Measuring Maternity Care Access in the United States: A Scoping Review of Maternity Care Deserts, Obstetric Service Availability, and Geographic Access
Access to inpatient obstetric services is increasingly recognized as a critical component of maternal health infrastructure; however, substantial variation exists in how maternity care access is defined and measured. This scoping review synthesized the methodological approaches used to operationalize maternity care access, maternity care deserts, labour and delivery unit closures, and geographic access to obstetric services in the United States. Literature searches were conducted in PubMed and Scopus for studies published between 2010 and 2026. Following screening and full-text review, 55 studies met the inclusion criteria and were included in the final synthesis. Hospital-based measures were the predominant approach to measuring maternity care access, appearing in 94.5% of studies, while provider-based measures were used in 52.7%. Fewer than half of the studies (41.8%) explicitly defined maternity care deserts. Geographic methodologies varied considerably, with geographic information system mapping used in 50.9% of studies, travel distance measures in 38.2%, and travel-time analyses in only 10.9%. Facility-level verification of obstetric service availability was reported in 60.0% of studies. Overall, the literature demonstrated substantial heterogeneity in definitions, data sources, geographic methodologies, and infrastructure measures used to evaluate maternity care access. Greater methodological standardization may improve comparability across studies, strengthen surveillance of obstetric infrastructure, and support more effective maternal health policy, workforce planning, and resource allocation.
Ashley Parks*, Sydney Stanley, Matthew Lazari and Andrew McCart
Introduction
Access to inpatient obstetric services is a critical component of maternal health infrastructure and an essential determinant of timely, high-quality maternity care. The availability of labour and delivery services, emergency obstetric care, and appropriately resourced maternity facilities influences where and how pregnant individuals receive care throughout pregnancy, childbirth, and the postpartum period [1, 2, 3, 4]. Over the past two decades, concerns regarding maternity care access have intensified as rural hospitals have closed, labour and delivery units have been discontinued, workforce shortages have reduced the capacity of many communities to maintain obstetric services, and hospital acquisitions have altered the availability of obstetric care in rural communities [5, 6, 7, 8, 9]. Recent evidence suggests that rural hospital acquisitions are associated with increased obstetric unit closures, reductions in local obstetric services, and worsening maternal outcomes, underscoring the importance of accurately measuring obstetric infrastructure and access. These changes have contributed to growing geographic disparities in access to maternity care and have increased attention on the distribution of obstetric resources across the United States [1, 3, 4].
As concerns regarding maternity care access have grown, researchers, policymakers, advocacy organizations, and health systems have increasingly sought to quantify and monitor access to obstetric services [2, 10, 11, 12, 13]. The concept of the maternity care desert has emerged as one of the most widely recognized frameworks for identifying communities with limited maternity care availability [10, 11, 12, 13]. National organizations, including the March of Dimes, have used maternity care desert classifications to identify underserved areas and inform policy discussions regarding maternal health infrastructure [10], [12]. At the same time, a diverse body of literature has developed that measures maternity care access using a variety of alternative approaches, including travel time and distance analyses, provider-to- population ratios, hospital service availability, workforce distribution measures, geographic information system (GIS) methodologies, and assessments of labour and delivery unit closures [1, 2, 3, 4, 14, 15, 16, 17].
Although these approaches are often discussed collectively as measures of maternity care access, they frequently capture different dimensions of access and may identify different populations as underserved [10- 13,15.16.18]. Some studies rely primarily on hospital-based indicators, such as the presence of active labour and delivery units, hospital obstetric capability, or labour and delivery unit closures. Others emphasize provider-based measures, including the availability of obstetrician-gynaecologists, certified nurse midwives, family physicians providing obstetric care, or combinations of workforce indicators. Geographic approaches likewise vary substantially, ranging from county-level maternity care desert classifications to travel time modelling, spatial accessibility analyses, and GIS- based mapping techniques. Differences also exist in the data sources used to identify obstetric services, including hospital surveys, administrative datasets, licensing databases, workforce registries, vital statistics systems, and direct facility verification.
This methodological heterogeneity presents important challenges for researchers, policymakers, and health systems seeking to understand the true extent of maternity care access. Differences in definitions, data sources, and measurement strategies may produce substantially different estimates of access, complicate comparisons across studies, and limit efforts to monitor changes in obstetric infrastructure over time. Variability in how labour and delivery unit closures, workforce shortages, and rural service erosion are identified and measured may also influence conclusions regarding the magnitude and consequences of declining maternity care availability. Because access measures are increasingly used to guide resource allocation, workforce planning, maternity care shortage designations, and policy interventions, understanding how these measures are constructed is essential.
Despite the growing literature on maternity care access, relatively little attention has been devoted to systematically synthesizing the methods used to define and operationalize access itself. Existing reviews have largely focused on maternal outcomes associated with geographic barriers to care rather than on the methodological approaches used to measure access. A comprehensive assessment of these measurement strategies is needed to identify areas of consensus, highlight inconsistencies, and inform future efforts toward greater methodological standardization.
Given the increasing use of access measures to guide policy decisions, workforce planning, and maternity care shortage designations, understanding how these measures are constructed has become increasingly important. Therefore, the purpose of this scoping review was to characterize how maternity care access has been defined and measured in the United States literature and to identify opportunities for greater methodological standardization.
Materials and Methods
Study Design
This scoping review was conducted to characterize how hospital-based obstetric access, maternity care deserts, labour and delivery unit closures, and geographic access to inpatient obstetric services have been defined and measured in the United States literature. The review was designed to identify methodological approaches, data sources, geographic techniques, and infrastructure measures used to evaluate access to maternity care. The review was guided by the methodological framework for scoping reviews described by Arksey and O’Malley and subsequent refinements to scoping review methodology. The objective was not to evaluate intervention effectiveness, but rather to map the existing evidence base and identify methodological trends and gaps in measurement approaches.
Eligibility Criteria
Studies were eligible for inclusion if they evaluated hospital-based obstetric access, maternity care deserts, labour and delivery unit closures, or geographic and infrastructure-based measures of maternity care access within the United States. Studies focused exclusively on clinical outcomes, outpatient prenatal care, educational interventions, or non-U.S. populations were excluded. Full inclusion and exclusion criteria are presented in Table 1.
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Hospital-based obstetric access studies | Clinical outcomes only |
| Maternity care deserts | Outpatient prenatal care only |
| Labor and delivery closures | Provider education/ interventions |
| Geographic/spatial access measures | Editorials/commentaries |
| US studies | Non-US studies |
| Peer-reviewed English- language studies | Conference abstracts |
Table 1: Eligibility Criteria.
Information Sources and Search Strategy
A comprehensive literature search was conducted in PubMed and Scopus to identify studies examining maternity care deserts, hospital-based obstetric access, labour and delivery unit closures, and geographic access to inpatient obstetric services in the United States. Searches were limited to English-language studies published between January 1, 2010, and June 1, 2026. The search strategy was designed around four primary concepts: (1) maternity care deserts and obstetric services, (2) hospital-based labour and delivery care, (3) geographic access and travel burden, and (4) rural obstetric service availability and closures.
The PubMed Search Strategy Utilized Included the Below Search Terms
(“maternity care desert*”[Title/Abstract] OR ((“labour and delivery”[Title/Abstract] OR obstetric*[Title/Abstract]) AND closure*[Title/Abstract]) OR (obstetric*[Title/Abstract] AND hospital*[Title/Abstract] AND access [Title/Abstract])) AND (rural [Title/Abstract] OR geographic [Title/Abstract] OR distance [Title/Abstract] OR travel [Title/Abstract]) AND (“United States”[Title/Abstract] OR US[Title/Abstract]) AND (2010:2026[pdat])
The Scopus Search Strategy Utilized Included the Below Search Terms
TITLE-ABS-KEY (“Maternity Care Desert*” OR ((“Labour and Delivery” OR Obstetric*) AND Closure*) OR (Obstetric* AND Hospital* AND Geographic)) AND TITLE-ABS-KEY (Rural OR Travel OR Distance OR Access) AND TITLE-ABS- KEY (“United States “OR US) AND PUBYEAR > 2009 Search Results from Both Databases Were Imported into Covidence Systematic Review Software for Deduplication, Screening, Full-Text Review, And Data Extraction. The Search Strategy Was Intentionally Designed to Prioritize Studies Focused on Hospital-Based Obstetric Infrastructure and Access Measurement Rather Than Maternal Clinical Outcomes Alone.
Study Selection
All records identified through the database searches were imported into Covidence for screening and review. Duplicate citations were removed before title and abstract screening. Studies judged potentially relevant were advanced to full-text review, where eligibility was assessed according to the predefined inclusion and exclusion criteria. Screening and full-text review were conducted independently by the review team, and any disagreements regarding eligibility were resolved through discussion and Consensus. The Study Selection Process and Reasons for Exclusion at the Full-Text Stage are Presented in The Prisma Flow Diagram.
Data Extraction
A standardized data extraction form was developed before full-text review to ensure consistent collection of information across studies. The extraction form was designed to capture the methodological approaches used to define, measure, and evaluate maternity care access, with particular emphasis on hospital-based obstetric services, maternity care deserts, geographic accessibility, and labour and delivery unit closures.
Information extracted from each study included publication characteristics, study design, geographic scope, and population characteristics. Additional data were collected regarding definitions of maternity care deserts and obstetric access, data sources used to identify obstetric services, geographic and spatial methodologies, infrastructure measures, workforce considerations, approaches to identifying labour and delivery unit closures, outcomes examined, and key study findings. Particular attention was given to the operationalization of access measures, including the use of hospital-based, provider-based, and combined approaches to measuring maternity care availability.
Data Synthesis
Data were synthesized using descriptive and narrative approaches. Studies were first characterized according to their design, geographic scope, and primary focus.
Subsequently, studies were grouped according to the methodological approaches used to measure maternity care access and obstetric service availability.
The synthesis focused on identifying patterns in how maternity care deserts were defined, how hospital-based obstetric access was operationalized, what data sources were used to identify active obstetric services, and how geographic accessibility was measured. Additional attention was given to methods used to identify labour and delivery unit closures, evaluate rural obstetric service erosion, and assess workforce shortages and infrastructure capacity.
Findings were summarized through narrative synthesis and descriptive tables to highlight methodological similarities, differences, and gaps across the literature. The primary goal of the synthesis was to characterize the range of approaches currently used to measure hospital- based obstetric access in the United States and to identify opportunities for greater standardization in future research.
Results
Study Selection
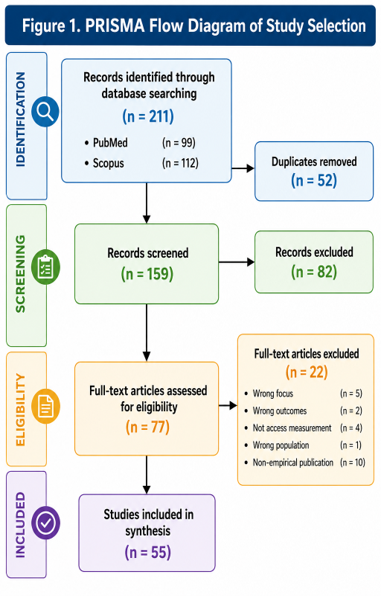
The database search identified 211 records, including 99 records from PubMed and 112 records from Scopus. After removal of 52 duplicate citations, 159 records remained for title and abstract screening. Following screening, 82 records were excluded and 77 articles underwent full-text review. Twenty-two studies were subsequently excluded because of incorrect study focus (n = 5), evaluation of outcomes without access measurement (n = 2), lack of maternity care access measurement (n = 4), incorrect patient population (n = 1), or non-empirical publication type (n = 10). A total of 55 studies met all eligibility criteria and were included in the final synthesis. The study selection process is presented in Figure 1.
Study Characteristics
The characteristics of the 55 included studies are summarized in Table 2. Cross-sectional studies represented the most common study design (25.5%), followed by GIS or spatial analyses (21.8%) and retrospective cohort studies (16.4%). Nearly one-half of all studies were national in scope (47.3%), while state-level studies accounted for an additional 18.2% of the literature. Collectively, these findings demonstrate the strong emphasis on population-level and geographically oriented approaches to evaluating maternity care access.
| Characteristic | n (%) |
| Study Design | |
| Cross-sectional | 14 (25.5) |
| GIS/Spatial analysis | 12 (21.8) |
| Retrospective cohort | 9 (16.4) |
| Ecological | 7 (12.7) |
| Mixed methods | 6 (10.9) |
| Qualitative | 5 (9.1) |
| Other | 1 (1.8) |
| Geographic Scope | |
| National | 26 (47.3) |
| State-level | 10 (18.2) |
| Multi-state | 6 (10.9) |
| Regional | 5 (9.1) |
| County-level | 5 (9.1) |
| Census tract-level | 1 (1.8) |
Table 3: Characteristics of Included Studies (n = 55).
The predominance of national and state-level analyses suggests that investigators frequently examine maternity care access as a systems-level phenomenon rather than focusing on individual facilities or local service areas [11, 12, 14, 16, 18, 19]. However, substantial variation existed in how studies defined and measured access, prompting further examination of the specific access measures employed across the literature.
Access Measurement Approaches
The methodological approaches used to operationalize maternity care access are presented in Table 3. Hospital- based measures were the dominant approach, appearing in 94.5% of studies, while provider-based measures were incorporated in approximately half of the literature (52.7%). Although maternity care deserts have become increasingly prominent in policy and research discussions, fewer than half of the studies (41.8%) provided an explicit definition of the concept. Labor and delivery unit closures were discussed in nearly nine out of ten studies (87.3%), highlighting the extent to which declining obstetric infrastructure and rural service erosion have become central themes within contemporary maternity care access research [6, 7, 8, 17, 20].
| Measure | n (%) |
|---|---|
| Hospital-based access measured | 52 (94.5) |
| Provider-based access measured | 29 (52.7) |
| Inpatient obstetric services included | 54 (98.2) |
| Maternity care desert definition provided | 23 (41.8) |
| Labor and delivery closures discussed | 48 (87.3) |
Table 2: Approaches Used to Measure Maternity Care Access.
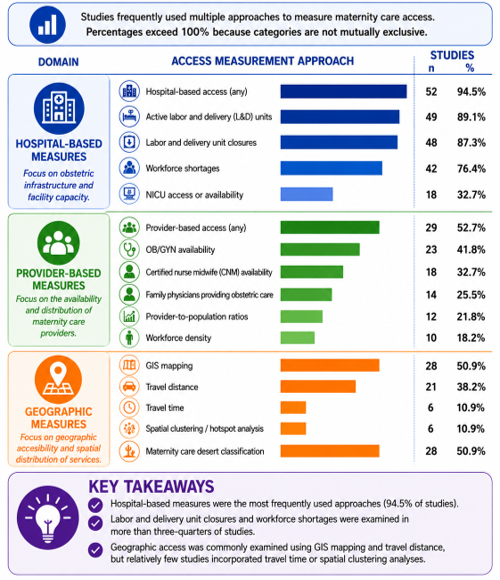
These findings suggest that hospital availability remains the primary lens through which maternity care access is evaluated [6, 18, 19]. Nevertheless, considerable variation exists regarding whether access is conceptualized through facilities, providers, geographic proximity, or combinations of these measures [10, 11, 12, 14, 15]. This variability becomes particularly apparent when examining the geographic methodologies used across studies [1, 3, 4]. To provide a broader overview of how maternity care access has been operationalized across the literature, Figure 2 summarizes the frequency of major measurement approaches identified in the included studies. Hospital-based measures were the most commonly used approaches, followed by workforce and provider-based measures. In contrast, direct measures of geographic accessibility, such as travel-time analyses and spatial clustering methods, were comparatively uncommon [1, 3, 4, 8].
Studies frequently incorporated multiple approaches to measuring maternity care access; therefore, categories are not mutually exclusive and the percentages exceed 100%. Hospital-based measures were the most used approaches, whereas travel-time and advanced spatial analytic methods were used infrequently.
As shown in Figure 2, the literature is heavily oriented toward hospital infrastructure and service availability measures [6, 10, 18, 19]. Nearly all studies incorporated hospital-based indicators [21], and a large proportion examined labour and delivery unit closures, active obstetric services, or workforce shortages [6, 14, 15, 17, 20]. Although geographic barriers to care were frequently discussed, relatively few studies incorporated direct travel-time measures. This pattern suggests that maternity care access research has focused primarily on the availability of services rather than the practical accessibility of those services from the patients’ perspective. The substantial difference between the frequency of hospital-based measures and travel-time methodologies suggests that much of the literature evaluates service availability rather than directly measuring patient accessibility [1, 3, 4].
Geographic Methodologies
Geographic approaches to measuring maternity care access varied substantially across the included studies (Table 4). Rurality classifications were the most employed geographic measure (89.1%), followed by GIS mapping techniques (50.9%). Travel distance measures appeared in 38.2% of studies; however, only 10.9% incorporated travel-time analyses despite widespread discussion of transportation barriers and travel burden within the literature. Similarly, spatial clustering techniques were used infrequently.
| Methodology | n (%) |
|---|---|
| Rurality classification | 49 (89.1) |
| GIS mapping | 28 (50.9) |
| Travel distance measurement | 21 (38.2) |
| Travel time measurement | 6 (10.9) |
| Spatial clustering methods | 6 (10.9) |
| Measure | n (%) |
| Active labor and delivery units evaluated | 49 (89.1) |
| Workforce shortages discussed | 42 (76.4) |
| Facility-level verification performed | 33 (60.0) |
| Hospital closures evaluated | 30 (54.5) |
| NICU access discussed | 18 (32.7) |
Table 4: Geographic and Spatial Methodologies Used to Measure Access.
The relatively limited use of travel-time and advanced spatial analytic methods suggests that many studies rely on administrative or geographic classifications rather than direct measures of accessibility. Consequently, studies may identify underserved populations differently depending on the methodological approach selected. The infrastructure measures used to characterize obstetric service availability also varied considerably.
Infrastructure Measures and Closure Methodologies
Infrastructure measures used across the literature are summarized in Table 5. Most studies evaluated active labour and delivery units (89.1%), while workforce shortages were discussed in more than three-quarters of studies (76.4%). Hospital closures or labour and delivery unit closures were formally evaluated in 54.5% of studies. Notably, only 60.0% of studies reported facility-level verification of obstetric service availability. NICU access was incorporated less frequently, appearing in approximately one-third of studies.
The incomplete use of facility-level verification highlights an important methodological limitation within the literature. Researchers frequently rely on administrative datasets, workforce databases, or secondary classifications of access, yet comparatively few studies verify the ongoing availability of obstetric services directly at the facility level.
This variation contributes to broader inconsistencies in how maternity care deserts and obstetric access are defined and measured.
Definitions Of Maternity Care Deserts and Obstetric Access
To better characterize the conceptual frameworks underlying maternity care access measurement, studies were grouped according to their primary operational approach (Table 6). Definitions of maternity care deserts and obstetric access varied substantially across studies and are summarized in Table 6. Although the March of Dimes framework emerged as the most cited maternity care desert definition, alternative approaches relied on hospital availability, provider availability, travel burden, workforce density, or combinations of these measures. Some studies defined access primarily through hospital-based indicators, whereas others emphasized provider availability or geographic proximity to services.
| Access Framework | Operational Definition | Common Data Sources | Representative Studies |
|---|---|---|---|
| Maternity Care Desert Classification | Counties lacking hospitals providing obstetric services and/or maternity care providers. Most commonly based on March of Dimes criteria incorporating obstetric facilities, OB/GYNs, certified nurse midwives, and provider density thresholds. | March of Dimes, HRSA, AHRF, provider databases | Wallace, et al. [10], Ramos, et al. [22], Palmer, et al., Stoneburner, et al. [13] |
| Hospital- Based Service Availability | Presence or absence of active labor and delivery units, obstetric hospitals, or inpatient obstetric services within a geographic area. | American Hospital Association (AHA), hospital surveys, state hospital data, hospital websites | Kozhimannil, et al. [19], Radke, et al. [6], O’Hanlon, et al. [26] |
| Labor and Delivery Unit Closure Measures | Identification of communities experiencing closure or loss of labor and delivery services, often measured through closure dates, service discontinuation, or changes in hospital service offerings. | AHA data, state licensing data, hospital records, news reports | McGregor, et al. [7], Radke, et al. [6], Sullivan, et al. [20] |
| Provider-Based Access Measures | Availability or density of obstetric providers, including OB/GYNs, certified nurse midwives, family physicians, or anesthesia providers involved in maternity care. | HRSA, NPPES, AHRF, workforce surveys, professional certification databases | Tong, et al. [15], Topmiller, et al. [12], Walter, et al. [14], Vandenbroeck, et al. [16] |
| Travel Distance Measures | Access measured through distance between residence and maternity care services, often expressed as miles to nearest obstetric facility. | GIS data, Census data, hospital location databases | Hung, et al. [19], McGregor, et al. [7], Strickland, et al. [21] |
| Travel Time Measures | Access measured through estimated driving time to maternity care services or delivery hospitals. | GIS network analysis, Google Distance Matrix, road network data | Rayburn, et al. [1], Thorsen, et al. [3], Uribe-Leitz, et al. [4], Woodward, et al. [8] |
| Regionalized Care and Referral Models | Access measured through maternal transfer systems, referral networks, levels of maternal care, or availability of specialty obstetric services. | Hospital transfer databases, AHA data, referral records | Morriss, et al., Rosenbloom, et al., Kozhimannil, et al. [27] |
| Combined Infrastructure and Workforce Models | Access measured through combinations of hospital availability, provider availability, workforce capacity, and geographic access indicators. | March of Dimes, HRSA, AHA, workforce datasets | Topmiller, et al. [12], Ramos, et al. [22], Palmer, et al. |
Table 5: Conceptual Approaches Used to Measure Maternity Care Access.
Considerable variation was observed in how maternity care access was defined and operationalized across studies (Table 6). The most common approaches relied on hospital- based measures of labour and delivery service availability or maternity care desert classifications [10, 18, 19]. More recent studies increasingly adopted multidimensional frameworks that combined hospital infrastructure, provider availability, and geographic accessibility measures [11, 12, 22]. Travel distance and travel time measures were used to quantify geographic barriers to care, although travel-time analyses were comparatively uncommon [1, 3, 4]. Studies evaluating labour and delivery unit closures frequently conceptualized access as the loss of local obstetric infrastructure [6, 8, 20], whereas workforce-focused investigations emphasized provider availability and distribution [14, 15, 23]. Collectively, these findings demonstrate that maternity care access is measured using multiple distinct but overlapping conceptual frameworks, with no single standardized approach dominating the literature.
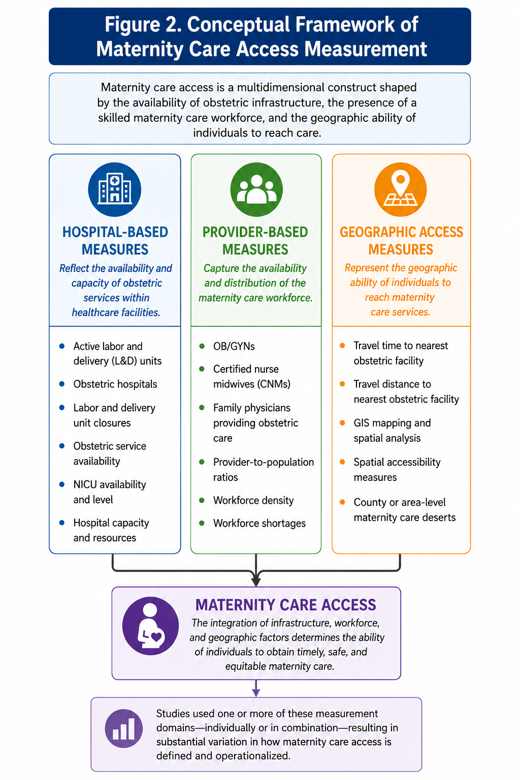
The findings suggest that contemporary maternity care access research can be broadly organized into three overlapping methodological domains: hospital-based measures, provider-based measures, and geographic access measures (Figure 3). While many studies incorporated elements from multiple domains, substantial variation existed in how these components were combined to define and operationalize access [10, 11, 12, 22]. This conceptual framework illustrates the principal approaches identified across the literature and highlights the multidimensional nature of maternity care access measurement.
As illustrated in Figure 3, the literature conceptualizes maternity care access through three primary methodological domains: hospital-based measures, provider-based measures, and geographic access measures [1, 14, 19]. While individual studies frequently incorporated elements from more than one domain, substantial variation existed in the relative emphasis placed on infrastructure, workforce, and geographic accessibility [10, 12, 22]. The lack of a standardized framework integrating these dimensions contributes to the methodological heterogeneity observed across the literature and highlights an important opportunity for future standardization efforts.
Methodological Gaps in Maternity Care Access Measurement
Several methodological gaps emerged across the included studies. Fewer than half of the studies provided an explicit definition of a maternity care desert, and substantial variation existed in the criteria used to classify underserved communities [10, 11, 12, 13]. Although hospital-based measures dominated the literature, provider-based approaches and multidimensional access frameworks were applied inconsistently [14, 15, 19, 22]. Direct measures of geographic accessibility were relatively uncommon, with only a small proportion of studies incorporating travel-time analyses despite widespread discussion of travel burden as a barrier to care [1, 3, 4, 8]. In addition, only 60% of studies reported facility-level verification of obstetric service availability [6, 18, 19]. Together, these findings highlight substantial heterogeneity in how maternity care access is measured and operationalized across the United States literature.
Discussion
This scoping review identified substantial methodological variation in how maternity care access has been defined, measured, and operationalized across the United States literature. Across 55 studies, hospital-based, provider-based, and geographic approaches were used in varying combinations, with no single framework emerging as the dominant standard for measuring maternity care access [1, 3, 5, 19]. Notably, the three primary measurement domains identified in this review, hospital-based, provider-based, and geographic approaches, often capture different dimensions of access and therefore may identify different communities as underserved [10, 11, 12, 13].
Hospital-based measures represented the dominant approach to measuring maternity care access. Measures such as the presence of active labour and delivery units, obstetric service availability, and hospital-based delivery capacity were used in nearly all included studies [5, 6, 19]. This emphasis reflects the central role of inpatient obstetric infrastructure in maternity care access; however, it also suggests that much of the literature continues to conceptualize access primarily as the presence or absence of hospital-based services.
Provider-based measures represented a second major domain of access measurement. Approximately half of the literature also incorporated provider-based measures, including the availability of obstetrician-gynaecologists, certified nurse midwives, family physicians providing obstetric care, and broader workforce capacity indicators [14, 15, 16, 23]. These findings suggest that maternity care access is increasingly recognized as a multidimensional construct that extends beyond the presence or absence of a labour and delivery unit. Collectively, these findings indicate that hospital availability remains the dominant conceptualization of maternity care access despite increasing recognition that infrastructure alone may not fully characterize access.
Geographic measurement approaches represented another area of substantial variation. Although nearly all studies acknowledged the importance of geographic barriers to care, relatively few incorporated direct travel-time analyses [1, 3, 4]. Instead, investigators frequently relied on rurality classifications, county-level designations, or other administrative geographic units as proxies for accessibility [1, 4, 5]. While these approaches are practical and readily available, they may not fully capture the lived experience of patients navigating transportation barriers, mountainous terrain, limited road networks, or regional referral systems [1, 3, 4, 8]. The limited use of travel-time methodologies suggests an important opportunity for future research to incorporate more precise measures of geographic accessibility.
The maternity care desert framework represents one of the clearest examples of integrating hospital infrastructure, provider availability, and geographic accessibility into a single measure of access. The review also demonstrated the growing influence of maternity care desert frameworks within maternal health research. While the March of Dimes classification system has become one of the most widely recognized approaches for identifying underserved communities, fewer than half of the studies explicitly defined maternity care deserts [10, 11, 12, 13]. Furthermore, studies frequently modified or supplemented existing classifications using alternative provider, infrastructure, or geographic indicators [6–8,12] [11, 12, 13, 16]. As a result, communities identified as underserved under one framework may not necessarily be classified similarly under another. This inconsistency has important implications for policy development, workforce planning, and resource allocation, particularly as maternity care access measures are increasingly used to guide state and federal maternal health initiatives [10, 11, 12, 13].
The findings also highlight ongoing challenges in measuring obstetric infrastructure. Emerging evidence further highlights the importance of accurately measuring obstetric infrastructure. Recent analyses suggest that rural hospital acquisitions are associated with increased obstetric unit closures, reduced local obstetric service availability, and increases in maternal morbidity, emphasizing that changes in obstetric infrastructure have meaningful consequences for maternal health outcomes. These findings reinforce the need for standardized methods to identify and monitor changes in hospital-based obstetric services over time [9]. More than half of the studies evaluated labour and delivery unit closures, reflecting increasing concern regarding rural obstetric service erosion and the expansion of maternity care deserts [6, 7, 17, 18, 20, 24, 25, 26]. However, only 60% of studies reported direct facility-level verification of obstetric service availability. Many investigations relied on administrative datasets, workforce registries, or secondary classifications without confirming that obstetric services remained active at the facility level [9, 16, 18] [6, 7, 17, 18, 20, 24, 27]. Given the frequency of service reductions, temporary suspensions, and closure announcements, greater consistency in facility verification could improve the accuracy and comparability of maternity care access measures.
When considered together, these findings suggest a need for greater methodological standardization in maternity care access research. Future efforts should consider integrating hospital-based, provider-based, and geographic measures into multidimensional frameworks capable of capturing the complex nature of obstetric access. Standardized definitions, transparent verification procedures, and consistent reporting practices would facilitate comparisons across studies and strengthen the evidence base used to inform maternal health policy, healthcare planning, and resource allocation. Future research should prioritize the development of standardized access measurement frameworks that integrate hospital infrastructure, provider availability, and geographic accessibility. Incorporating travel-time measures, facility- level verification, and consistent reporting standards may improve the validity and comparability of future maternity care access studies.
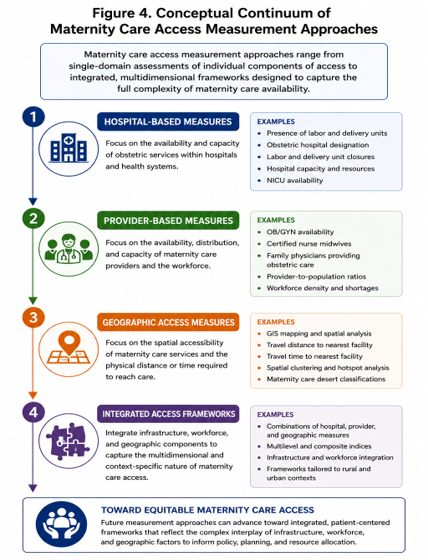
Figure 4 presents a conceptual continuum illustrating how maternity care access measures identified in the literature range from single-domain approaches focused on hospitals, providers, or geography to increasingly integrated multidimensional frameworks. While many studies continue to rely on individual measures of access, future efforts may benefit from combining infrastructure, workforce, and geographic indicators to more comprehensively characterize maternity care availability.
Policy Implications
The absence of standardized approaches to measuring maternity care access may have important policy implications. Access measures are increasingly used to inform workforce planning, maternity care shortage designations, rural hospital funding initiatives, and maternal health resource allocation [28]. Differences in how access is measured may therefore lead to different conclusions regarding which communities are underserved. Greater consistency in access measurement could improve comparability across studies and support more evidence-informed decision-making. As maternity care access measures increasingly inform maternal health policy, workforce planning, and designation of underserved communities, greater methodological consistency may improve the precision and effectiveness of interventions designed to address geographic inequities in maternity care [16, 23].
Collectively, this review suggests that maternity care access should no longer be conceptualized as a single construct measured solely through hospital availability or provider supply. Rather, access is a multidimensional phenomenon that reflects the interaction of healthcare infrastructure, workforce capacity, and geographic accessibility. Future measurement frameworks that integrate these dimensions may provide a more comprehensive understanding of obstetric service availability and better support maternal health research, policy, and planning.
Limitations
Several limitations should be considered when interpreting the findings of this review. The search was limited to studies indexed in PubMed and Scopus and published in English, which may have resulted in the exclusion of relevant studies. The review focused exclusively on studies conducted in the United States, limiting generalizability to other healthcare systems, but increasing the relevance of the review to the United States healthcare system. Since the purpose of a scoping review is to characterize the existing literature rather than evaluate intervention effectiveness, no formal assessment of study quality or risk of bias was performed. Finally, the review synthesized methodologies and definitions as reported by study authors and therefore reflects the variability inherent within the existing literature. Because data extraction and synthesis focused on methodological characteristics reported by study authors, the review was dependent on the completeness and accuracy of reporting within the included studies.
Conclusion
Maternity care access has become an increasingly important area of research, policy development, and healthcare planning in the United States. Hospital-based measures dominated the literature, while relatively few studies incorporated travel-time methodologies or standardized facility verification procedures. However, this review demonstrates that substantial variation exists in how access is defined, measured, and operationalized. Hospital- based measures remain the dominant approach, but provider- based, geographic, and multidimensional frameworks are increasingly common. Differences in definitions, data sources, geographic methodologies, and facility verification procedures contribute to inconsistent estimates of access across studies. Greater methodological standardization may improve comparability, strengthen surveillance of obstetric infrastructure, and support more effective efforts to identify and address gaps in maternity care access.
Conflict of Interest
The authors have no conflict of interest to disclose.
Funding Statement
This research received no external funding.
Acknowledgments
This review was conducted as part of a faculty-mentored research initiative designed to support student research training and the development of future work related to community-level obstetric vulnerability measurement.
Institutional Review Board Statement
Not applicable. This study involved the analysis of published literature and did not involve human subject’s research.
References
-
Rayburn WF, Richards ME, Elwell EC (2012) Drive times to hospitals with perinatal care in the United States. Obstet Gynecol 119 (3): 611-616.
-
Hung P, Henning-Smith CE, Casey MM, and Kozhimannil KB (2017) Access to Obstetric Services In Rural Counties Still Declining with 9 Percent Losing Services 2004–14. Health Aff (Millwood) 36(9):1663-1671.
-
Thorsen ML, Harris S, McGarvey R, Palacios J, Thorsen A (2022) Evaluating disparities in access to obstetric services for American Indian women across Montana. J Rural Health 38 (1): 151-160.
-
Uribe-Leitz T, Matsas B, Dalton MK, Lutgendorf MA, Moberg E, et al. (2021) Geospatial Analysis of Access to Emergency Cesarean Delivery for Military and Civilian Populations in the US. JAMA Netw Open 5(1): e2142835.
-
Kozhimannil KB, Casey MM, Hung P, Prasad S, Moscovice IS (2016) Location of childbirth for rural women: implications for maternal levels of care. Am J Obstet Gynecol 214(5): 661.e1-661.e10.
-
Radke SM, Smeins L, Ryckman KK, Gruca TS (2023) Closure of Labor & Delivery units in rural counties is associated with reduced adequacy of prenatal care, even when prenatal care remains available. J Rural Health 39 (4):746-755.
-
McGregor AJ, Hung P, Garman D, Amutah-Onukagha N, Cooper JA (2021) Obstetrical unit closures and racial and ethnic differences in severe maternal morbidity in the state of New Jersey. Am J Obstet Gynecol MFM 3(6):100480.
-
Woodward R, Mazure ES, Belden CM, Denslow S, Fromewick J, et al. (2023) Association of prenatal stress with distance to delivery for pregnant women in Western North Carolina. Midwifery 118: 103573.
-
Dranove D, Gaynor M, Geddes E (2025) Expecting Harm? The Impact of Rural Hospital Acquisitions on Maternal Health Care. Social Science Research Network Rochester NY: 5404058.
-
Wallace M (2021) Maternity Care Deserts and Pregnancy- Associated Mortality in Louisiana. Womens Health Issues 31(2): 122-129.
-
Walter G, Topmiller M, Jetty A, Jabbarpour Y (2022) Family Physicians Providing Obstetric Care in Maternity Care Deserts. Am Fam Physician 106 (4): 377-378.
-
Topmiller M, Walter G, Jetty A, Pristell C, Rankin JL, et al. (2025) The Geographic Distribution of Family Physicians Providing Maternity Care and Opportunities for Expanding Access to Care in Rural Areas. Ann Fam Med 23(4): 302-307.
-
Stoneburner A, Lucas R, Chestnut JF, Jones EE, DeMaria AL (2026) Nowhere to go: An overview of maternity care access across the U S. Semin Perinatol 50(1): 152188.
-
Walter G, Jetty A, Topmiller M, Huffstetler A (2024) Family physicians provide maternity care in and around the maternity care shortage areas, particularly rural. J Rural Health 40(4): 664-670.
-
Tong ST, Morgan ZJ, Bazemore AW, Eden AR, Peterson LE (2023) Maternity Access in Rural America: The Role of Family Physicians in Providing Access to Cesarean Sections. J Am Board Fam Med 36(4): 565-573.
-
Vandenbroeck A, Markowski JH (2025) Targeted Regulations of Abortion Providers Associated with Significant Decreases in OB-GYN Density, 1993–2021. Health Aff (Millwood) 44(8): 943-952.
-
Kozhimannil KB, Interrante JD, Admon LK, Basile Ibrahim BL (2022) Rural Hospital Administrators’ Beliefs about Safety, Financial Viability, and Community Need for Offering Obstetric Care. JAMA Health Forum 3(3): e220204.
-
Kozhimannil KB, Interrante JD, Carroll C, Sheffield EC, Fritz AH, et al. (2025) Obstetric Care Access Declined in Rural and Urban Hospitals Across US States, 2010-22. Health Aff Millwood 44(7): 806-811.
-
Hung P, Casey MM, Kozhimannil KB, Karaca-Mandic P, Moscovice IS (2018) Rural-urban differences in access to hospital obstetric and neonatal care: How far is the closest one?. J Perinatol 38(6): 645-652.
-
Sullivan EE, Gilburg ML, McDonald M, Deutchman M (2025) Innovating for success: Strengthening rural maternity care and delivery programs. J Rural Health 41(4): e70099.
-
Strickland CL, Tumin D, Harris A, Murphy H, Whiteside JL (2024) Obstetric outcomes among rural parturients across US urban and rural hospitals. Rural Remote Health 24(3): 8836.
-
Ramos SZ, McNamara IF, Alonso-Bermudez B, Has P, Werner EF, et al. (2026) Maternal care deserts and risk of maternal morbidity in term pregnancies. Am J Obstet Gynecol MFM 8(1): 101821.
-
Thumm EB, Dau KQ, Marcelle E, Smith DC (2025) The Certified Nurse-Midwife/Certified Midwife Workforce and Factors Affecting Its Growth. Obstet Gynecol Clin North Am 52 (4): 773-788.
-
Kozhimannil KB, Casey MM, Hung P, Han X, Prasad S, et al. (2015) The Rural Obstetric Workforce in US Hospitals: Challenges and Opportunities. J Rural Health 31(4): 365-
-
Busse CE, O’Hanlon K, Kozhimannil KB, Interrante JD (2025) Financial challenges of providing obstetric services at rural US hospitals. J Rural Health 41(4): e70082.
-
O’Hanlon CE, Kranz AM, DeYoreo M, Mahmud A, Damberg CL, et al. (2019) Access, Quality, And Financial Performance of Rural Hospitals Following Health System Affiliation. Health Aff (Millwood) 38(12): 2095-2104.
-
Kozhimannil KB, Henning-Smith C, Hung P (2016) The Practice of Midwifery in Rural US Hospitals. J Midwifery Womens Health 61(4): 411-418.
-
VanGompel EW, Singh L, Carlock F, Rittenhouse C, Ryckman KK, et al. (2024) Family Medicine Presence on Labor and Delivery: Effect on Safety Culture and Cesarean Delivery. Ann Fam Med 22(5): 375-382.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda