Cardiovascular Morbidity and Mortality in Sub-Saharan Africa; Wide Hospital Survey in Democratic Republic of Congo
Background: Cardiovascular diseases are the leading cause of death worldwide. In Sub-Saharan Africa, alongside infectious diseases which once constituted the main burden of mortality, we are witnessing a meteoric rise in cardiovascular diseases. However, the evidence is still lacking in Subsaharan Africa. The objective of this study was to determine, over a ten-year period, the burden of major cardiovascular diseases in hospital morbidity and mortality in a large sub-saharan african city, Kinshasa. Methods: This is a study relating to the descriptive epidemiology of cardiovascular diseases covering a period of ten years, from 2007 to 2016, conducted in the main hospital facilities in the city of Kinshasa, a city of more than 10 million. of inhabitants. Results: A total of 62,553 patients were listed; cardiovascular pathologies affected 19,480 patients, representing 31% of all patients hospitalized in the medical sector. Deaths concerned 10,790 patients, i.e. an overall mortality rate of 17%, and 3,814 patients died of cardiac causes, i.e. 35% of all deaths. Stroke accounted for 53% of cardiovascular morbidity, 16.6% of overall morbidity, 55.7% of cardiovascular mortality and 19.7% of overall mortality. From 2007 to 2016, cardiovascular diseases experienced a significant increase in hospital morbidity, going from 36.4 to 39.4% (P=0.0001), unlike other diseases. Conclusion: The present study confirms the alarming progression of cardiovascular diseases in Sub-Saharan Africa where it constitutes a major public health problem. Stroke is the leading cause of cardiovascular morbidity and mortality. Given the current insufficiency of medical infrastructure and human resources in this area, prevention constitutes, more in Sub-Saharan Africa than elsewhere, the best way to reduce the burden of these diseases.
Abbreviations
CVD: Cardiovascular Diseases; CVRF: Cardiovascular Risk Factor; NCD: Non-Communicable Diseases; SSA: Sub- Saharan Africa; IM: Internal Medicine; CT-scan: Computed Tomography; VTE: Venous Thromboembolism.
Introduction
Cardiovascular diseases (CVD), also called cardio- neurovascular diseases, constitute a group of disorders affecting the heart and blood vessels, including coronary heart disease, cerebrovascular disease, peripheral arteriopathy, rheumatic heart disease, congenital heart defects, deep vein thrombosis and pulmonary embolism [1]. To this list, we should add arterial hypertension, the most powerful cardiovascular risk factor (CVRF), cardiomyopathy and other non-rheumatic valvular diseases, as well as heart failure, the endpoint of the majority of CVD. CVD is the leading cause of death worldwide.
It is estimated that in 2012, 17.5 million people died from it, or 30% of all deaths worldwide. An estimated 7.5 million of these deaths are due to coronary heart disease and 6.7 million are due to stroke.
By 2030, nearly 23.6 million people will die from cardiovascular diseases, mainly heart disease and stroke. These conditions are projected to remain the leading cause of death worldwide [2].
It is estimated that 80% of these deaths occur in low- and middle-income countries, which face a double burden of infectious diseases and the increasing burden of non- communicable diseases (NCD). Even more, 85% of premature deaths, those occurring between ages 30 and 69, occur in these countries [3].
However, in these countries, basic epidemiological data are very little known. The few hospital studies and sometimes in the general population carried out over the last three decades indicate that infectious diseases constitute the leading cause of mortality in sub-Saharan Africa (SSA), followed by CVD or that cardiovascular diseases are experiencing exponential growth; this is notably the case of a Nigerian hospital study and another from Cameroon [4, 5].
In the Democratic Republic of Congo (DR Congo), there is no large-scale study on cardiovascular morbidity and mortality either at the hospital level or in the general population on a national scale. . It is in this context that this study takes place, consisting of a large hospital survey which covers one of the largest cities in sub-Saharan Africa (SSA), Kinshasa, capital of DR Congo.
Objective: determine over a ten-year period the burden of major CVDs in hospital morbidity and mortality in a large city in sub-Saharan Africa, Kinshasa.
Method
Type of Study
This is a descriptive and cross-sectional study covering a period of ten years, from 2007 to 2016. Secondarily, some analytical aspects were addressed in the comparative evaluation of these diseases as well as in their projection in the near future.
Location of The Study
The study was conducted in the main hospital facilities in the city of Kinshasa, capital of DR Congo, a city of more than 10 million inhabitants. Hospital of Kinshasa, Saint-Joseph Hospital, Bondeko Hospital, Sino-Congolese Friendship Hospital, Nganda Hospital Center and Monkole Hospital Center.
Study Size
This is an exhaustive sample made up of all hospitals meeting the criteria relating to the diagnosis and management of CVD. The survey thus covered eight hospitals in the city that met the criteria as described in the “data collection” section, for a total number of 62,553 patients. . These are the following hospitals: Kinshasa University Clinics, Ngaliema Clinic, Kinshasa Provincial General Reference Hospital, Saint-Joseph Hospital, Bondeko Hospital, Sino-Congolese Friendship Hospital, Nganda Hospital Center and Monkole Hospital Center.
Study Parameters
Parameters of interest included patient numbers, discharge diagnosis and vital outcome. All patients were analyzed globally without distinction of age groups.
Inclusion Criteria for Registers and Files
All patient files registered in hospital in the medical sector, with a discharge diagnosis and an identified discharge modality (vital outcome) were included in the study. Registers or files with missing data were excluded from the study.
Data Collection and Ethical Aspect
The data were taken from hospitalization registers and, when necessary, from medical files, within the internal medicine (IM) and/or cardiology departments as well as in the medical units. multipurpose intensive care of internal medicine. All these different services are run by doctors specializing in internal medicine/cardiology, thus offering a minimum of diagnostic reliability. The availability of the minimum paraclinical examinations necessary for the diagnosis of cardiovascular pathologies was effective in the majority of the hospital establishments concerned or nearby for a few others. These include computed tomography (CT-scan), cardiac and vascular Doppler ultrasound, electrocardiography as well as a medical biology laboratory where routine cardiological examinations are carried out.
All hospitals used the international classification of diseases ICD-10, chapter 09, dedicated to diseases of the circulatory system.
Since the survey focused exclusively on the registers and files of patients who had already been discharged from hospitals several months or years earlier, there was therefore no contact with the patients. Authorization from the national ethics committee and from the management committee of each hospital were obtained on the basis of the study protocol.
Statistical Analysis
The data were analyzed on EXCEL and SPSS IBM Version 20. The description of different parameters was made by calculating frequencies. The Chi-2 test allowed the comparison of frequencies. The forecast of developments over the next ten years was made using the combined model approach including the ARIMA, ETS, NNAR, STL and TBATS methods. The significance level was set at 5%.
Results
Cardiovascular Morbidity and Mortality
A total of 62,553 patients were listed; cardiovascular pathologies affected 19,480 patients, or 31% of all patients hospitalized in the medical sector.
Deaths concerned 10,790 patients, i.e. an overall mortality rate of 17%, and 3,814 patients died of cardiac causes, i.e. 35% of all deaths.
Stroke accounted for 53% of cardiovascular morbidity, 16.6% of overall morbidity, 55.7% of cardiovascular mortality and 19.7% of overall mortality (Table 1).
| CVD | Morbidity | Mortality | ||
|---|---|---|---|---|
| n | % | n | % | |
| Stroke | 10367 | 16,57 | 2124 | 19,68 |
| Heart failure | 5477 | 8,76 | 876 | 8,12 |
| Ischemic cardiopathy | 501 | 0,80 | 86 | 0,80 |
| Pulmonary embolism | 278 | 0,44 | 103 | 0,95 |
| Deep vein thrombosis | 246 | 0,39 | - | - |
| Pericarditis | 81 | 0,13 | 13 | 0,12 |
| Valvular heart diseases | 79 | 0,13 | 12 | 0,11 |
| Bacterial endocarditis | 6 | 0,01 | 2 | 0,02 |
| Acute articular rhumatism | 13 | 0,02 | 1 | 0,01 |
| Other CVDs | 2432 | 3,89 | 597 | 5,53 |
| All CVDs | 19480 | 31,14 | 3814 | 35,35 |
| Non-cardiovascular diseases | 43073 | 68,86 | 6976 | 64,65 |
| Total internal medicine hospitalisation | 62553 | 100,00 | 10790 | 100,00 |
Table 1: Cardiovascular morbidity and mortality
CVDs: Cardiovascular diseases. Table 1: Cardiovascular morbidity and mortality
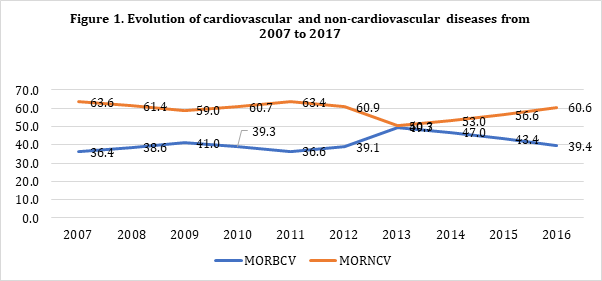
Evolution of the morbidity of cardiovascular diseases and non-cardiovascular diseases from 2007 to 2016.
From 2007 to 2016, CVD experienced a significant increase in hospital morbidity, going from 36.4 to 39.4% (P=0.0001) while other diseases in the medical sector experienced a decline, going from 63.6 to 60.6% (Figure 1).
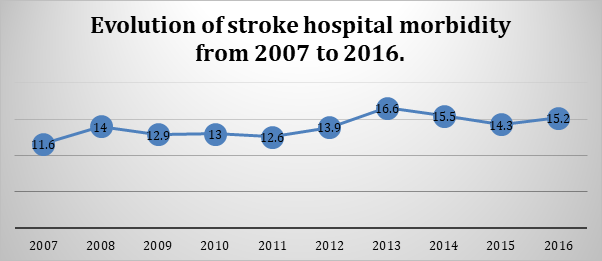
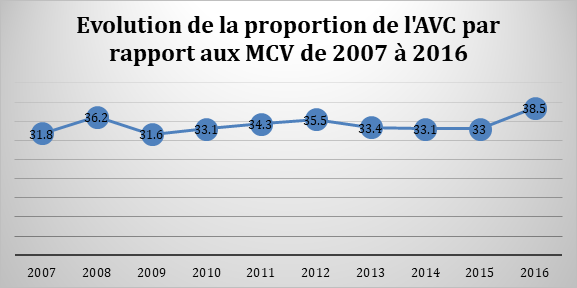
Evolution of stroke from 2007 to 2016 in Kinshasa.
Stroke has experienced an increasing and significant trend in Kinshasa (Figure 2), going from 11.6% of all hospitalized patients in 2007 to 15.2% in 2016 (P=0.0001). It represented 31.8% of all cardiovascular pathologies in 2007 compared to 38.5% in 2016 (Figure 3).
Comparison of cardiovascular morbidity and mortality between 2007 and 2016.
The morbidity of all CVDs increased between 2007 and 2016 (P=0.0001) while their mortality rather decreased (P=0.01).
Stroke morbidity in the same period also increased (P=0.0001) while their mortality remained statistically unchanged. These data are summarized in Table 2.
| Years | Morbidity | Mortality | ||||
|---|---|---|---|---|---|---|
| 2007 | 2016 | P | 2007 | 2016 | P | |
| N= 5246 | N= 9480 | N= 846 | N= 1198 | |||
| CVDs | 1907(36.4%) | 3734(39.4%) | 0.0001 | 323(38.2%) | 418(34.8%) | 0.01 |
| Stroke | 607(11.6%) | 1437(15.2%) | 0.0001 | 168(19.9%) | 245(20.5%) | 0,57 |
Table 2: Comparison of cardiovascular morbidity and mortality between 2007 and 2016.
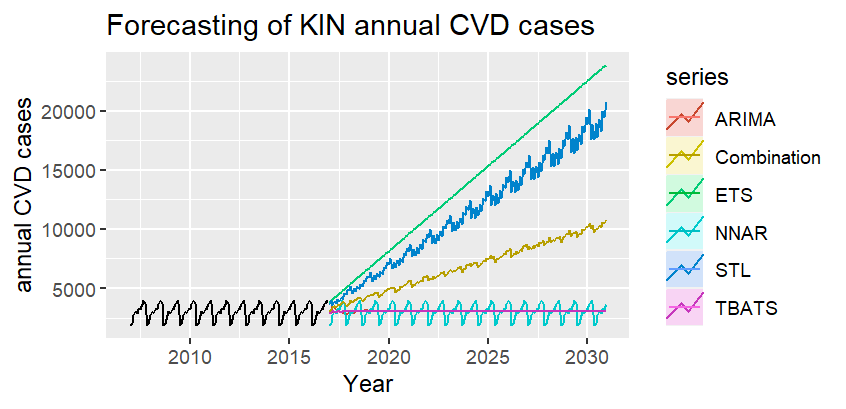
Forecast of the evolution of CVD by 2030.
The forecast approach of the combined model predicts for most of the methods used an exponential evolution of CVD by 2030, as indicated in Figure 4.
Discussion
The present hospital survey highlights the significant and increasing burden of CVD, and especially stroke, in comparison to previous local and sub-Saharan data; it also highlights the place of stroke which appears as the leading cause of cardiovascular death in sub-Saharan Africa, far ahead of ischemic heart disease which is known in other regions of the world, especially in the West, as the leading cause of death.
Indeed, this hospital survey reveals that in the period from 2007 to 2016, CVD represented 31% of all patients hospitalized in the medical sector in the city of Kinshasa and 35% of all deaths. Stroke accounted for 53% of cardiovascular morbidity, 16.6% of overall morbidity, 55.7% of cardiovascular mortality and 19.7% of overall mortality. These results reflect the same profile as that of a hospital survey carried out thirty years ago in one of the main establishments concerned by the present survey, at the same time as they show the increasing trend in the burden of CVDs. This previous survey, which focused on stroke, indicated that it represented 31% of cardiovascular morbidity, 6% of overall morbidity, 57% of cardiovascular mortality and 12% of overall mortality [6]. The two surveys indicate that stroke is the leading cause of cardiovascular death in sub-Saharan Africa, as indicated by a large African study covering the period from 1990 to 2013 [7]. Likewise, the Nigerian study on hospital morbidity and mortality mentioned above and carried out in 2020, indicated that CVD represented the 2nd
cause of mortality after infectious diseases, with 15.8% and 22.7% respectively. Set of deaths [4].
The increasing evolution of CVDs in SSA and the preeminent place of stroke now constitute a known reality and described in the scientific literature [7, 8, 9, 10]. This illustrates the notion of epidemiological transition [11] in which most low-income countries currently find themselves, which face a concomitant double burden, that of NCDs and that of infectious diseases.
This epidemiological shift results from several factors, notably the improvement in the management of infectious diseases and the adoption of a new way of life in urban and peri-urban areas, characterized by a tendency towards a sedentary lifestyle and a diet rich in sodium. and calories, excessive alcohol consumption, socio-professional stress, all this in a context of poverty or social precariousness linked in particular to an uncontrolled rural exodus. The juxtaposition of these behavioral risk factors results in an increase in biological or physiological risk factors [12, 13, 14, 15]. Furthermore, the role of climate change in the rise of CVD is increasingly mentioned in several studies, although in SSA, the results still remain disparate, probably due to the diversity of methodologies used [16, 17, 18, 19, 20, 21].
Ischemic heart disease is increasing in SSA, much more than in many other regions of the world, due in particular to the progression of FDRCV and the epidemiological transition [22]. However, in this survey, it comes far behind stroke and all-cause heart failure probably due to underdiagnosis or often late diagnosis, at the stage of heart failure.
Rheumatic valve disease does not feature prominently in this survey. Recent data in Africa indicate that CVD linked to poverty and malnutrition, such as rheumatic valve disease, once very common in Africa [23, 24, 25], is currently decreasing in favor of atherosclerotic diseases such as high blood pressure, coronary heart disease and heart failure [22].
Venous thromboembolism (VTE) is on the rise in SSA due in particular to the lack of preventive measures. Indeed, in a study carried out in five SSA countries, more than half of patients at risk of thromboembolism did not benefit from preventive measures, in this case preventive anticoagulant treatment [26].
By their proximity to other CVDs as well as surgical contexts which most often require prolonged immobilization, VTEs are among the emerging pathologies in SSA [27, 28] and are in the process of supplanting rheumatic valve disease, such as indicate the results of the present study. Unfortunately, the epidemiology of VTE is still insufficiently exploited in SSA.
Regarding the epidemiological profile by 2030, in terms of morbidity and mortality, the models used in the present survey project an increasing evolution of CVD, like other forecast models used at the African level [29, 30], if States do not strengthen their health policies in terms of prevention and control of CVRF. There is therefore a need and urgency for SSA States to strengthen CVD screening and prevention strategies.
Limitations of The Study
Some registers and medical files were not necessarily well maintained, leading to the exclusion of some cases with possibly some influence on the statistics. Furthermore, a certain selection bias could exist due to a survey in a hospital environment.
Conclusion
The present study confirms the alarming progression of CVD in SSA where it constitutes a major public health problem in terms of morbidity and mortality. Stroke is the leading cause of cardiovascular morbidity and mortality both in DR Congo and across Africa. Given the current insufficiency of medical infrastructure and human resources in this area, prevention is more in SSA than elsewhere, the best way to reduce the burden of these diseases, prevention based on improving lifestyle, early detection and management of FDRCV. There is reason to consider a subsequent study of a broader scope with a view to confirming the trends that emerged in the present investigation.
Conflicts of Interest
The authors have no conflict of interest to declare.
• Thanks To the entire team of the National Cardiovascular Diseases Control Program in DR Congo.
References
-
(2017) Cardiovascular diseases. WHO.
-
(2020) About cardiovascular diseases. WHO.
-
(2018) UN General Assembly Third High-level Meeting on NCDs. WHO.
-
Okoroiwu HU, Uchendu KI, Essien RA (2020) Causes of morbidity and mortality among patients admitted in a tertiary hospital in southern Nigeria: A 6 year evaluation. PLoS One 15(8): e0237313.
-
Nkoke C, Jingi AM, Makoge C, Teuwafeu D, NKouonlack C, et al. (2019) Epidemiology of cardiovascular diseases related admissions in a referral hospital in the South West region of Cameroun ; A cross sectional study in sub- Saharan Africa. PLoS One 14(12) : e0226644.
-
Mbala Mukendi M, Tambwe MJ, Lizwa BB, Dikasa NL, M’Buyamba Kabangu JR (1994)Morbidity and mortality of the Zairean adult; Panorama med 5: 234-237.
-
Mensah GA, Roth GA, Sampson UK, Moran AE, Feigin VL, et al. (2015) Mortality from cardiovascular diseases in sub-Saharan Africa, 1990–2013: a systematic analysis of data from the Global Burden of Disease Study 2013. Cardiovasc J Afr 26(2): S6-S10.
-
Yuyun MF, Sliwa K, Kengne AP, Mocumbi AO, Bukhman G (2020) Cardiovascular Diseases in Sub-Saharan Africa Compared to High-Income Countries: An Epidemiological Perspective. Glob Heart 15(1): 15.
-
Shehu MN, Adamu UG, Ojji DB, Ogah OS, Sani MU (2023) The Pandemic of Coronary Artery Disease in the Sub- Saharan Africa: What Clinicians Need to Know. Curr Atheroscler Rep 25(9): 571-578.
-
Alhuneafat L, Ta’ani OA, Tarawneh T, ElHamdani A, Al-Adayleh R, et al. (2024) Burden of cardiovascular disease in Sub-Saharan Africa, 1990-2019: An analysis of the Global Burden of Disease Study. Curr Probl Cardiol 49(6): 102557.
-
Omran AR (2005) The epidemiologic transition: a theory of the epidemiology of population change. Milbank Q 83(4): 731-757.
-
Limbole Bakilo E, Nkarnkwin Kasanza DS, Womba L, Atheno V, Kika M, et al. (2021) Lifestyle and cardiovascular risk factors: urban population versus rural population in sub-Saharan Africa; in “Lifestyle and epidemiology - Poverty and cardiovascular diseases, a double burden for African Populations”. IntechOpen, pp: 163-176.
-
Longo-Mbenza B, Vangu Ngoma D, Nahimana D, Mupepe Mayuku D, Mbungu Fuele S, et al. (2008) Screen detection and the WHO stepwise approach to the prevalence and risk factors of arterial hypertension in Kinshasa. Eur J Cardiovasc Prev Rehabil 15(5): 503-508.
-
Aspray TJ, Mugusi F, Rashid S, Whiting D, Edwards R, et al. (2000) Rural and urban differences in diabetes prevalence in Tanzania: the role of obesity, physical inactivity and urban living. Transactions of the Royal Society of Tropical Medicine and Hygiene 94(6): 637‑644.
-
Poulter NR, Khaw K, Hopwood BE, Mugambi M, Peart WS, et al. (1985) Determinants of blood pressure changes due to urbanization: a longitudinal study. Journal of Hypertension Supplement 3(3): S375‑377.
-
Amegah AK, Rezza G, Jaakkola JJ (2016) Temperature- related morbidity and mortality in Sub-Saharan Africa: A systematic review of the empirical evidence. Environ Int 91: 133-149.
-
Kintoki Mbala F, Longo-Mbenza B, Mbungu Fuele S, Zola N, Motebang D, et al. (2016) Impact of seasons, years El Nino/La Nina and rainfalls on stroke-related morbidity and mortality in Kinshasa. J Mal Vasc 41(1): 4-11.
-
Lokotola CL, Wright CY, Wichmann J (2020) Temperature as a modifier of the effects of air pollution on cardiovascular disease hospital admissions in Cape Town, South Africa. Environ Sci Pollut Res Int 27(14): 16677-16685.
-
Arisco NJ, Sewe MO, Bärnighausen T, Sié A, Zabre P, et al. (2023) The effect of extreme temperature and precipitation on cause-specific deaths in rural Burkina Faso: a longitudinal study. Lancet Planet Health 7(6): e478-e489.
-
Greibe Andersen J, Kallestrup P, Karekezi C, Yonga G, Kraef C (2023) Climate change and health risks in Mukuru informal settlement in Nairobi, Kenya - knowledge, attitudes and practices among residents. BMC Public Health 23(1): 393.
-
Bühler JL, Shrikhande S, Kapwata T, Cissé G, Liang Y, et al. (2022) The Association between Apparent Temperature and Hospital Admissions for Cardiovascular Disease in Limpopo Province, South Africa. Int J Environ Res Public Health 20(1): 116.
-
Shehu MN, Adamu UG, Ojji DB, Ogah OS, Sani MU (2023) The Pandemic of Coronary Artery Disease in the Sub- Saharan Africa: What Clinicians Need to Know. Curr Atheroscler Rep 25(9): 571-578.
-
Maru M (1993) The changing pattern of cardiovascular diseases in Ethiopia. East Afr Med J 70(12): 772-776.
-
Longo-Mbenza B, Bayekula M, Ngiyulu R, Kintoki VE, Bikangi NF, et al. (1998) Survey of rheumatic heart disease in school children of Kinshasa town. Int J Cardiol 63(3): 287-294.
-
Oli K, Porteous J (1999) Prevalence of rheumatic heart disease among school children in Addis Ababa. East Afr Med J 76(11): 601-605.
-
Kingue S, Bakilo L, Ze Minkande J, Fifen I, Gureja Y, et al. (2014) Epidemiological African day for evaluation of patients at risk of venous thrombosis in acute hospital care settings. Cardiovasc J Afr 25(4): 159-164.
-
Gebremedhin A, Shamebo M (1998) Deep venous thrombosis in a university teaching hospital, Addis Ababa, Ethiopia. East Afr Med J 75(7): 432-435.
-
Mulatu A, Melaku T, Chelkeba L (2020) Deep Venous Thrombosis Recurrence and Its Predictors at Selected Tertiary Hospitals in Ethiopia: A Prospective Cohort Study. Clin Appl Thromb Hemost 26: 1076029620941077.
-
Mathers CD, Loncar D (2006) Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med 3(11): e442.
-
Lopez AD, Mathers CD (2006) Measuring the global burden of disease and epidemiological transitions: 2002-2030. Ann Trop Med Parasitol 100(5-6): 481-499.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda