Problematic of Intensive Care Units in Venezuela
Critical care corresponds to the contemporary stage and includes automated multi-parameter monitoring for the management of patients with multi-organ impairment, complementary tests, devices for basic and advanced bedside support, and a multidisciplinary clinical team. Insufficient financing and inefficiencies in the allocation and use of available resources for health care represent important challenges in moving towards equity and financial protection. In fact, the average public spending on health (GPS) in the Region of the Americas is around 4% of the gross domestic product (GDP), a very low level compared to the 8% that the countries of the Americas allocate on average. The sixth edition of the Venezuela National Hospital Survey (ENH), collects information from 40 hospitals in the 24 states of the country. In the National Survey of Hospitals 2018, it can be seen in the Operative / Non-existent services line that 20% of the units are inoperative in Intensive Care Units for adults, 70% have intermittent failures and only 9% are 100% functional. . In relation to Pediatric Intensive Care, it is observed that 4% are inoperative and 95% have intermittent failures and the Emergency areas 5% are inoperative and 95% have intermittent failures. During 2019, both adult and pediatric Intensive Care Units maintained a pattern of operation between 10 and 20% of closed units, between 65 and 70% of open units and between 10 and 15% with intermittent operation.
Introduction
Critical medicine has specialized in the care and management of patients in critical condition or at risk of developing it, care that cannot be provided in regular hospital wards. Intensive therapy, in turn, emerged in the 1940s, when specific devices and procedures were applied to patients with a single dysfunction, such as mechanical Investigation Paper ventilation, hemodialysis, and electrical defibrillators. Critical care corresponds to the contemporary stage and includes automated multi-parameter monitoring for the management of patients with multi-organ impairment, complementary tests, devices for basic and advanced bedside support, and a multidisciplinary clinical team. Critical medicine as a discipline refers to the science of monitoring and managing critical patients [1].
Intensive care helps people with life-threatening injuries and illnesses. It can treat problems such as complications from surgeries, accidents, infections and severe respiratory problems, involving close and constant medical attention, provided by a team of specially trained health professionals. This care is usually provided in an intensive care or intensive care unit. Monitors, IV lines, feeding tubes, catheters, ventilators and other equipment are common in intensive care units, these devices can keep a person alive, but also increase the risk of infections associated with health care (IACS) [2].
Critical medicine has had a vertiginous development, in which excellent personalized attention to patients, profound knowledge of the pathophysiology of critically ill patients, dazzling advances in technology, molecular biology, monitoring, management and treatment, ethics, and finally, everything that makes critical patient care exciting. Latin America has not been immune to this development. The first Intensive Care units were founded in the late 1960s and early 1970s. Today we can ensure that all Latin American countries have them, managed by intensivists, equipped with sufficient technology to provide adequate management to patients. Patients who require it [3].
Problematic
Progress in the management of patients at acute risk of a life-threatening condition has accelerated with technological advances in monitoring, increasing medical knowledge, as well as with invasive and non-invasive interventions that could be performed: intubation, mechanical ventilation, mechanical ventilation Noninvasive hemodialysis, volume replacement guided by measurement of intravascular pressures, cardiac output, improvements in cardiopulmonary resuscitation, defibrillation, and transient intravenous pacing became common use. These particular techniques have progressed in recent decades, facilitating the work of anesthesiologists in the operating room, post-anesthetic recovery units, and cardiologists in the catheterization room. Conventional observation methods based on physical examination and manual measurement of vital signs at the patient’s bedside were replaced by electronic quantitative and qualitative monitoring techniques that translate the clinical condition of patients [2, 3, 4].
(PIC) is a relatively new discipline within Pediatrics. The first Pediatric Intensive Care Unit (PICU) was established in Gothenburg (Sweden) in 1955, and the first in the United States was created at the Children’s Hospital of the District of Columbia in 1965. In Latin America, PICUs began between 1972 and 1990. Although they have shown great progress, similar in many centers to those of developed countries, the general characteristics of its organization or development are not known. World publications on the subject are scarce and there are no reliable records on the availability of beds in PICUs, access to them and the quality of care provided. Intensive Care Units contribute to improving hospital mortality by up to 10% and, according to international regulations, they should occupy 8 to 10% of installed hospital capacity [5].
Problematic of Intensive Care Units in Venezuela
Access to urgent medical care for life-threatening conditions is a key health expectation for all communities. Medical care in general, and CIP in particular, should help meet these needs with early and timely intervention. From this premise derives the logical interaction that must exist between intensivists and health professionals who care for patients with vital risk. The action of the intensive care physician should not be restricted to the confines of the ICU [4, 5].
Intensive care helps people with life-threatening injuries and illnesses. It can treat problems such as complications from surgery, accidents, infections, and severe respiratory problems. It involves close and constant medical care, provided by a team of specially trained health professionals. This care is usually provided in an intensive care or intensive care unit. Today, critical care is provided by physicians in different specialties: anesthesiology, internal medicine, surgery, pediatrics, and critical care specialists. The health model in this specialty from the beginning has been characterized by teamwork in which cooperation, information and analysis of monitoring data involve doctors from all specialties, nurses, physiotherapists and pharmacologists, among others [5, 6].
Despite the economic growth and advances in health achieved in the last decade, poverty and inequities at the national level and among different countries continue to be a challenge for the Region of the Americas. 29% of the population still lives below the poverty line and 40% receives less than 15% of total income, with very marked differences between countries. The richest 10% of the population has 14 times the average income of the poorest 40% in Latin American and Caribbean (LAC) countries. Likewise, it is estimated that 30% of the population does not have access to health care due to economic reasons and that 21% give up seeking care due to geographic barriers [7].
In parallel, problems of exclusion and lack of access to quality services persist for large sectors of the population. The prevailing models of care, based more on episodic care for acute conditions in hospitals than on prevention and health promotion, often with excessive use of technology and poor distribution of medical specialists, do not necessarily respond to the different health needs of individuals and communities. Investments to reform and improve health systems have not always been geared to meeting new challenges, largely related to the demographic and epidemiological transition, as well as to population expectations [8].
The result is a lack of universality and equity in access to quality services and appropriate coverage, which has a considerable social cost and impoverishing effects on the population groups that are most vulnerable. It is proven that when there are barriers to access to services (whether economic, geographic, cultural, demographic, or others), the deterioration of health not only implies higher expenses, but also the loss of income. The non-existence of protection mechanisms against the financial risk of illness originates and perpetuates a vicious circle of illness and poverty [8, 9].
Insufficient financing and inefficiencies in the allocation and use of available resources for health care represent important challenges in moving towards equity and financial protection. In fact, the average public spending on health (PSH) in the Region of the Americas is around 4% of the gross domestic product (GDP), a very low level compared to the 8% that the countries of the Americas allocate on average. Direct payment (or out-of-pocket expense) at the time of service provision, the most inefficient and regressive source of financing, represents an unstable flow of financial resources and constitutes a barrier to access that prevents or delays care and makes it more expensive for people and the system; It also has a relatively greater impact on people with fewer resources, for whom the smallest payment can represent a significant fraction of their budget. In the Region of the Americas, only six countries have direct spending levels below 20% of total health spending (THS), which is the figure that distances them, according to the World Health Organization (WHO), of the risk that its inhabitants have to face impoverishing or catastrophic expenses [8, 9].
Taking into account the reference of at least 6% of THS as GPS present in the universal health strategy. Only 5 countries of the total of 34 that present information are above that threshold: Canada, Costa Rica, Cuba, the United States and Uruguay. Among those that are below the threshold there are 3 countries that exceed 5% of THS as GPS: Colombia (5.4%), Nicaragua (5.1%) and Panama (5.9%). The Venezuelan health system in the last 20 years has been progressively deteriorating, motivated by several reasons, among them we can mention the low budgetary investment in health, reaching 1.86% of spending on Health expressed as a % of Total Public Expenditure, representing 0.77% of the Gross Domestic Product (GDP), which is equivalent to a Per Capita Public Expenditure of 72 US$ (data as of 2016), the centralization of purchases by the Popular Ministry of Health (MPPS), unscheduled purchases and without consulting the health team that makes life in hospitals, but above all, the abandonment of the traditional health system for the implementation of a parallel system (Barrio Adentro), to which an important part of the budget was derived and without However, it was not efficient either, having reinvested, without obtaining the results initially offered, causing a generalized deficit in the attention of the population that requires health services. Years, evidencing a Complex Humanitarian Emergency in health, manifested by a deficit in medical-surgical supplies, lack of hospital beds, collapse of diagnostic systems, inoperative Bioanalysis laboratories, insufficient Operating Rooms and a limited supply of Intensive Care beds [9, 10].
The coronavirus pandemic arrives in Venezuela with a health system in crisis, with a shortage of supplies, personnel, and, of course, beds. According to the Global Health Security Index 2019, Venezuela is one of the three countries in the region with the fewest hospital beds: only 80 per 100,000 people. That is, for every 1,000 inhabitants there are 0.8 hospital beds in the country. Well below the figure of 2.7 recommended by the World Bank [9, 11].
The crisis with the beds in Intensive Care is general. The former Minister of Health, José Félix Oletta, in the balance on “The last 20 years of health policies in Venezuela”, asserted that at the national level there is a deficit of 37.6% of beds for intensive care. Although there are no official figures from the Ministry of Health to date, the last one published in 2012 revealed that 2,195 beds were required for Intensive Care and 1,360 were available, which is equivalent to 62%.
As far as Caracas is concerned, the bed deficit is similar. There are 16 hospitals dependent on the public network, of these, 14 are in the Libertador municipality and among all, the number of usable beds is 4,861, the budgeted ones are 4,047 and the functional ones are 2,717, that is, 56% of the total. The actual number of emergency beds available in the Ministry of Health hospitals located in Libertador is 271; this is equivalent to 10% of the total beds enabled. In relation to the beds available in the Emergency area, the real number of beds available in the hospitals of the Ministry of Health located in the Liberator municipality (metropolitan area) is 271; this is equivalent to 10% of the total beds enabled [11].
In the year 2000, the World Health Organization (WHO) set the “Millennium Goals” with the purpose of improving the living conditions of humanity until the year 2015. Within these, it stands out, for being of interest to paediatricians, goal 4: «reduce mortality in children under 5 years of age by two thirds by the year 2015». Reaching this goal would mean avoiding more than 6 million deaths each year. The strategy designed to achieve the “Millennium Goals” is based mainly on preventive health measures, but it seems unlikely that these goals will be achieved in many countries due to various problems. New action alternatives are also required, such as those that depend on emergency services and pediatric intensive care (CIP), which must be promptly available to all children who require them, having shown that their planned and careful installation can easily reduce mortality by at least 50%. Once 2015 arrived, and the millennium goals were not achieved, the Sustainable Development Goals program was implemented, to be achieved in 2030, by all developed and developing countries. [9, 11].
Mortality in Pediatric Intensive Care Units
The average mortality in the PICUs of the countries studied is 12%, but it fluctuates from 4% in Spain to 25% in Honduras. The average mortality in Latin American PICUs was 13.29 and 5% in European PICUs, with a statistically significant difference between both regions (p=0.005). Mortality is inversely correlated with PICU availability, number of pediatric intensivists, number of beds, and number of specialty pediatric centers. The more difficult the access to a PICU, the higher the mortality. The cases of Honduras, the Dominican Republic and Ecuador illustrate this correlation. This is not necessarily true in all countries; for example, Mexico has the largest number of specialty pediatric centers, but mortality is comparable to that of Ecuador [2].
Access to urgent medical care for life-threatening conditions is a key health expectation for all communities. Medical care in general, and Pediatric Intensive Care (PIC) in particular, should help meet these needs with early and timely intervention. From this premise derives the logical interaction that must exist between intensivists and health professionals who care for patients with vital risk. The action of the pediatric intensivist should not be restricted to the confines of the PICU [3]. The efficiency of health spending plays a fundamental role in the region’s health performance: if Latin America were a more efficient region in terms of health spending, Latin Americans could live almost four years longer. And in countries like Bolivia, Guyana, Trinidad and Tobago, and Suriname, that number could go up to seven and reach almost 80 years. Latin American and Caribbean countries are generally inefficient in how they spend their money on health. Today, the region is not only behind the developed economies (grouped in the OECD) in health spending per capita —1,109 dollars versus 4,701—, but 22 of 27 countries in Latin America and the Caribbean are below the average in terms of its effectiveness in health spending. And 12 of them, almost half of the total, in the bottom 25% of the entire study [12, 13].
Critical attention has grown significantly in Latin America. This growth is caused by the increase in the number of patients who require this specialized care for whom excellent results are achieved with the indisputable development of critical care. There is a growing interest in the application of systems that guarantee quality medical care, which is why some countries have decided to include critical care in their legislation. Due to economic conditions in the region, there is a marked difference in the number of intensive care beds between Latin American countries compared to European countries and the United States.
Standards are being prepared to establish the minimum human and physical resource requirements to ensure that existing beds are equipped in the best possible way [8, 11].
Mortality figures are significantly different between Latin American and European countries. In Latin America, mortality is inversely correlated with PICU availability, number of pediatric intensivists, number of beds, and number of specialty pediatric centers. The needs for the specialty, expressed by the participants, can help explain this phenomenon, including inequity and heterogeneous distribution of resources, as well as difficult access to them [2].
The Venezuela National Hospital Survey (ENH), technical-scientific reports carried out by the Doctors for Health organization and the Tropical and Infectious Diseases Research Group (GIDETI) with the endorsement of the Societies of Child Care and Pediatrics, Society of Internal Medicine, Venezuelan Society of Cardiology and the National Academy of Medicine-Venezuela. The Doctors for Health Organization has been a spokesperson for the serious humanitarian crisis that Venezuela is experiencing. In the face of censorship and official silence, an alternative was sought to highlight the crisis that Venezuelan doctors knew existed but that no one was talking about. This is how the Venezuela National Hospital Survey (ENH) was born [14].
The survey works on a digital platform, so that it is easily accessible to doctors from all over the country, and with it the conditions of hospital centers at the national level are monitored. Today, as there are no official figures on health issues in Venezuela, ENH has become the only real and reliable information on this crisis. The Organization of American States (OAS), the United Nations (UN), Human Rights Watch, the Pan American Health Office (PAHO), and the World Health Organization (WHO) have been some of the international organizations that have used data from the Survey to argue the serious crisis that Venezuela is going through today [14, 15].
The sixth edition of the National Hospital Survey (ENH), collects information from 40 hospitals in the 24 states of the country. For this edition, only type III and IV hospitals were taken into account (according to the classification of the Ministry of Popular Power for Health), each one of them being the most important hospital/s in its entity. The registered health centers cover all the ascription bodies of the health area, being these: Ministry of Popular Power for Health (MPPS), Venezuelan Institute of Social Security (IVSS), Military Health and Governorates. The survey also records General Hospitals, Military Hospitals, Maternity Hospitals and Children’s Hospitals [11, 14].
In the Venezuela National Survey of Hospitals 2018, it can be seen in the Operative / Non-existent services line that 20% of the units are inoperative in Intensive Care Units for adults, 70% have intermittent failures and only 9% are 100% functional. . In relation to Pediatric Intensive Care, it is observed that 4% are inoperative and 95% have intermittent failures and the Emergency areas 5% are inoperative and 95% have intermittent failures (Graph 1) [14].
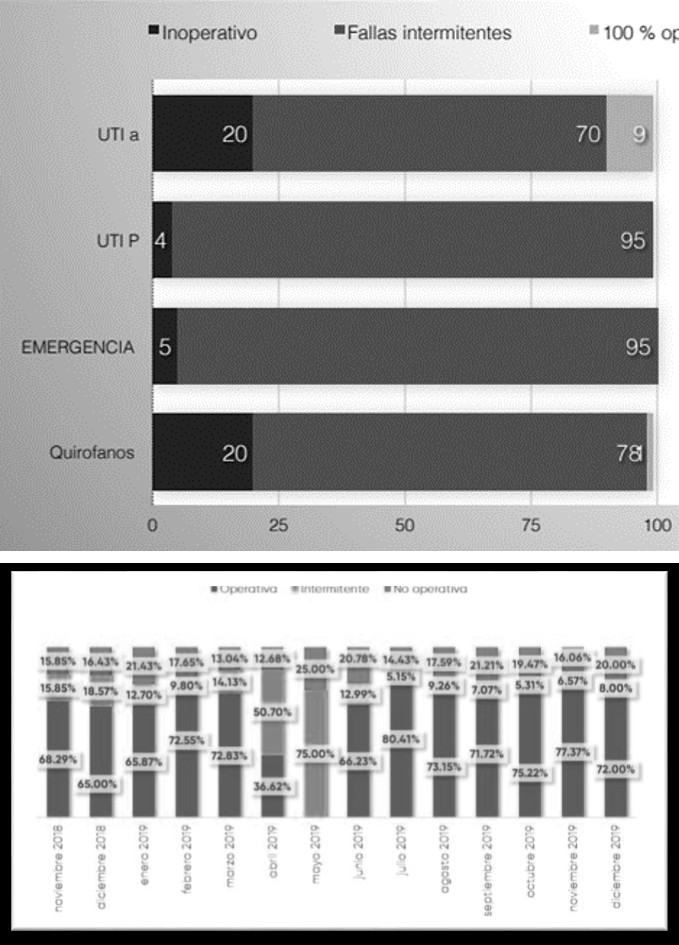
Source: ENH 2018 [14]. Graph 1: ENH 2018. Inoperative/Nonexistent Services.
Service is considered operational when it provides service 24 hours a day, 7 days a week; due to the nature of the survey, the intermittent or with faults and the inoperative ones are grouped together and therefore in some cases there is 100% in that indicator. However, the number of inoperative services at the national level is increasing. There seems to be no willingness to improve conditions. The ministry’s networks only indicate that they are investing in small hospitals or in inner neighborhoods, which do not have the capacity to replace the central hospitals and meet their demand. Added to the crisis in the provision of supplies and medicines (responsibility of the MPPS) was the collapse of public services: electricity, water, garbage and the food crisis [14].
For 2019, the ENH had detailed information from hospitals week by week for a year, it was also marked by events that affected the operation of health centers; electrical blackouts and the entry of humanitarian aid affected the development of the crisis. During 2019, both adult and pediatric Intensive Care Units maintained a pattern of operation between 10 and 20% of closed units, between 65 and 70% of open units and between 10 and 15% with intermittent operation. During the months of March, April and May, the intermittency of the operation of Intensive therapies increased, reaching 75%, a period in which the largest electricity failures were recorded at the national level. Although the power outages lasted 4 to 5 days, the high rate of intermittence in the Intensive Care Units lasted for weeks and even months (Figures 2&3) [15].
Source: ENH 2019 [15]. Figure 2: Operation ICU Adults.
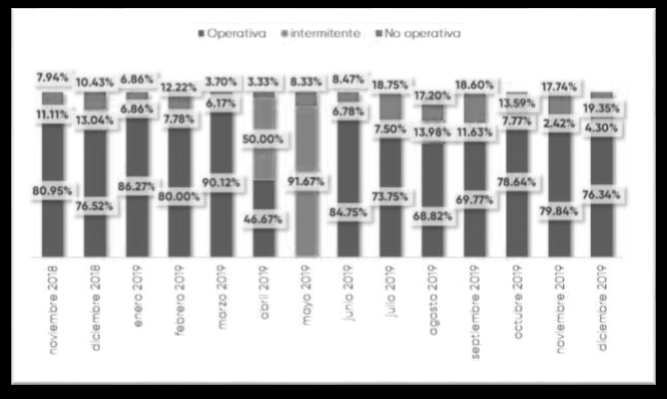
Source: ENH 2019 [3]. Figure 3: Pediatric ICU operability.
In relation to Emergency beds, the national average of Emergency beds had an upward trend of 46.7% in relation to 2018: 35.2% (Figure 4) [15].
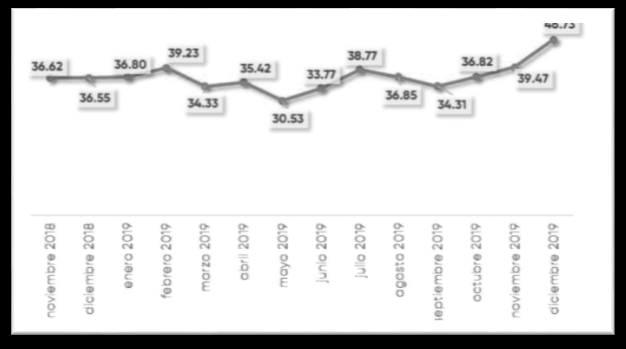
Source: ENH 2019 [15]. Figure 4: Emergency operating beds.
In the availability of human resources and the operability of units such as Emergency, Intensive Care Unit (ICU) and general ward, there seems to be a pattern to keep the most critical areas operational at the expense of the mobilization of personnel and supplies, which in parallel generates that the less critical areas such as hospitalization see a significant deterioration, at least in its real operational capacity. The impact of the national blackouts was very noticeable and manifested itself in less available staff, fewer operating beds, and hospital units mostly operating intermittently [14, 15].
In relation to supply, understanding that it is not easy, since there are countless categories, presentations and formulas that make this measurement complex. Since the beginning of the monitoring, a basic score has been used that measures the availability of medicines or essential supplies in emergencies and operating rooms. The shortage index score is based on the measurement of supplies and medicines considered basic, in Emergencies the existence or not of: antihypertensives, insulin, morphine, aminoglycosides/ quinolones, clindamycin, steroids, heparin, cephalosporins/ beta-lactams, Diazepam, DiphenylHydantoin, inhaled asthma medications, NSAIDs, defibrillator, Lidocaine, Atropine, Intubation, fluid therapy, Dopamine, catheters, Adrenaline, Oxygen, suction, Vancomycin/Clindamycin. On this base list, the availability of each item is rated week by week and is translated into a percentage of general supply. The overall stockout average in 2019 was 49% for emergency rooms. With an initial measurement of 49.67% in November 2018 (Figure 5) [15].
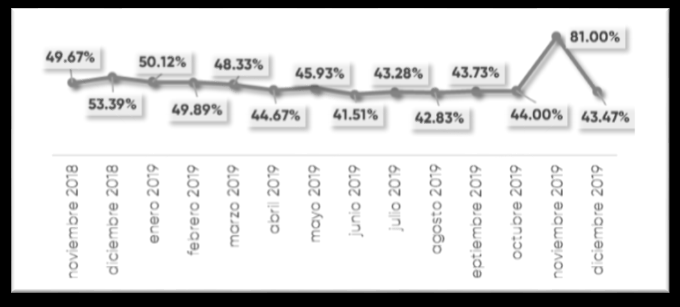
Source: ENH 2019 [15]. Figure 5: Average Shortage in Emergency.
Citizens and political leaders must support professionals with the best scientific knowledge to make decisions about the management of critically ill patients, within a sustainable economic model. Scientific societies have a crucial role in defining minimum levels of intensive medical care and also in ensuring training standards, training of intensivists and accreditation, promoting interaction between specialties, universities and the Venezuelan state. The perception of Intensive Medicine among citizens and the administration must be constantly improved, through efforts aimed at increasing knowledge, taking into account the achievements made by it [16].
An efficient allocation of public spending is a necessary condition to reduce inequities. The implementation of the care model centered on people and communities requires that efficiency be increased by allocating new resources, as a priority, to the first level of care and in the networks to expand the supply of quality services and address unmet health needs quickly. Simultaneously, it is necessary to put into operation a series of available mechanisms to transform the care model and the organization of services. One of them, particularly important, are payment systems that encourage integrated care and continuity of care [17].
By undertaking reforms, changes, or transformations with principles of equity and solidarity, based on health as a right, the member states of PAHO have committed to following the path of eliminating direct or out-of-pocket spending, obtaining pooled funds as broad as possible and the increase in efficient public financing as a way to promote greater access for people and communities to comprehensive quality services in integrated health systems, with a strengthening of the first level of care. In this effort, the types of health systems that are developed in the Region are configured [8, 15, 17].
Conclusion
The region is aging. Latin America and the Caribbean is experiencing a demographic transition where women have fewer children and a more veteran population that needs more (and better) medical coverage. This makes the diagnosis obvious: countries must invest in health and distribute resources more intelligently. Many believe that better health care has to do with how much money the country spends. It has always been thought that more hospitals, more medical personnel and more money would mean better health. And while that’s an important factor, it’s not all about quantity.
Venezuela must urgently increase the budget allocation in health and invest it with equity and social justice, in order to provide an adequate health system.
References
-
Ochoa Parra M (2017) Historia y evolución de la medicina crítica: de los cuidados intensivos a la terapia intensiva y cuidados críticos. Acta Colombiana de Cuidado Intensivo. Acta Colomb Cuid Intensivo 17(4): 258-268.
-
Miño CS, Sasbón J, Dessauer BV. Los cuidados intensivos pediátricos enLatinoamérica. Med Intensiva 36(1).
-
Baker T (2009) Pediatric emergency and Critical care in low-income countries. Paediatr Anaesth 19(1): 23-27.
-
Epstein D, Brill JE (2005) A History of Pediatric Critical Care Medicine. Pediatr Res 58(5): 987-996.
-
Rodriguez EC, Rubiano S (2006) Critical Care in Latin America: Current Situation. Crit Care Clin 22(3): 439- 446.
-
Rodríguez B, Franco J (2015) Historia de la medicina crítica. AnMed Mex 60(2): 156-159.
-
Inciarte GM, Wilhem M (2015) History of the Specialization in Critical Medicine of the Autonomous Service Hospital Universitario de Maracaibo. Historia de la Medicina Crítica en Venezuela 66(1-2).
-
Romero Uzcategui Y (2012) La Formaiòn Medica en Venezuela:¡profesionales para la atención de salud o la enfermedad. Educere 16(54): 59-68.
-
Organización Mundial de la salud/ Organización Panamericana de la Salud. Financiamiento de la Salud en las Américas.
-
Gasto Público en Salud. Datos macro.com
-
Encuesta Nacional de Hospitales 2022.
-
Blanch L, Palomar G (2013) Innovation in intensive care medicine: yes, we must. Med Intensiva 37(1): 3-5.
-
Banco Interamericano de Desarrollo. Mejor gasto, mejor salud.
-
Johns Hopkins (2019) Global Health Security Index. Bloomberg School of Public Health; Center for Health Security.
-
Encuesta Nacional de Hospitales (2019) Balance Final 2019, parte I.
-
Blanch L, Annane D, Antonelli M, Chiche J, Cuñat J, et al. (2013) The future of Intensive care medicine. Med Intensiva 37(2): 91-98.
-
Vincent JL, Singer M, Marini JJ, Moreno R, Levy M, et al. (2010) Thirty years of critical care medicine. Crit Care 14(3): 311.
- Capacity Constraints in Pediatric Inpatient Psychiatric Care: A Cross-Sectional Analysis of Bed Availability and Geographic Access in North Carolina
- Why Healthcare Analytics Still Optimizes the Wrong Things
- Coding, Coverage, and Care: The Infrastructure of Transgender Health Inequities
- The Effect of Classroom Attendance on Academic Achievement of Management and Leadership Discipline of Nursing Students at Instituto Superior Cristal and Universidade de Dili, Timor-Leste, 2024: A Case Study
- The Role of Social Bonds in Facilitating Shared Investments and Resource Allocation: Addressing the “Wrong Pocket Problem” in Public Health and Healthcare
- Social-Cultural Factors Contributing to Antimicrobial Resistance in Livestock Farmers and Community Households in Kayonza District, Rwanda