with their family, 17.6% expressed they lived with their parents, 9.2% were living with a relative, 7.6% lived with their children and in a lower percentage of 3.0% the patients who referred living alone; This condition is related to the patient’s financial dependence, in regard to family relationships, 79.4% considered it to be good (Table 2).
Data from Table 2 corresponds to the socio-demographic variables that address occupation, employment, income, economic dependence, persons living with patient and familial relationships, this last variable is closely related to the age and health status of the patient, which is responsible for the deterioration of health and the physical, emotional and material well-being (economic status) of the patient, this is because entering the treatments of renal replacement therapy, requires candidates to undergo rigorous procedures and measures, which, in most instances, does not allow them to perform their normal activities at work and thus, receive an income that support their needs, being this the cause why a considerable amount of patients depend financially on their families. (Spouse, sons/daughters or parents) According to the time of disease evolution, the progression of patients undergoing renal replacement therapy ranges from one to nine years; nonetheless, it was observed that the highest percentage of patients, the 32.8%, belonged in the range of one to three years. Regarding the time of start of hemodialysis treatment, the majority of participants, an amount of 31.3%, answered one to two years, followed by 22.9% expressing less than one year, a score that represents an average of 2.68+1.4. After measuring the quality of life in patients with CKD undergoing hemodialysis replacement treatment, the expected range situates from 43 to 215 points, observing a minimum score of 109 points and a maximum score of 206 points, 50% of data are greater than or equal to 164, a mean average of 163 points was obtained, and a standard deviation of 21.5 points ranked as good quality of life, the score followed the normal distribution in the Shapiro-Wilk normality test (p> 0.03). (Table 3)
| Quality of Life | Frequency | Percentage | Mean | S.D. | P value |
|---|---|---|---|---|---|
| Bad | 12 | 9.2 | 2.41 | 0.655 | 0.003 |
| Regular | 53 | 40.5 | |||
| Good | 66 | 50.3 | |||
| Total | 131 | 100 |
Table 3: Quality of Life Scale score. Source: Quality of Life Scale to evaluate CKD patients on Hemodialysis After relating quali
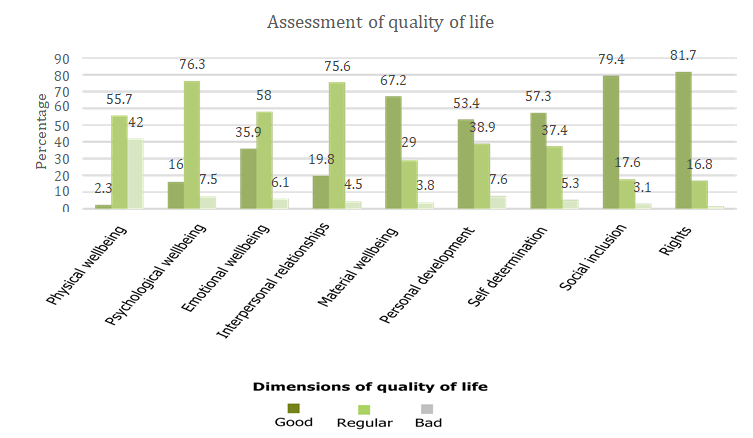
Table 3: Quality of Life Scale score. Source: Quality of Life Scale to evaluate CKD patients on Hemodialysis After relating quality of life to each of the dimensions that comprise it, it can be inferred that the most affected dimensions, were: physical, psychological and emotional well-being. Regarding physical well-being, 64.9% of the patients reported having pain or discomfort due to their health condition (although not being so significant statistically) as a result, 38.5% of them could not perform any activity or physical exercise, in addition, 30% expressed they are not satisfied with their health condition. In relation to the evaluation of quality of life, this dimension unveiled that 55.7% of the patients reported having a regular quality of life, followed by the 42%, who considered their quality of life as poor.
Another dimension is the psychological well-being of patients, the results evaluated this dimension as moderately significant with a value of 13,725 and p= .008, furthermore, according to the estimate of quality of life, 76.3% were located in regular, where 56.5% of patients reported having difficulty remembering important information for daily life, and the 46.6% stated they were not adapted to their new health condition.
An alteration was considered regarding the dimension of emotional well- being, according to the results, it was observed that its level of significance is highly significant, it has a value of 53.142 and p= .000, according to the evaluation of quality of life, 58% of patients considered their quality of life to be regular due to the presence of considerations linked to negativity and dissatisfaction with life and themselves, 30% conveyed they do not enjoy life and 50% considered that their life has no meaning. Likewise, 22% of patients reported not accepting their physical appearance, 38% felt useless and 30% reported not being motivated.
The panorama of a chronic disease, where treatment generates pain and discomfiture, as well as other risks such as dependence on medication and renal replacement therapy, involves fatigue and decreased mobility for the patient, on top of that, the treatment´s characteristics play a role as well, the process of connecting to a machine tree times per week in periods of four hours each time, have repercussions which affect not only physically but emotionally and even occupationally, this is because some patients cannot perform work activities.
In Dimensions 4, interpersonal relationships with a value of (p = 0.47), 5. Material well-being (p = 0.102), 6. Personal development (p = 0.001), 7. Self-determination (p = 0.000), 8.
Social inclusion ( p = 0.002) 9. Rights (p = 0.001) 5, 6, 7 8 and 9, as it could be noticed according to the p values, these are moderately significant and some very significant, according to the quality of life these values are shown as good except for the dimension of interpersonal relationships, where it was found to be fair. (Table 4, 5 and figure 1)
| Statistics | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Physical Wellbeing | Psychological Wellbeing | Emotional Wellbeing | Interpersonal Relationships | Material Wellbeing | Personal Development | Self Determi nation | Social Inclusion | Rights | |
| Mean | 1.6 | 2.08 | 2.3 | 2.15 | 2.63 | 2.31 | 2.52 | 2.76 | 2.8 |
| Median | 2 | 2 | 2 | 2 | 3 | 2 | 3 | 3 | 3 |
| S.D. | 0.536 | 0.481 | 0.578 | 0.472 | 0.558 | 0.609 | 0.599 | 0.494 | 0.437 |
Table 4: Dimensions of quality of life. Source: Quality of Life Scale to evaluate CKD patients on Hemodialysis.
| Dimensions of quality of life | Spearman’s | Quality of life | |||
|---|---|---|---|---|---|
| correlation | Good | Regular | Bad | ||
| 1. Physical wellbeing | Ro | 1.441 | 2.3% | 55.7% | 42% |
| Sig. | 0.837 | ||||
| 2. Psychological wellbeing | Ro | 13.72 | 16% | 76.3% | 7.5% |
| Sig. | 0.008 | ||||
| 3. Emotional wellbeing | Ro | 53.14 | 35.9% | 58% | 6.1% |
| Sig. | 0 | ||||
| 4. Interpersonal relationships | Ro | 9.618 | 19.8% | 75.6% | 4.5% |
| Sig. | 0.47 | ||||
| 5. Material wellbeing | Ro | 7.72 | 67.2% | 29% | 3.8% |
| Sig. | 0.102 | ||||
| 6. Personal development | Ro | 18.67 | 53.4% | 38.9% | 7.6% |
| Sig. | 0.001 | ||||
| 7. Self determination | Ro | 35.85 | 57.3% | 37.4% | 5.3% |
| Sig. | 0 | ||||
| 8. Social inclusion | Ro | 16.55 | 79.4% | 17.6 | 3.1% |
| Sig. | 0.002 | ||||
| 9. Rights | Ro | 19.42 | 81.7% | 16.8% | 1.5% |
| Sig. | 0.001 | ||||
| Ro= Spearman’s correlation. Sig= Significance. | |||||
| **. Correlation is significant at the 0.01 level. *. Correlation is significant at the 0.05 level. | |||||
| Source. Quality of Life Scale to evaluate CKD patients on Hemodialysis |
Table 5: Relationship between the dimensions of quality of life. Source: Quality of Life Scale to evaluate CKD patients on Hemodi
Discussion
According to data obtained by López-López in 2016: Calidad de vida en hemodiálisis y diálisis peritoneal tras cuatro años de tratamiento (Quality of life in hemodialysis and peritoneal dialysis), participants experienced mental effects (47%), physical effects (34%), burden of CKD (46%), effects of CKD (55%) and symptoms typical of the pathology (71%) [24]. These data are similar to those found in the present study, according to the dimensions of quality of life evaluated, it was possible to identify the dimensions with the greatest impact on patients, such dimensions are: physical well- being (55.7%), psychological well-being reaching (76%), and alterations in the emotional well-being dimension with (58%).
Conclusions
It is clear that CKD shows slight differences according to gender; according to the results, prevalence is higher in women; regarding the progression of the disease, it is faster in men and according to the prognosis, young women undergoing renal replacement therapy increase their non- cardiovascular mortality rate and lose the survival advantage over men in the general population. In this sense, the higher prevalence of CKD in women is related to life expectancy, which is higher for women than men.
CKD occurs regardless of the patient’s marital status, this is because it does not represent a risk factor to determine its cause; However, it is a condition that significantly influences the life of the patient’s partner, this is due to the family support and the implications needed so that the patient can face his health condition, a new health condition where there are changes in the activities of daily life, mood, spirituality and perception of life; Therefore, the response to this situation from the patient’s partner and family are fundamental for all these processes. The socioeconomic condition of patients with CKD is an extremely important aspect due to the implications for their state of health and quality of life, given that this pathology occurs more and more at early ages of life, especially in the economically active population, this implies a substantial impact in the work or occupation of the patient by reason of their health condition and the strict treatment that it demands, such impact has a remarkable prominence in patients with jobs where the functions performed are remunerated with low salaries, sometimes not in accordance with the activities they carry out, in some scenarios, the impact presents itself as a plain job loss, which limits their financial income, affecting the family nucleus, leaving an income that is insufficient to cover the basic needs and the treatment that the patient requires, such as those of the family, in which the primary provider is the patient.
However, even when family support is present, this circumstantial situation generates feelings of sadness in the person, existential conflicts begin to appear, where the patient expresses feeling various types of losses such as: financial position, work or occupation, together with the loss of health, self-worth, and of the functions of the organism, which limit the adaptation to the new health condition, which makes heavy repercussions for the patient’s quality of life. The greatest impact comes when CKD is in its advanced stage, this stage represents a great impact over the health related quality of life (HRQOL) of those who develop it, living with this affection can be hard and complex in both the short and long term. From the initial stages until the terminal ones, symptoms, restrictions (specially dietetic), and treatment are reflected in the daily life of patients, this condition requires heavy acceptance and adherence from the patient side, especially when it comes to treatment [25].
Facing adversity in health (such as CKD, a chronic phase or the terminal stage of a disease) has an effect not only in the body, but also in the mind and soul of patients, thus it is crucial to consider these two additional dimensions that play a role when health it’s compromised. Rather than just focusing on the body and aim to restore its health, healthcare professionals need to visualize the from a higher perspective that allows them to dimension the patient in its completeness, a perspective which encompasses the wholeness of human beings, specially the human mind, a disposed mind can make the difference in the course of any disease [26].
The QoL in people living with CKD on Renal Replacement Therapy (RRT) is substantially decreased as a result of HD treatment; By relating quality of life to each of the dimensions that comprise it, it can be inferred that the dimensions most affected were: physical, psychological and emotional wellness, having serious repercussions for the state of health and therefore the quality of life of the person.
References
-
(2021) Non communicable diseases. World Health Organisation.
-
(2019) National Development Plan of Mexico 2019- 2024. Official Gazette of the Federation, Government of Mexico, pp: 1-64.
-
Mendes de Abreau M, Walker D, Sesso R, Ferraz M (2011) Health Related Quality of Life of Patients Receiving Hemodialysis and Peritoneal Dialysis in Sao Paulo, Brazil: A Longitudinal Study. Value Health 14(5): S119-S121.
-
Canal C, Pellicer R, Facundo C, Gràcia-Garcia S, Montañés-Bermúdez R, et al. (2014) Tables for estimating the glomerular filtration rate using the new CKD-EPI equation from serum creatinine concentration. Nephrology Madrid 34(2): 223-229.
-
Krederdt S, Taboada DY, Meléndez E (2020) Perceived quality of life in ambulatory patients with terminal chronic renal failure. Scientific Nursing Magazine 9(2): 2-15.
-
Kidney Disease: Improving Global Outcomes (KDIGO) (2013) Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney International Supplements 3(1): 1-150.
-
Levey AS, de Jong PE, Coresh J, El Nahas M, Astor BC, et al. (2011) The definition, classification, and prognosis of chronic kidney disease: a KDIGO Controversies Conference Report. Kidney Int 80(1): 17-28.
-
Hallan SI, Ritz E, Lydersen S, Romundstad S, Kvenild K, et al. (2009) Combining GFR and albuminuria to classify CKD improves prediction of ESRD. J Am Soc Nephrol 20(5): 1069-1077.
-
Levey AS, Eckardt KU, Tsukamoto Y, Levin A, Coresh J, et al. (2005) Definition and classification of chronic kidney disease: a position statement from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int 67(6): 2089-2100.
-
Vassalotti JA, Stevens LA, Levey AS (2007) Testing for chronic kidney disease: a position statement from the National Kidney Foundation. Am J Kidney Dis 50(2): 169-180.
-
Gorostidi M, Santamaria R, Alcazar R, Fernandez- Fresnedo G, Galceran JM, et al. (2014) Spanish Society of Nephrology document on KDIGO guidelines for the assessment and treatment of chronic kidney disease. Nefrologia 34(3): 302-316.
-
Bencomo RO (2015) Chronic Kidney Disease: preventing it, better than treating it. Cuban Journal of Comprehensive General Medicine 31(3).
-
Barberena NS, Polo Amarante RA, Mendez Rogríguez SN, Barberena MS (2016) Characterization of patients with chronic kidney disease undergoing hemodialysis treatment. MediSur 14(4): 382-388.
-
Martínez R I (2012) Quality of Life of patients in hemodialysis and continuous ambulatory peritoneal dialysis programs. (Bachelor’s Degree Thesis, Universidad Veracruzana).
-
(1996) What quality of life? The WHOQOL Group. World Health Organization Quality of Life Assessment. World Health Forum 17(4): 354-356.
-
Schwartzmann L (2003) Health-related quality of life: conceptual aspects. Science and nursing 9(2): 09-21.
-
The World Health Organization Quality of Life assessment (WHOQOL): position paper from the World Health Organization (1995) Soc Sci Med 41(10): 1403- 1409.
-
Marín López MT, Rodríguez-Rey R, Montesinos F, de Galvis SR, Ágreda-Ladrón MR, et al. (2021) Factors associated with quality of life and its prediction in kidney patients on hemodialysis. Nephrology Magazine 42(3): 1-9.
-
Testa M, Simmonson D (1996) Assessment of Quality-of- Life Outcomes. N Engl J Med 334(13): 835-840.
-
Patrick D, Erickson P (1993) Health Status and Health Policy: Quality of life in Health Care Evaluation and Resource Allocation. Oxford University Press New York, pp: 478.
-
Naughton MJ, Shumaker SA, Anderson RT, Czajkowski SM (1996) Psychological Aspects of Health-Related Quality of Life Measurement: Tests and Scales. Quality of Life and Pharmaco economics in Clinical Trials 15: 117-131.
-
Hernández Sampieri R, Mendoza Torres C (2018) Research Methodology, quantitative, qualitative and mixed routes. In: (1st Edn.), McGraw Hill Publishing, Mexico, pp: 148-217.
-
Schalock RL, Verdugo MA (2007) The concept of quality of life in services and supports for people with intellectual disabilities. Spanish Magazine on intellectual disabilities 38(4): 21-36.
-
López y López LR, Baca-Córdova A, Guzmán-Ramírez PM, Ángeles-Acuña A, Ramírez-del Pilar R, et al. (2017) Quality of life in hemodialysis and peritoneal dialysis after four years of treatment. Internal Medicine of Mexico 33(2): 177-184.
-
Ruiz MA, Pardo A (2005) Health-related quality of life: definition and use in medical practice. Pharmacoeconomics-Spanish Research Articles 2(1): 31-43.
-
Puchalski CM (2002) Spirituality and end-of-life care: a time for listening and caring. J Palliat Med 5(2): 289-294.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda