Urogenital Schistosomiasis: Knowledge, Attitude, and Control Practices among Rural Communities in the Atiwa West District, Ghana
Background: Ghana and other Sub-Saharan African countries have a high prevalence of urogenital schistosomiasis due to insufficient awareness of the potential risks of infection. Despite routine mass drug administration (MDA) in endemic areas, sustainable control interventions require knowledge about the disease, its causes, route of transmission, signs and symptoms, control, and risk factors. Therefore, strategic perspectives or elements for treating urogenital schistosomiasis in high-risk groups include knowledge, attitude, and preventive measures. Objective: To assess urogenital schistosomiasis knowledge (K), attitudes (A), and control practices (P) in four rural communities in Atiwa West District. Methods: A cross-sectional study using a structured survey assessed the KAP among households in four rural communities within the Atiwa West District. Results: The study included 400 household heads in total, and a prevalence of 14.57% was recorded among children for urogenital schistosomiasis. 84.50% have heard about the disease, but their knowledge of its signs and symptoms, transmission, and prevention was limited. Individuals with water-related occupations have a significantly higher risk of infection (OR = 4.063) than those with non-waterbody-related occupations, with males having a substantially higher risk of infection (OR = 2.861) than females. Uneducated participants have a higher risk of urogenital schistosomiasis compared to educated participants (OR = 0.45; 95% CI = 0.24, 0.86; p = 0.016). 26.25% believe that providing a safe water supply would help control and prevent the disease; however, 64.25% still rely on unsafe water sources for domestic use, which will trigger infection to persist. The study recorded good attitudes among participants, but 25.75% and 33.50% urinate or defecate in water and swim or fish, respectively. Although 50% suggested that health education and promotion programs are essential to schistosomiasis intervention, these initiatives are minimal within the study area, and residents still need clarification about the infection status and KAPs. Conclusion: The study revealed that people in the Atiwa West District have fair control practices, positive attitudes, and moderate knowledge regarding urogenital schistosomiasis transmission. To overcome this, intensive health education at both community and school levels is required. Health education should focus on the causes, transmission routes, and health effects of urogenital schistosomiasis. In addition, providing tap water for domestic and pit latrines within vulnerable communities helps reduce the risk of urogenital schistosomiasis.
Abbreviations
CDC: Center for Disease Control; NTD: Neglected Tropical Disease; HIV: Human Immunodeficiency Virus; MDA: Mass Drug Administration.
Introduction
Schistosomiasis is a persistent parasitic disease caused by a trematode parasite of Schistosoma [1]. In the subtropical and tropical regions of the Caribbean, South America, Asia and Africa, the infection is the second most prevalent parasitic infection, with approximately 779 million people at risk of developing the disease [2]. According to a 2015 Center for Disease Control (CDC) study in sub-Saharan Africa, schistosomiasis causes 224 million malignancies and results in 280,000 deaths per year, the majority of which occur in rural areas [3]. Furthermore, schistosomiasis predominantly affects low-income populations worldwide but is considered a neglected tropical disease (NTD) despite its prevalence [4]. Although six Schistosoma species cause schistosomiasis worldwide, intestinal schistosomiasis and urogenital schistosomiasis are the primary schistosomiasis caused by Schistosoma mansoni and Schistosoma haematobium, respectively [5].
In Ghana, urogenital schistosomiasis is endemic and causes significant morbidities due to its widespread distribution [6]. The disease is spread through water contact caused by human activities with the snail (intermediate host) of the genus Bulinus [7]. Schistosomiasis is a significant work-related risk for developing agricultural, fisheries, mining, and irrigation projects. In addition, everyone is at risk, but especially children, who become infected while doing household chores such as fetching water for cooking, drinking, washing, and bathing [8]. Also, the high prevalence of schistosomiasis infections was associated with poor sanitation, lack of access to safe drinking water, poverty, and lack of knowledge about the risk of infection, especially in rural areas where multiple infections are common [9].
Studies conducted in Ghana and other sub-Saharan African countries show that schistosomiasis is responsible for developing hematuria, dysuria, and hydronephrosis, with children presenting the most significant risk of infection [10]. Urogenital schistosomiasis is also associated with Katayama fever/Katayama syndrome, characterized by hypersensitivity responses, including serum sickness due to immune complex formation, resulting in pyrexia, fatigue, aches, lymphadenopathy [4, 7]. The existence of S. haematobium eggs in both the urinary and genital systems of males and females causes painful urination, abnormal ejaculation, prostatitis, haematospermia, abnormal swelling of genital organs, epididymitis, menstrual disorders, uterine enlargement, cervicitis, and infertility [11]. Several studies have also demonstrated the association between urogenital schistosomiasis and human immunodeficiency virus (HIV) infection. Thus, females with urogenital schistosomiasis (FSG) are more likely to have HIV infection by increasing HIV receptors in FSG lesions and damage of the cervical mucosa and vaginal that accelerate the progression of HIV infection [12, 13].
Other health effects associated with the disease include the possibility of anaemia, nutrient deficiencies, stunted growth in children, portal hypertension, bladder cancer, and impaired cognitive development in individuals suffering from the infection [9, 14, 15]. WHO, working to combat schistosomiasis in humans, identifies mass drug administration (MDA) as a critical intervention by administering a single dose of 40 mg/kg to school children, intending to eliminate schistosomiasis by 2025 [16]. An estimated eleven million individuals in the country require preventive chemotherapy for schistosomiasis annually, out of which an estimated 4.7 million are school-age children. However, only 1.4 million received preventive chemotherapy in Ghana. Research carried out shows that MDA intervention as a stand-alone schistosomiasis control campaign is not ineffective in curbing the morbidities caused by the disease and reducing disease prevalence [17, 18].
Studies have suggested that inadequate population awareness of schistosomiasis transmission, signs and symptoms, and prevention measures may lead to poor control practices that perpetuate the disease [17], [19]. For instance, Odhiambo and colleagues showed in their study that some communities perceived schistosomiasis as a sexually transmitted disease [20]. Inadequate knowledge, poor attitudes and control practices, and misconceptions about the disease may be responsible for disease prevalence [21, 22]. Therefore, monitoring and assessing the prevalence and intensity of the disease, as well as community knowledge, attitudes, and control practices, are critical to developing long-term control strategies and assisting in changing behaviours that reduce the risk of infection and improve the quality of disease policy decisions.
We conducted this study to fill the gap by assessing knowledge (K), attitude (A), and control practices (P) regarding urogenital schistosomiasis in rural communities would improve decisions on policy formation towards intensified programs to mitigate the impact of urogenital schistosomiasis within the area.
Methodology
Study Design
This cross-sectional study assessed knowledge, attitude, and control practices (KAPs) regarding schistosomiasis. It examined the prevalence of urogenital schistosomiasis and its risk factors among four rural communities within the Atiwa West District.
Description of the Study Area: The study was conducted in the Eastern Region of Ghana, particularly in the Atiwa West District. Atiwa West District was part of Atiwa District until partition on March 15, 2018 [23]. Atiwa West District has a land area of 656 km² and an estimated population of 61,219 of the region’s 2.9 million residents, of which 51.1% are men and 48.9% are women. Of the total population of Atiwa West District, 33.3% live in urban areas, while 66.7% live in rural and remote areas [24]. The Atewa Range Forest Reserve, which covers an area of approximately 23,663 hectares, is home to the Atiwa West District. The reserve has several natural mineral resources (such as gold, bauxite, etc.), with three main rivers, namely Ayensu River, Densu River and Birim River, surrounding and flowing through the reserve. Many of Ghana’s largest populations live in surrounding communities, and these rivers serve as their primary source of industrial and industrial water [25]. The majority of the residents are engaged in agriculture. The district has substantial agricultural resources for cultivating cocoa, oil palm, coffee, citrus, and food crops such as cassava, maize, plantain, yam, and cocoyam. Large-scale manufacturing activities dominate the industrial sector, including gari processing, oil palm extraction, small-scale mining, sawmills, and bakeries.
Study Population and Sample Size: Four communities have been classified as schistosomiasis hotspots based on Kwabeng Health Directorate health records. The report on neglected tropical diseases in the district suggested that these communities may be endemic for urogenital schistosomiasis [26, 27]. The study population comprised household heads from Kwabeng, Asamama, Afrofufu and Abomosu communities. In the study, a household head was defined as a person who carried out the economic and social tasks of a household and was selected for the study because they make important decisions regarding the health of family members. Slovin formula was used to determine the study sample size [28]. A population (N) of 61,219 inhabitants within the district and a margin of error (e) 5% (0.05) was considered and accepted when calculating the study population [24].
/1 2 n N Ne = + Where: n = sample size N = Population size = 61219 e = Margin error (5%) = 0.05 n = 61219 1+ [61219 × (0.05)2] n = 397.40 n ≈ 397 The calculated sample size is 397. However, considering a non-response rate of 1%, we estimated a minimum sample size of 400 participants to participate in the study. Therefore, 400 household heads were enrolled in the study.
Sampling Technique: Study participants were selected using convenient and simple random techniques. These techniques were chosen because they ensure rapid data collection, prevent bias, and allow the researcher to make inferential statistics correctly.
Sample/Data Collection: Quantitative data collection methods were used using structured, self-administered questionnaires developed by reviewing the international, national and scientific literature on urogenital schistosomiasis [29]. Questionnaires and personal interviews were used to collect data from respondents. The questionnaire included open-ended and closed-ended questions about KAP, written in English and interpreted for participants who could not read. The validated survey questionnaire provided information ranging from participants’ sociodemographic characteristics to general awareness of urogenital schistosomiasis, including knowledge, attitudes, control practices, treatment, prevention, and control strategies. All respondents who had problems completing the questionnaire were helped. During the household survey, only one adult per household was interviewed, and clean 30-mL universal screw-top plastic bottle containers for providing urine samples were provided to children between the ages of 6 and 15 years available in the selected household who agreed to participate. However, children were asked to warm up with some aerobic exercise before sampling. During the study period, samples were only taken randomly from 8:00 a.m. to 10:00 a.m. The samples were immediately transported to Kwabeng Health Center for further processing and testing. Children who had taken anti- schistosome medication (praziquantel) in the past 14 days before or during the study were excluded. Data Management and Analysis: Microsoft Excel 2016 and Statical Package for Social Sciences (SPSS) software, version 29.0.1, were used for data entry and analysis and expressed in percentages, tables, and charts for the different variables. In the logistic regression analysis, variables with a P value less than 0.05 were employed to clarify whether there was any statistically significant correlation between predictor and result variables. The strength of the association was ultimately determined using the odds ratio (OR) with a 95% confidence interval (CI).
Ethical Consent Consideration: This study was approved by the Koforidua Technical University and Human Research Ethics Committee. All ethical principles and considerations related to human research were strictly adhered to and implemented. Before inclusion in the study, written or verbal consent was obtained from the study participant. Sample Preparation: Urine samples collected from participants were transported to the Kwabeng Health Center to examine Schistosoma haematobium ova/eggs. The urine samples were left to settle for about ten minutes on the bench. Each bottle contained roughly 30 millilitres after the urine samples were disposed of. Macroscopy and biochemistry examinations were performed on each urine sample and documented in a urine routine examination worksheet. In addition, a microscopic examination was performed using 10x and 40 objectives to identify and count parasites [30].
Results
Sociodemographic Characteristics
This study involved 400 participants in total. Of the respondents, men comprised the majority (54%), and less than half (44.5%) were younger than 40. Only 85(21.25%) had no form of formal education. Most (56.50%) respondents had at least an elementary level of education. Of 400 participants, 317, representing almost 80%, were married. Additionally, 89.5% were Christians. Most participants have spent more than ten years living in their respective communities. Most respondents rely on piped water (54.25%), with the majority (219) and 54.25% being farmers.
| Sociodemographic Variables | Category | n | % |
|---|---|---|---|
| Sex | Male | 216 | 54 |
| Female | 184 | 46 | |
| Age of respondents | ≥40years | 222 | 55.5 |
| <40 | 178 | 44.5 | |
| Occupation | Mining | 46 | 11.5 |
| Farming | 219 | 54.75 | |
| Civil servant | 23 | 5.75 | |
| Trader | 90 | 22.5 | |
| Source of water | Hand-dug well | 64 | 16 |
| Lake/River | 49 | 28.25 | |
| Borehole | 70 | 17.5 | |
| Pipe born | 217 | 54.25 |
Table 1: Sociodemographic Characteristics of the Participants in the Study.
n=number of participants, %= percentage Table 1: Sociodemographic Characteristics of the Participants in the Study.
Urogenital Schistosomiasis Prevalence and Distribution
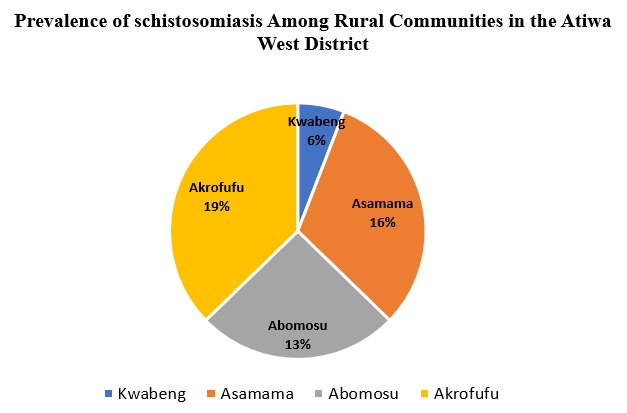
The table provides data on the prevalence of schistosomiasis among study participants in four different communities. In each community, the number of male and female participants testing positive for Schistosoma haematobium eggs was recorded. The total number of individual cases in all communities was 51 out of 350 study participants, corresponding to an overall prevalence of approximately 14.57%. In contrast, 31 men and 20 women, representing 60.8% and 39.2%, respectively, suffered from urogenital schistosomiasis. In many tropical regions, urogenital schistosomiasis, caused by the parasitic worm Schistosoma haematobium, poses a severe health threat. The data suggests that the disease occurs to varying degrees in all four communities, with most cases reported in Akrofufu.
| Community | Participants | Isolated in Male (n) | Isolated in Female (n) | Total Schistosoma haematobium egg/ova isolated Microscopy | Overall Prevalence of Schistosomiasis |
|---|---|---|---|---|---|
| Kwabeng | 50 | 3 | 0 | 3 | |
| Asamama | 100 | 9 | 7 | 16 | |
| Abomosu | 100 | 8 | 5 | 13 | |
| Akrofufu | 100 | 11 | 8 | 19 | |
| Total | 350 | 31 | 20 | 51 | 14.57% |
Table 2: Urogenital Schistosomiasis Prevalence in Study Participants (n = 350).
n=number of participants, %= percentage Table 2: Urogenital Schistosomiasis Prevalence in Study Participants (n = 350).
| Variables | n | % |
|---|---|---|
| Knowledge of Schistosomiasis | ||
| Heard of schistosomiasis | ||
| Yes | 338 | 85 |
| No | 62 | 16 |
| At risk of urogenital Schistosomiasis | ||
| Children | 117 | 29 |
| Adults | 42 | 11 |
| Aged | 10 | 2.5 |
| Everyone is at risk | 231 | 58 |
| Transmission | ||
| Playing with soil | 11 | 2.8 |
| Dirty hands | 7 | 1.8 |
| Eating contaminated food | 19 | 4.8 |
| Swimming/playing in infested water | 210 | 53 |
| Drinking infected water | 91 | 23 |
| Eating snails | 1 | 0.3 |
| Do not know | 61 | 15 |
| Signs and symptoms of urogenital schistosomiasis | ||
| Abdominal pain | 17 | 4.3 |
| Painful urination | 128 | 32 |
| Haematuria (Blood in urine) | 200 | 50 |
| Fever | 6 | 1.5 |
| Itching | 8 | 2 |
| Diarrhoea | 9 | 2.3 |
| Do not know | 28 | 7 |
| Others | 4 | 1 |
| Cause of blood in urine | ||
| Menarche | 30 | 7.5 |
| Malaria | 18 | 4.5 |
| Urogenital Schistosomiasis | 156 | 39 |
| Sexually transmitted disease (STD) | 61 | 15 |
| Witchcraft | 8 | 2 |
| Do not know | 127 | 32 |
| Risk factors | ||
| Body contact with an infected person | 45 | 11 |
| Contact with infested river/dam/canal | 221 | 55 |
| Walking across water barefooted | 25 | 6.3 |
| Eating unwashed fruit and vegetables | 14 | 3.5 |
| Do not know | 95 | 24 |
| How to reduce the risk of reinfection | ||
| Maintaining good personal hygiene | 76 | 19 |
| The use of herb | 28 | 7 |
| Avoid contact with infested water | 114 | 29 |
| Seeking treatment from a health facility | 150 | 38 |
| Prayers | 13 | 3.3 |
| Do not know | 19 | 4.8 |
| Attitude Regarding Urogenital Schistosomiasis | ||
| Schistosomiasis/bilharzia is a severe disease | ||
| Strongly agree | 189 | 47 |
| Agree | 203 | 51 |
| Strongly disagree | 8 | 2 |
| Do you believe the disease can be prevented? | ||
| Strongly agree | 171 | 43 |
| Agree | 219 | 55 |
| Disagree | 0 | 0 |
| Strongly disagree | 10 | 2.5 |
| Schistosomiasis/bilharzia part of growing up | ||
| Strongly agree | 35 | 8.8 |
| Agree | 170 | 43 |
| Disagree | 191 | 48 |
| Strongly disagree | 4 | 1 |
| It doesn’t matter whether you urinate or defecate in water | ||
| Strongly agree | 38 | 9.5 |
| Agree | 65 | 16 |
| Disagree | 164 | 41 |
| Strongly disagree | 133 | 33 |
| Children can swim and play in infested water | ||
| Strongly agree | 42 | 11 |
| Agree | 92 | 23 |
| Disagree | 120 | 64 |
| Strongly disagree | 146 | 37 |
| It is important to screen for schistosomiasis/bilharzia periodically | ||
| Strongly agree | 156 | 39 |
| Agree | 183 | 46 |
| Disagree | 51 | 13 |
| Strongly disagree | 10 | 2.5 |
| It is important to take anti-bilharzia deworming tablets | ||
| Strongly agree | 184 | 46 |
| Agree | 168 | 42 |
| Disagree | 44 | 11 |
| Strongly disagree | 4 | 1 |
| Should I visit the hospital when blood is in my urine? | ||
| Strongly agree | 267 | 67 |
| Agree | 107 | 27 |
| Disagree | 18 | 4.5 |
| Strongly disagree | 8 | 2 |
| Control Practices Regarding Urogenital Schistosomiasis | ||
| How often do you wear shoes when walking along the river/dam bank? | ||
| Always | 208 | 52 |
| Sometimes | 137 | 34 |
| Never | 55 | 14 |
| How often do you rely on water from rivers/dams for domestic use? | ||
| Always | 48 | 12 |
| Sometimes | 209 | 52 |
| Never | 143 | 36 |
| How often do you engage in activities that expose you to contact with infested water? | ||
| Always | 43 | 11 |
| Sometimes | 232 | 58 |
| Never | 125 | 31 |
| How often do you use protective waterproof clothes or boots when in contact with the water bodies? | ||
| Sometime | 58 | 15 |
| Never | 135 | 34 |
| How often do you swim or bathe in a river, dam, or canal? | 207 | 52 |
| Always | ||
| Sometimes | 13 | 3.3 |
| Never | 214 | 54 |
| How often do you urinate/defecate into or around water bodies? | 173 | 43 |
| Always | ||
| Sometimes | 9 | 2.3 |
| Never | 128 | 32 |
| Have you ever passed blood in urine? | 263 | 66 |
| Always | ||
| Sometimes | 6 | 1.5 |
| Never | 55 | 14 |
| 339 | 85 | |
| Attend a health facility when I urinate blood | ||
| Always | 76 | 19 |
| Sometimes | 66 | 17 |
| Never | 258 | 65 |
Table 3: Study Population’s Level of knowledge, perceptions and practices regarding urogenital schistosomiasis.
n=number of participants, %= percentage Table 3: Study Population’s Level of knowledge, perceptions and practices regarding urogenital schistosomiasis.
Knowledge of Participants about Urogenital Schistosomiasis
Table 3 displays the findings of the participants’ knowledge regarding the signs and symptoms, prevention, and transmission of schistosomiasis. 338 (84%) of the respondents were the majority who had heard of schistosomiasis. The majority, 68.0% (231/400), stated that “everyone is at risk.” Additionally, 200 (50%) reported hematuria, 17 (4.25%) abdominal pain and 128 (32.00%) reported pain during urination; 7% did not know any symptom. The study participants lacked knowledge about the cause of hematuria, and 31.75% (127/231) of the respondents did not know the cause. Additionally, 52.50% reported that the disease is contracted by swimming/playing with contaminated water, while 91% (22.75/400) reported drinking contaminated water. Regarding knowledge about schistosomiasis prevention, 71.36% (284/400) reported avoiding swimming in river/dam water. 17.34% did not know any preventative measures.
Attitude Towards Urogenital Schistosomiasis
Of the 400 participants with knowledge of schistosomiasis, 98% (392/400) strongly agreed or agreed that schistosomiasis was a severe disease. 97% (390/400) strongly agree or agree that schistosomiasis can be prevented, and many respondents (47.75% (191/400) disagree that schistosomiasis is a part of growing up. Surprisingly, 25.75% (103/400) of respondents strongly agreed or agreed: “It doesn’t matter whether you urinate or defecate in water.” 84.75% (339/400) considered regular screening for schistosomiasis crucial. In addition, 30.5% (122/400) believed that urogenital schistosomiasis was on the rise, while 93.5% (374/400) described the hospital as health-seeking for treating urogenital schistosomiasis.
Treatment, Prevention, and Control of Urogenital Schistosomiasis
Table 4 shows the results of treatment, prevention, and control of genitourinary disease of the respondents with schistosomiasis. Regarding treatment response, the results showed that a significant number of participants (62.50% (250/400)) knew that there is a drug to treat infected people, and 25.50% (102/400) of respondents reported taking praziquantel in the past six months. While 48.75% (15/400) participated in the schistosomiasis control program, 46 (11.50%) reported a praziquantel-treated child in their household. Regarding prevention, even 50.00% (200/400) of respondents stated that health education could be used to prevent and control schistosomiasis/schistosomiasis. Interestingly, 9.50% (38/400) of participants could not name a preventive measure.
| Variables | n | % |
|---|---|---|
| Do you know there is a drug that treats infected persons? | ||
| Yes | 250 | 62.5 |
| No | 150 | 37.5 |
| Did you take Praziquantel in the last six months? | ||
| Yes | 102 | 25.5 |
| No | 298 | 74.5 |
| Have you or your children participated in the schistosomiasis control programme? | ||
| Yes | 195 | 48.75 |
| No | 205 | 51.25 |
| Did you have any child in your household affected treated with Praziquantel? | ||
| Yes | 46 | 11.5 |
| No | 354 | 88.5 |
| Do you want children to be treated with praziquantel during mass drug administration (MDA) or a treatment campaign? | ||
| Yes | 332 | 83 |
| No | 68 | 17 |
| What should be done to prevent and control schistosomiasis/bilharzia in your region? | ||
| Health education | 200 | 50 |
| MDA of praziquantel to all children | 43 | 10.75 |
| Provision of safe tap water | 105 | 26.25 |
| Use of latrines | 14 | 3.5 |
| Don’t know | 38 | 9.5 |
Table 4: Treatment, Prevention, and Control of Urogenital Schistosomiasis among Participants (n=400).
n=number of participants, %= percentage Table 4: Treatment, Prevention, and Control of Urogenital Schistosomiasis among Participants (n=400).
Discussion
According to the WHO, mass drug administration (MDA) is a crucial intervention for effectively controlling schistosomiasis, which has called for international efforts to eradicate schistosomiasis in humans by 2025 [16]. However, research has shown that MDA may be critical but not sufficient for controlling urogenital schistosomiasis because the prevalence and intensity of human schistosomiasis persist after a mass chemotherapy campaign. Against this backdrop, the current research assesses knowledge, attitudes, and control practices in rural communities in Atiwa West District.
The study results showed a high level of awareness of urogenital schistosomiasis among participants, indicating that residents of these communities were familiar with the disease, possibly due to the endemic area previously targeted by a schistosomiasis control program. These findings are consistent with the results in Gambia and Tanzania, which reported high levels of respondents’ awareness of schistosomiasis [31] and [22]. However, their attention to disease transmission, risk factors, symptoms, prevention, and control was moderate, indicating that simply hearing about the disease is not enough to curb the morbidities caused by the disease. For instance, only 39% of respondents know about the causes of urogenital schistosomiasis; surprisingly, 15.25% of respondents describe blood in the urine as a sexually transmitted disease, with 31.25% not knowing about its cause, which was also reported from other studies [32, 33, 34]. In addition, most participants (52.50%) responded that swimming in contaminated water (river/ lake) triggered disease transmission. Surprisingly, going to the lake or river (52.25%) was a common practice given participants’ dependence on domestic and economic work such as swimming, farming, fishing, mining, washing, cooking, and bathing.
The study found that the mean knowledge level of respondents could be due to participants’ lower level of education and inadequate health education and promotion campaigns. Nevertheless, the study established education of household heads, occupation, water source, and sanitation showed that socioeconomic conditions are often strongly associated with schistosomiasis. This finding aligns with a survey by Sacolo and colleagues, who attributed the decline in schistosomiasis knowledge to lower levels of education in the community [35].
The study also recorded good attitudes among participants, but 25.75% and 33.50% urinating or defecating in water and swimming or fishing, respectively, would enhance disease transmission or be at risk of schistosomiasis. Studies in Swaziland and southern Mauritania observed similar findings about participants’ attitudes toward schistosomiasis [36, 37]. The availability of recreational centres for children could lower their exposure to swimming or bathing in unsafe water sources, limiting disease transmission. Other studies also suggested that providing a pit latrine can reduce the likelihood of urination in freshwater [38, 17, 18]. Suppose these measures are not included in control strategies. In that case, there is a risk that people will develop negative attitudes towards the control program, as in Ghana and northwestern Uganda [39, 40]. Moreover, most participants assumed that the severity of the infection was due to someone excreting blood in their urine and believed the disease could be prevented compared to a previous study in Yemen [17]. Although respondents’ control practices are generally fair, many participants with poor control practices may still be at risk of infection. Most of their risky behaviours were related to their water contact habits, including dependence on bodies of water, walking barefoot across bodies of water, and swimming or bathing in infested waters. Attributable to inadequate boreholes and tap water in the communities, and for time management purposes, the residents prefer the stream, lake, dams, and rivers for their household activities, relinquishing the threat this exposure poses to their health. Moreover, the significantly higher risk of infection among males compared to females when walking across water bodies barefooted highlights gender disparities in exposure and susceptibility to infection, emphasizing the need for gender-sensitive interventions. High rates of water contact behaviours were also observed in other studies in Tanzania and Ghana [21, 30].
The findings of this study align with previous research indicating that occupational exposure to water sources is a significant risk factor for urogenital schistosomiasis infection [41]. Similarly, the observed higher risk of infection among individuals engaged in water-related occupations is consistent with the notion that direct contact with infested water increases the likelihood of parasite transmission [42]. These findings emphasize the importance of public health measures, including providing access to clean water sources and informing the community about safe control practices to reduce the risk of infection. According to the study, there is still an incidence of urogenital schistosomiasis in children, with a prevalence of 14.57%. The current study recorded a lower prevalence rate than previous studies conducted in the country [39, 43].
In contrast, the average knowledge, positive attitudes, and fair control practices with alarming prevalence reported in the present study suggest that the MDA intervention is insufficient to control and eradicate urogenital schistosomiasis, although the communities involved in the control program through mass chemotherapy. This highlights the importance of health education and promotion programs as an integral part of disease control strategies. Health education should foster an understanding of schistosomiasis within communities and encourage using protective clothing or boots when in contact with water from a river, dam, or canal. This will also help improve children’s and community knowledge, and influencing positive control practices will reduce reinfection rates after mass drug administration. Also, encouraging each household to adopt a one-latrine policy will help reduce the passing of stool or urine in the bush or water source. Therefore, the success of MDA depends on effective health education and promotion campaigns sensitization, as well as public health measures combining water, sanitation, and hygiene and providing access to clean water sources and community engagement in the schistosomiasis control program to influence behavioural changes to reduce the risk of infection. In addition, snail control and eradication by treating infested water sources are critical and must be carried out simultaneously with MDA in communities affected by schistosomiasis [41]. For instance, snail removal and health education in China and Egypt have significantly reduced schistosomiasis transmission, prevalence, and morbidity [42, 44]. Suppose the results of this study are translated to rural communities in Atiwa West District and other endemic communities. In that case, they will improve the planning, implementation, monitoring and evaluation of schistosomiasis interventions in the region.
Conclusion
In summary, the study revealed that heads of households in the Atiwa West District have fair control practices, positive attitudes, and moderate levels of knowledge regarding urogenital schistosomiasis transmission. To overcome the moderate level of expertise about urogenital schistosomiasis found in the study, intensive health education at both community and school levels is needed. Intensifying community health education and promotion programs and utilizing local media to educate residents about the disease’s symptoms, transmission, and prevention are vital for raising awareness and would aid in changing behaviours that lower the risk of exposure and significantly enhance the quality of decisions made regarding policy formation for more intensive programs that may lessen the effects of urogenital schistosomiasis. Furthermore, there is a dire need for the government, through the Ghana Water Company, to provide clean and safe water sources for vulnerable communities. Appropriate stakeholders should ensure the construction of adequate latrines within communities, foster household pit latrines, and ensure proper sanitation and hygiene. These could have a significant impact on their water contact behaviours. In addition, community health workers should be trained in schistosomiasis early detection and frontline health facilities should be equipped with diagnostics and treatment capacity at a subsidized cost, partnering with NGOs. All school-age children should participate in mass chemotherapy as this will help treat the infected individuals and reduce the spread of the disease. The role of the MDA must be played to its fullest in this regard.
Recommendations
Inculcating schistosomiasis control program education into the school curriculum and training teachers will help students learn preventive measures. Educating children about schistosomiasis will broaden their understanding, improve their attitude, and ensure good practice. In addition, assistance with construction and using latrines to reduce passing stools or urine in the bush or water is recommended. Finally, focus groups may be used in future research to assess people’s opinions about urogenital schistosomiasis knowledge, attitudes, and control practices in the region and other endemic areas.
Conflict of Interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of this article.
References
-
Colley DG, Bustinduy AL, Secor WE, King CH (2014) Human schistosomiasis. In: The Lancet. Elsevier BV, pp: 2253-2264.
-
Omedo M, Ogutu M, Awiti A, Musuva R, Muchiri G, et al. (2014) The effect of a health communication campaign on compliance with mass drug administration for schistosomiasis control in Western Kenya SCORE project. American Journal of Tropical Medicine and Hygiene 91(5): 982-988.
-
Yawson AA, Hotorvi C, Oduro EA, Tawiah PA, Quarshie SS, et al. (2019) Prevalence and Associated Factors of Urinary Schistosomiasis among Basic School Children in the Akyemansa District, Ghana. Asian Journal of Medicine and Health 1-10.
-
WHO (2022) WHO Guideline on control and elimination of human schistosomiasis. Geneva.
-
Kokaliaris C, Garba A, Matuska M, Bronzan RN, Colley DG, et al. (2022) Effect of preventive chemotherapy with praziquantel on schistosomiasis among school- aged children in sub-Saharan Africa: a spatiotemporal modelling study. Lancet Infect Dis 22(1): 136-149.
-
Anyan WK, Dyra CE, Price M, Naples JM (2020) Assessment of Dual Schistosome Infection Prevalence from Urine in An Endemic Community of Ghana By Molecular Diagnostic Approach 53.
-
Aula OP, Manus DPM, Jones MK, Gordon CA (2021) Schistosomiasis with a focus on Africa. Tropical Medicine and Infectious Disease 6(3): 109.
-
Larbi RT (2013) Regional Institute for Population Studies University of Ghana Exploring the Influence Of Climate Variability/ Change on the Prevalence of Schistosomiasis in Ghana: A Study of the Ga Districts.
-
Geleta S, Alemu A, Getie S, Mekonnen Z, Erko B (2015) Prevalence of urinary schistosomiasis and associated risk factors among Abobo Primary School children in Gambella Regional State, southwestern Ethiopia: A cross sectional study. Parasit Vectors 8(1).
-
Maseko TSB, Mkhonta NR, Masuku SKS, Dlamini SV, Fan CK (2018) Schistosomiasis knowledge, attitude, practices, and associated factors among primary school children in the Siphofaneni area in the Lowveld of Swaziland. Journal of Microbiology, Immunology and Infection 51(1): 103-109.
-
Ribeiro AR, Luis C, Fernandes R, Botelho MC (2019) Schistosomiasis and Infertility: What Do We Know?. Trends in Parasitology, Elsevier Ltd 35: 964-971.
-
Kleppa E (2015) HIV susceptibility related to HIV target cells and cervical ectopy. A study of young South African women living in a rural area endemic of urogenital schistosomiasis [Internet]. Oslo, Norway.
-
Nemungadi TG, Kleppa E, Dam GJV, Corstjens PLAM, Arachchige HNG, et al. (2022) Female Genital Schistosomiasis Lesions Explored Using Circulating Anodic Antigen as an Indicator for Live Schistosoma Worms. Frontiers in Tropical Diseases 3.
-
Jokonya TLM, Naicker T, Jokonya L, Midzi H, Vengesai A, et al. (2020) Association of Schistosoma haematobium infection morbidity and severity on co-infections in pre-school age children living in a rural endemic area in Zimbabwe. BMC Public Health 20(1): 1570.
-
Zaghloul MS, Zaghloul TM, Bishr MK, Baumann BC (2020) Urinary schistosomiasis and the associated bladder cancer: update. Journal of the Egyptian National Cancer Institute. Springer Science and Business Media Deutschland GmbH 32(1): 44.
-
Sady H, Al-Mekhlafi HM, Atroosh WM, Al-Delaimy AK, Nasr NA, et al. (2015) Knowledge, attitude, and practices towards schistosomiasis among rural population in Yemen. Parasit Vectors 8(1): 436.
-
Angelo T, Kinung’Hi SM, Buza J, Mwanga JR, Kariuki HC, et al. (2019) Community knowledge, perceptions and water contact practices associated with transmission of urinary schistosomiasis in an endemic region: A qualitative cross-sectional study. BMC Public Health 19(1): 703.
-
Odhiambo GO, Musuva RM, Atuncha VO, Mutete ET, Odiere MR, et al. (2014) Low Levels of Awareness Despite High Prevalence of Schistosomiasis among Communities in Nyalenda Informal Settlement, Kisumu City, Western Kenya. PLoS Negl Trop Dis 8(4): e2784.
-
Munisi DZ, Buza J, Mpolya EA, Angelo T, Kinung’Hi SM (2017) Knowledge, attitude, and practices on intestinal schistosomiasis among primary schoolchildren in the Lake Victoria basin, Rorya District, north-western Tanzania. BMC Public Health 17(1): 731.
-
Yohana C, Kinung’hi SM, Nyundo BA, Rambau PF, Bakuza JS (2022) Knowledge, Attitudes and Practices on Urinary Schistosomiasis-Related Morbidity among Communities in Itilima District, Tanzania. Tanzania Journal of Science 48(4): 875-885.
-
WHO (2012) A roadmap for implementation accelerating work to overcome the global impact of neglected tropical diseases a roadmap for implementation. Geneva, Switzerland.
-
Dawaki S, Al-Mekhlafi HM, Ithoi I, Ibrahim J, Abdulsalam A, et al. (2016) Prevalence and risk factors of schistosomiasis among Hausa communities in Kano state, Nigeria. Rev Inst Med Trop Sao Paulo 58: 54.
-
Atiwa West District (2021) Composite Budget for 2021- 2024 Programme Based Budget Estimates.
-
GSS (2022) Administrative Map of Ghana. Accra.
-
Rapid Assessment Program (2007) Biodiversity in the Atewa Range Forest Reserve, Ghana. Arlington, USA.
-
Ghana Statistical Service (2014) Atiwa District.
-
Tetteh-Quarcoo PB, Attah SK, Donkor ES, Nyako M, Minamor AA, et al. (2013) Urinary Schistosomiasis in Children—Still a Concern in Part of the Ghanaian Capital City. Open J Med Microbiol 03(03): 151-158.
-
Naing L, Winn T, Rusli BN (2006) Practical Issues in Calculating the Sample Size for Prevalence Studies. Archives of Orofacial Sciences 1: 9-14.
-
Anyolitho MK, Poels K, Huyse T, Tumusiime J, Mugabi F, et al. (2022) Knowledge, attitudes, and practices regarding schistosomiasis infection and prevention: A mixed-methods study among endemic communities of western Uganda. PLoS Negl Trop Dis 16(2): e0010190.
-
Dassah S, Asiamah GK, Harun V, Appiah-Kubi K, Oduro A, et al. (2022) Urogenital schistosomiasis transmission, malaria and anemia among school-age children in Northern Ghana. Heliyon 8(9): e10440.
-
Barrow A, Badjie M, Touray J, Kinteh B, Nget M, et al. (2020) Knowledge, Attitude, and Practice of Provincial Dwellers on Prevention and Control of Schistosomiasis: Evidence from a Community-Based Cross-Sectional Study in the Gambia. J Trop Med 2020: 2653096.
-
Munisi DZ, Buza J, Mpolya EA, Kinung’hi SM (2016) Intestinal Schistosomiasis among Primary Schoolchildren in Two On-Shore Communities in Rorya District, Northwestern Tanzania: Prevalence, Intensity of Infection and Associated Risk Factors. J Parasitol Res 2016: 1859737.
-
Boko PM, Ibikounle M, Onzo-Aboki A, Tougoue JJ, Sissinto Y, et al. (2016) Schistosomiasisand soil transmitted helminths distribution in Benin: A baseline prevalence survey in 30 districts. PLoS One 11(9): e0162798
-
Houweling TAJ, Karim-Kos HE, Kulik MC, Stolk WA, Haagsma JA, et al. (2016) Socioeconomic Inequalities in Neglected Tropical Diseases: A Systematic Review. PLoS Neglected Tropical Diseases 10(5): e0004546.
-
Sacolo H, Chimbari M, Kalinda C (2018) Knowledge, attitudes and practices on Schistosomiasis in sub- Saharan Africa: A systematic review. BMC Infect Dis 18: 46.
-
Maseko TBS, Masuku SKS, Mkhonta NR, Dlamini SV, Fan CK (2018) Schistosomiasis knowledge, attitude, practices, and associated factors among primary school children in the Siphofaneni area in the Lowveld of Swaziland. J Microbiol Immunol Infect 51(1): 103-109.
-
Koffi AJdA, Doumbia M, Fokou G, Keita M, Koné B, et al. (2018) Community knowledge, attitudes and practices related to schistosomiasis and associated healthcare- seeking behaviours in northern Côte d’Ivoire and southern Mauritania. Infect Dis Poverty 7(1): 70.
-
Folefac LN, Nde-Fon P, Verla VS, Tangye MN, Njunda AL, et al. (2018) Knowledge, attitudes and practices regarding urinary schistosomiasis among adults in the Ekombe Bonji health area, Cameroon. The Pan African Medical Journal 29: 161.
-
Anto F, Asoala V, Adjuik M, Anyorigiya T, Oduro A, et al. (2013) Water Contact Activities and Prevalence of Schistosomiasis Infection among School-age Children in Communities along an Irrigation Scheme in Rural Northern Ghana. Journal of Bacteriology and Parasitology 4(4): 1-6.
-
Parker M, Allen T, Hastings J (2008) Resisting control of neglected tropical diseases: Dilemmas in the mass treatment of schistosomiasis and soil-transmitted helminths in north-west Uganda. J Biosoc Sci 40(2): 161- 181.
-
Adema CM, Bayne CJ, Bridger JM, Knight M, Loker ES, et al. (2012) Will All Scientists Working on Snails and the Diseases They Transmit Please Stand Up? PLoS Neglected Tropical Diseases 6(12): e1835.
-
Liu L, Yang GJ, Zhu HR, Yang K, Ai L (2014) Knowledge of, attitudes towards, and practice relating to schistosomiasis in two subtypes of a mountainous region of the People’s Republic of China. Infect Dis Poverty 3: 16.
-
Ofori MF, Peprah BO, Adukpo S, Dickson EK, Anim- Baidoo I, et al. (2020) Prevalence of Urinary and Intestinal Schistosomiasis Among Rice Framers in Asutsuare, Ghana. International Journal of Microbiology and Biotechnology 5(2): 69-73.
-
Barakat RMR (2013) Epidemiology of Schistosomiasis in Egypt: Travel through Time: Review. Journal of Advanced Research 4(5): 425-432.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda