Depression and Suicide among Undergraduate Students of a Public University in Ghana
Introduction: Incidents of suicide cases and its related episodes increases in tertiary institutions and attract extreme mass media attention with a high proportion of suicide among college students. Globally, over 800 000 people die of suicide every year and it is the second leading cause of death in 15−29-year-olds. This study assessed depression and suicidal tendencies among KNUST undergraduate students. Methods: This study employed a cross sectional study, Likert scaled questionnaires on self-esteem, depression, and suicidal behaviour. And also closed ended questionnaires on availability of suicide preventive services on campus. Results: The study found out that majority of the students had high level of self-esteem (84.20%). Also, the prevalence of depression among students in this study was 25.15% for major depression episode and 66.34% for people who at mild depression. Again, it was revealed in this study that a prevalence of 26.37% suicidal tendency and its related behaviour exist among KNUST undergraduate students. Depression and Suicidal tendency demonstrated a weak and insignificant correlation of r= 0.18, p
Background Information
Suicide and depression are said to be important mental health challenges among college students. Family and society who are responsible for making psychological healthcare available, accessible and affordable are not giving the needed attention to this serious public health problem. Lereya ST, et al. [1], suicide and suicidal attempts are most important public health concern that needs attention. Recent information from the National Centre of Health Statistics point out that suicide is the third principal cause of death among people between the of ages of 10-24 and the 5th leading root of death among people ages 25-44. The overall suicidal rate for a study conducted on the big 10 students from 1980 to 1990 was 7.5 suicide per 100,000. This was the rate found highest among college students [2].
Suicidal behaviour rates in some countries increase progressively with age, although there is a peak in suicide rates among young adults. Young adults and elderly women in low- and middle-income countries, have more suicidal behaviour rates as compare to their corresponding person in high-income countries, though middle-aged men in high- income countries have more suicidal rates than individuals in low- and middle-income countries. Internationally, suicides account for 50% of all forceful deaths in men, and 71% of such deaths in women [3].
According to an updated fact of the World Health Organization, one of the key facts of depression is: “at worst depression leads to suicide”. Several reports show this problem to be serious. The third prominent root of death for adolescents, young adults or youth is suicide in the United States. Mental health conditions which are closely related with adolescent suicidal behaviour is the occurrence of mood Disorder. Consistently depression has been identified as a threat element for suicidal behaviour in adolescents and young adults. Risk factors associated with youth suicide include substance abuse, adverse life events before death, contact with legal authorities and arrests, family history of mental illness and suicide, history of sexual abuse and a history of past suicide attempt are definite risk factors for suicide attempts. Depression is a common mental disorder that presents one with depressed mood, loss of interest or pleasure, decreased energy, feelings of guilt or low self- worth, disturbed sleep or appetite, and poor concentration. Depression affects more than 300 million people of all ages; it’s the leading cause of disability worldwide, and a major contributor to the overall global burden of diseases; more women are affected by depression than men; at its worst depression can lead to suicidal behaviour.
Some suicide cases in University of Ghana were reported on myjoyonline.com in March, 2017 a final year student committed suicide by jumping from 4th floor and was found dead by porters with severe head injuries. And also in June, 2017 a Level 200 student of University of Ghana, Legon was reported to have committed suicide, he was alleged to have hanged himself. This preventable suicidality includes suicidal thoughts, ideations, attempts and its related behaviour and has been perceived to be so common among college-age students.
In 2017, suicide made headlines in Ghana, it can be recollected that there were a series of suicide cases in the country’s tertiary institutions that drew headlines in mainstream media. Cases of suicide were recorded in Ghana’s tertiary institutions.
WHO [4] also states that globally, for every person who completes a suicide 20 or more may attempt to end their lives. In Ghana, media reports on suicide are alarming. The Daily Graphic (September 15, 2015 edition) reported that Ghana records 1,500 suicide cases annually and this is caused by depression. This was revealed by Akwasi Osei, the Chief Executive Officer (CEO) of the Mental Health Authority (MHA). He added that “in every single reported case of suicide there were four unreported cases and this brings the number of unreported cases to about 6,000 annually”.
In Ghana, the absence of a national policy on suicide prevention is one of the greatest challenges, coupled with lack of political will and commitment to empower the MHA and negligence of counselling and guidance centres in schools and communities. In a news story on myjoyonline. com in February, 2017, a first-year student of the Kwame Nkrumah University of Science and Technology (KNUST) committed suicide, the young18 year-old lady, took her life in her hostel room with a rope. Also another incident as reported on ghanaweb.com in September, 2017, a death of a 20-year-old male student occurred after ingestion of a bottle of poisonous No-pest insecticide. His friends said, he made six different suicidal attempts. Unfortunately, his seventh attempt has been successful. In my view, suicide among teenagers and young adults pursuing college/university program is becoming common. This can be prevented through early recognition and prediction of signs and symptoms of depression.
Methods and Materials
Study Population
The target population were undergraduate students in the six (6) colleges of KNUST-Kumasi, namely: College of Science (CoS), College of Engineering (CoE), College of health sciences (CoHS), College of Agriculture and Natural Resource (CANR), College of Art Built & Environment (CABE), and College of Humanity and Social Sciences (CoHSS).
Study Variables
The main variables in this study were self-esteem, depression, suicidal tendencies, suicide risk factors, and suicide preventive services.
Sampling
Studying the whole population to arrive at a generalization is expensive and impractical. Therefore, a sample size was determined from the population in question using an appropriate sampling technique for observation and analysis. The below Cochran’s method was used to estimate the sample size of undergraduate population of KNUST. Thus n= Z2p(1-p)/d2
n = required sample size Z = Confidence level of 95% = 1.96 p = Assumed proportion from similar studies is 40% expressed in decimal = 0.4 (Thomas, 2015) q=1-p= probability of the event not occurring, in this case 1-0.4 d = Margin of error of 5% expressed in decimal = 0.05 = = 368.7 n ≅ 369 Adding a 10% non-response rate; = 37 n = 369 + 37 = 406 Using 2.5 as design effect (as a correction factor to adjust the required sample size). n = 406 x 2.5 = 1015, approximately 1000 Therefore, a sample size of one thousand (1000) undergraduate students were selected from the six colleges of KNUST as participants. Convenient sampling method was used to select 1000 participants from all the six colleges using probability proportionate to size (PPS), this was based on the population proportions in the various colleges and a total students’ population of 33,216 as at July, 2017 (Quality Assurance Unit KNUST), these were expressed as follows: CANR 4733 (14%) were 140 participants, CABE 3266 (10%) were 100 participants, CoE 4993 (15%) were 150, CoHS 5840 (18%) represented 180 participants, CoHSS 8576 (26%) were 260 participants, and CoS 5808 (17%) also representing 170 participants. Since only college of engineering students’ list and school of medical sciences was obtained from the university, probability sampling (simple random) could not be employed. Hence, convenient sampling strategy was used to select the estimated participants for the study.
Participation in this study was voluntary; one thousand (1000) questionnaires were administered after extensive information has been given to the participants for self- administration. There were eight hundred and twenty-three (823) who responded to the questionnaires and retrieved from study subjects and even with this some skipped some of the items on the questionnaire. This may be due to the total number of the questions as some of participants called to complain that the questions were too many and that it was taking a lot of their time. It may also be due to fact that some were not willing to shear their private information.
Pre-Testing
One hundred (100) subjects were conveniently selected from a similar population, University College of Management Studies (UCOMS) with the same characteristics for pre-testing of data collection tools (questionnaires). After administration of questionnaires to the respondents, the tool was assessed, analysed and the necessary adjustment and corrections were made in the questionnaire.
Data Collection Techniques and Tools
This study made use of primary data. The primary data provided structured close ended questionnaires to adequately cover the purpose of this research. The questionnaires were given to respondents (students) directly and were self- administered. Majority of the questionnaires were adopted from existing tested scaled questionnaires that have been used in other studies, they were; Centre of Epidemiology Scale of Depression (CES-DC), Rosenberg’s Self-Esteem Scale (SES) and Suicide Behaviour Questionnaire-Revised (SBQ-R). There were also questionnaires that were used to collect data on demography, risk factors of suicide and suicide supportive services. The questionnaires were simply worded, language terminologies were ensured, such that respondents were not alienated or marginalized with regards to sexual orientation, gender, age, disability or race.
Brief Description of Scale Instruments
Centre for Epidemiologic Studies Depression Scale (CES- DC): The scale was made up of twenty statements which were all examining these negative felling of the individual, except four of them connoting a positive feeling to act as a check on some of the sensitive issues. Each item was scored using the following items: zero point for rarely or none of the time (less than 1 day), 1 point for some or a little of the time (1-2 days), 2 points for occasionally or a moderate amount of time (3-4 days), and 3 points for most or all of the time (5-7 days). The scoring of positive items is reversed. Possible range of scores is zero to 60, with the higher scores indicating the presence of more symptomatology. Scores on the CES-DC range from 0 to 60, in which higher scores suggest a greater presence of depressive symptoms. A score of 30 or more is interpreted to indicate a risk for depression. However, screening for depression is a complex process and scoring a 16 or higher on the CES-DC should be followed by further evaluation.
Suicide Behaviour Questionnaire-Revised (SBQ-R): This tool contained four questions assessing individual’s suicidal behaviour. The individuals are asked questions relating to their attempts to kill themselves, frequency of these thoughts, sharing of these thoughts with someone and the likelihood of them committing the act. The SBQ-R has 4 items each seeking a different dimension of suicidality.
- Item 1 taps into lifetime suicide ideation and or suicide attempts. Response 1 is 1point, response 2 is 2points, response 3 & 4 are 3points and response 5 & 6 are 4points.
- Item 2 evaluates the incidence of suicide of suicidal thoughts over the past twelve months. Here, response 1 is 1point, response 2 is 2points, response 3 is 3points, response 4 is 4points and response 5 is 5points.
- Item 3 also assesses the threats of suicide attempts. Response 1 is 1point, response 2 & 3 are 2points and response 4 & 5 are 3points.
- Item 4 evaluates self-reported likelihood of suicidal behaviour in the future. In this item response 1 is 0 point, response 2 is 1point, response 3 is 2points, response 4 is 3points, response 5 is 4 points, response 6 is 5points, and response 7 is 6points.
A maximum score of 18 and minimum of 3 is possible on the SBQ-R. A total score of 7 and higher in the general population and a total score of 8 and higher in patients with psychiatric disorders indicate significant risk of suicidal behaviour. Due to the wording of the four SBQ-R items a broad range of information is obtained in a very brief administration. Responses can be used to identify at risk individuals and specific risk behaviours. In general population the sensitivity is 93% and specificity 95%.
Rosenberg Self-Esteem Scale: It consists of 10 statements related to overall feelings of self-worth or self-acceptance. Scoring and interpretations are calculated as follows: For items 1, 2, 4, 6, 7: strongly agree=3, agree=2, disagree=1, strongly disagree=0. For items 3, 5, 8, 9, 10: strongly agree=0, agree=1, disagree=2, strongly disagree=3. The scale score ranges from 0-30, a higher score of 15 denotes higher self- esteem. Administration Time-2 to 3 minutes. Administration Technique - Self-administered questionnaire. Strengths - The SES is widely used. Researchers will be able to search literature for established norms in areas of interest. Scale Format - Likert type scale, ranging from strongly agree - strongly disagree. 10 items. Test-retest Reliability - Correlations range from .82 to .88. Internal Consistency - Cronbach’s alpha range from .77 to .88. Some studies that have used these instruments are: Gray Little B, et al, Baumeister RF, et al, Ciarrochi J, et al, [5, 6, 7] and a Comprehensive discharge planning for the hospitalized elderly (Jun 1994).
Data Handling: All collected data were stored on the personal desktop computer of the principal investigator, where the data was kept under strict surveillance and assess was granted to only investigators for analysis. This information however was deleted from the site when the final report is ready for presentation. Data collected during the study were only kept for the period needed and would be destroyed after three years of this study. The recorded study data was not shared with any third party but used only by the researcher for the purpose for which they were collected.
Data Analysis: Descriptive analyse was employed. Data was analysed quantitatively using STATA version 13.0, a univariate analysis was performed to describe the counts on each research question and the average responses to each question. This helped the study to get the general picture on the frequency of responses to each research question. Logistic regression analysis was used to test the relation among study variables; self-esteem, depression and suicidal tendencies. Graphical presentation such as tables and charts (scatter diagram) were presented in the results chapter to illustrate findings and visualize relationships.
Ethical Consideration: Aside the ethical clearance been requirement the researcher was anticipating possible ethical issue that may arise during and after the studies. A written approval to conduct this study was obtained from Committee of Human Research Publications and Ethics (CHRPE) of the Kwame Nkrumah University of Science and Technology, Kumasi. Also, the dean of students approved the study, head of department (Health Education and Promotion) approved and again had an approval from the various provosts of the six colleges studied in KNUST in this research. In addition, there were consent forms for participants, which explained participant’s rights; to participate voluntarily, to withdraw from the study any time, to provide information about the purpose of the study, to ask question and also right to privacy that should be protected.
Results
Evaluation of Self-Esteem Among Students Using Rosenberg’s Self-Esteem Scale
The study also evaluated the student’s self-esteem by using Rosenberg’s self-esteem scale. The scale employs ten statements which aims to assess the general feeling of an individual about his self-worth. Five of these statements have been structured to connote a negative sentiment about the individual, whiles the other group also connotes a positive sentiment. On the positive statements, half (51.04%) of the study population believe that they are of equal worth like other people, whiles four percent also disagree strongly that other people are better than them.
Similarly, some sixty-three percent of the student strongly feel they possess good quality whiles a little over one percent hold a strong contrary view. Most of the students also agree strongly that they are able to do things as other people are capable of (54.14%). Meanwhile almost three percent also disagree that they are able to do things on their own. The scale further reveals that half of the students take positive statements toward themselves and also strongly agrees to be satisfied with them. On the contrary, one percent and other two percent of the student however strongly disagree with this assertion (Table 1).
| for header rows | for data cells | |
|---|---|---|
| Age group in years | ||
| 18-24 | 793 | 96.35 |
| 25-34 | 23 | 2.79 |
| 35-44 | 7 | 0.85 |
| Sex | ||
| Male | 418 | 50.78 |
| Female | 405 | 49.22 |
| Relation status | ||
| Not in a romantic relationship | 656 | 79.71 |
| In romantic relationship | 167 | 20.29 |
| Parent’s relationship status | ||
| Remain married | 591 | 71.81 |
| Divorced or separated | 75 | 9.11 |
| Remarried (one parent or both parents) | 44 | 5.35 |
| Other | 113 | 13.73 |
| Academic year/level | ||
| First-year | 400 | 48.6 |
| Second year | 339 | 41.19 |
| Third year | 45 | 5.47 |
| Fourth-year | 39 | 4.74 |
| Campus resident type | ||
| Male only | 220 | 26.73 |
| Female only | 47 | 5.71 |
| Mixed | 333 | 40.46 |
| Non-campus residential | 223 | 27.1 |
| Nationality | ||
| Ghanaian | 797 | 96.84 |
| Nigeria | 18 | 2.19 |
| Other Nationals | 8 | 0.97 |
| College | ||
| Agriculture and natural resource | 346 | 42.04 |
| Health Sciences | 158 | 19.2 |
| Humanities and Social Sciences | 134 | 16.28 |
| Arts and Built Environment | 74 | 8.99 |
| Sciences | 28 | 3.4 |
| Engineering | 83 | 10.09 |
| Ever had counselling | ||
| No | 538 | 65.37 |
| Yes | 285 | 34.63 |
| Personal mental health history | ||
| No | 816 | 99.15 |
| Yes | 7 | 0.85 |
| Family mental health history | ||
| No | 791 | 96.11 |
| Yes | 32 | 3.89 |
Table 1: Demographic Characteristics of Undergraduate Students of KNUST Demographic Characteristics of Undergraduate Students of
Source: field data, 2018 Table 1: Demographic Characteristics of Undergraduate Students of KNUST Demographic Characteristics of Undergraduate Students of a Public University.
Further to the individual evaluating themselves, most of them strongly disagree that they are failures (60.32%), however there were eleven percent of the students who strongly feel they have failed. More than a third of the students strongly feel they have something to be proud of (39.66%), whereas twenty-one percent agrees to the fact that they do not have much to pride themselves with. Forty percent of the students agrees that they have more respect for themselves whiles twelve percent strongly disagree in their current state to lack respect. Similarly, most (39.66%) of the students strongly disagree to the fact of feeling useless at times. Sixteen percent of the students believe strongly that they are not good at all, whiles over thirty-six percent of the students disagree strongly to that as shown in Table 2.
| Positive Score | 1 | 2 | 3 | 4 | |
|---|---|---|---|---|---|
| Positive Score | No. | Strongly Agree (%) | Agree (%) | Disagree (%) | Strongly Disagree (%) |
| 1 | I feel that I am a person of worth, at least on an equal plane with others. | 416 (51.04) | 306 (37.55) | 57 (6.99) | 36 (4.42) |
| 2 | I feel that I have a number of good qualities. | 519 (63.06) | 279 (33.90) | 14 (1.70) | 11 (1.34) |
| 4 | I am able to do things as well as most other people. | 445(54.14) | 296(36.01) | 58(7.06) | 23(2.80) |
| 6 | I take a positive attitude toward myself. | 426(51.76) | 332(40.34) | 53(6.44) | 12(1.46) |
| 7 | On the whole, I am satisfied with myself. | 390(47.39) | 280(34.02) | 135(16.40) | 18(2.19) |
| 4 | 3 | 2 | 1 | ||
| Reverse Score | Strongly Agree (%) | Agree (%) | Disagree (%) | Strongly Disagree (%) | |
| 3 | All in all, I am inclined to feel that I am a failure | 92(11.23) | 41(5.01) | 192(3.44) | 494(60.32) |
| 5 | I feel I do not have much to be proud of. | 61(7.44) | 177(21.59) | 259(31.59) | 323(39.39) |
| 8 | I wish I could have more respect for myself. | 225(27.54) | 350(42.84) | 138(16.89) | 104(12.73) |
| 9 | I certainly feel useless at times. | 74(9.00) | 180(21.90) | 242(29.44) | 326(39.66) |
| 10 | At times I think I am not good at all. | 134(16.28) | 204(24.79) | 184(22.36) | 301(36.57) |
Table 2: Evaluation of self-esteem among students using Rosenberg’s Self-esteem Scale.
Evaluation of Depression Level among Students Using the Centre for Epidemiologic Studies Depression Scale (CESD)
The Table 3 below show the frequency and percentage distribution of student’s response to a list of statements which describes how an individual feel or behave at times. These statements are self-reported measure of depression for individual known as centre for epidemiologic studies depression scale. These are twenty set of statements which have been grouped nine subscales with each measuring a particular aspect of depression. In evaluating the possibility of Sadness (Dysphoria), most (41.36%) of the students rarely show signs of poor appetite or eating habit, however others occasionally do not feel like eating at all (17.76%) whiles a little below four percent (3.89%) in most or all of the time do not have appetite at all. Similarly, forty-three percent of the student rarely feel a sense of depressed, but on the contrary some students on occasionally (13.03%) and most of the time feel depressed (12.18%). Fourteen percent of the student on rare occasion feels they are as good as other people, whiles most (42.32%) of them feels they as good as others all the time as shown in Table 4.3.
Most of the students at all times feels hopeful about their future (58.14%), whiles nine percent feels hopeful some or a little of the time. Also, almost eight percent all the time feels fearful in life (7.93%) in an attempt to evaluate feeling of loss of interest (Anhedonia). Seven percent among the study population most of the time feel sad whiles a similar eight percent also get bothered about thing that usually does not others them between five to seven days at a point in time.
About half of students experiences restless sleep (48.30%), however fourteen percent on occasionally had trouble in sleeping. Over a quarter of them also believe that people dislike them at some or little of the time (28.22%), whiles nine percent also have difficulty in keeping their mind on what they are doing in most of the times. In measuring the students thinking or concentration, more than half (55.85) of them on rare occasion feel they could not get going contrary to the fourteen percent who on all the time feels they could not get going. However, nine percent at all the time feels that without friends or families “they could not shake off the blues”.
| No | Subscales | 0 | 1 | 2 | 3 |
|---|---|---|---|---|---|
| Rarely or none of the time (less than 1 day) (%) | Some or a little of the time (1-2 days) (%) | Occasionally or a moderate amount of time (3-4 days) (%) | Most or all of the time (5-7 days) (%) | ||
| Sadness (Dysphoria) | |||||
| 2 | I did not feel like eating; my appetite was poor | 340(41.36) | 304(36.98) | 146(17.76) | 32(3.89) |
| 4 | I felt I was just as good as other people. (reverse score) | 117(14.27) | 154(18.78) | 202(24.63) | 347(42.32) |
| 6 | I felt depressed | 355(43.24) | 259(31.55) | 107(13.03) | 100(12.18) |
| Loss of interest (Anhedonia) | |||||
| 8 | I felt hopeful about the future (reverse score) | 158(19.34) | 75(9.18) | 109(13.34) | 475(58.14) |
| 10 | I felt fearful. | 394(48.05) | 234(28.54) | 127(15.49) | 65(7.93) |
| Appetite | |||||
| 1 | I was bothered by things that usually don’t bother me | 293(35.82) | 220(26.89) | 239(29.22) | 66(8.07) |
| 18 | I felt sad | 378(46.10) | 240(29.27) | 141(17.20) | 61(7.44) |
| Sleep | |||||
| 5 | I had trouble keeping my mind on what I was doing | 262(31.95) | 292(35.61) | 190(23.17) | 76(9.27) |
| 11 | My sleep was restless. | 397(48.30) | 217(26.40) | 119(14.48) | 89(10.83) |
| 19 | I felt that people dislike me | 430(52.31) | 232(28.22) | 76(9.25) | 84(10.22) |
| Thinking or Concentration | |||||
| 3 | I felt that I could not shake off the blues even with help from my family or friends | 380(47.50) | 193(24.13) | 150(18.75) | 77(9.63) |
| 20 | I could not get “going.” | 458(55.85) | 193(23.54) | 49(5.98) | 120(14.63) |
| Guilt (worthlessness) | |||||
| 9 | I thought my life had been a failure | 533(64.92) | 124(15.10) | 119(14.49) | 45(5.48) |
| 17 | I had crying spells | 499(61.15) | 191(23.41) | 86(10.54) | 40(4.90) |
| Tired (Fatigue) | |||||
| 7 | I felt that everything I did was an effort | 127(15.54) | 196(23.99) | 237(29.01) | 257(31.46) |
| 16 | I enjoyed life. (reverse score) | 123(15.02) | 203(24.79) | 152(18.56) | 341(41.64) |
| Movement (Agitation) | |||||
| 12 | I was happy (reverse score) | 137(16.71) | 118(14.39) | 180(21.95) | 385(46.95) |
| 13 | I talked less than usual | 250(30.49) | 215(26.22) | 233(28.41) | 122(14.88) |
| Suicidal ideation | |||||
| 14 | I felt lonely | 323(39.73) | 255(27.68) | 132(16.24) | 133(16.36) |
| 15 | People were unfriendly | 300(36.67) | 264(32.27) | 164(20.05) | 90(11.00) |
| REVERSE SCORE | 3 | 2 | 1 | 0 | |
| Rarely or none of the time (less than 1 day) (%) | Some or a little of the time (1-2 days) (%) | Occasionally or a moderate amount of time (3-4 days) (%) | Most or all of the time (5-7 days) (%) |
Table 3: Evaluation of the level of depression among students using the centre for epidemiologic studies depression scale (CESD).
Only few students at most of the time felt their lives had been a failure in an attempt to measure their feeling of self- worth (5.48%). Similarly, about five percent also experience crying spells all of the time (4.90%). Fifteen percent of the students rarely feels they enjoy life and also feels that everything they did was an effort in a way, contrary to the thirty-one and forty-one percent who time feel same at most or all of the time respectively. A further attempt was made to measure the suicidal ideation and what they termed as movement (agitation). About sixteen percent and eleven percent feels lonely and also feels people are unfriendly in most of the time contrary to the thirty-nine and thirty-six percent who on rare occasion feels that respectively. Also, about forty-six percent of the students in most or all the time feels happy, whiles thirty percent also rarely feels they talk less than usual contrary to the fourteen percent who in most of the time talk less than usual.
Assessment of Suicidal Tendencies among Students Using Suicide Behaviour Questionnaire (SBQ-R)
The possibility of an existence of suicide behaviour among the students were examined using the revised suicide behaviour questionnaire. More than half of the students interviewed had never thought or made any attempt to kill him/herself (63.56%), however there were about six percent who had attempted to kill themselves but didn’t want to die, whiles there were other students (0.61%) who attempted to killing themselves and really hoped to die. Also, there were other students (0.86%) who had a plan of killing themselves once and really wanted to die as shown in Table 4.
| Frequency | Percentage | |
|---|---|---|
| 1. Have you ever thought about or attempted to kill yourself? | ||
| 1=Never | 518 | 63.56 |
| 2=It was just a brief passing thought | 213 | 26.13 |
| 3=I have had a plan at least once to kill myself but did not try to do it | 20 | 2.45 |
| 4=I have had a plan at least once to kill myself and really wanted to die | 7 | 0.86 |
| 5=I have attempted to kill myself, but did not want to die | 52 | 6.38 |
| 6=I have attempted to kill myself, and really hoped to die | 5 | 0.61 |
| 2. How often have you thought about killing yourself in the past year? | ||
| 1=Never | 554 | 67.64 |
| 2=Rarely (1 time) | 192 | 23.44 |
| 3=Sometimes (2 times) | 23 | 2.81 |
| 4=Often (3-4 times) | 47 | 5.74 |
| 5=Very Often (5 or more times) | 3 | 0.37 |
| 3. Have you ever told someone that you were going to commit suicide or that you might do it? | ||
| 1=No | 586 | 72.44 |
| 2=Yes, at one time, but did not really want to die | 171 | 21.14 |
| 3=Yes, at one time, and really wanted to do it | 28 | 3.46 |
| 4=Yes, more than once, but did not want to do it | 2 | 0.25 |
| 5=Yes, more than once, and really wanted to do it | 22 | 2.72 |
| 4. How likely is it that you will attempt suicide in the future? | ||
| 0=Never | 560 | 68.21 |
| 1=No chance at all | 172 | 20.95 |
| 2=Rather Unlikely | 55 | 6.7 |
| 3=Unlikely | 26 | 3.17 |
| 4=Likely | 2 | 0.24 |
| 5=Rather Likely | 1 | 0.12 |
| 6=Very Likely | 5 | 0.61 |
Table 4: Assessment of Suicidal Tendencies among Students Using the Revised Suicide Behaviours Questionnaire (SBQ-R).
Source: field data, 2018. Table 4: Assessment of Suicidal Tendencies among Students Using the Revised Suicide Behaviours Questionnaire (SBQ-R).
In an attempt to assess how often students thought of killing themselves in the past year, about sixty-seven percent never had that thought often, however there were other students (0.37%) who thought about that very often; for more than five or more times. The majority (7.44%) of the students had not ever mention to anyone about their plan to kill themselves; however others (2.72%) informed people of their intentions for more than one occasion and really wanted to do it. Most of the students believe is never likely they will attempt suicide in the future, whiles there are less than a percentage (0.61%) who believe they are very likely to attempt it in the future (Table 5).
| Frequency | Percentage | |
|---|---|---|
| Rosenberg Self-Esteem Scale | ||
| Score ≤ 20 | ||
| Low Self-Esteem (Score Less Than 20) | 130 | 15.8 |
| Score ≥ 20 | ||
| High Self-Esteem (Score Greater Than 20) | 693 | 84.2 |
| Mean Score (SD) | 22.19 (2.57) | |
| Center for Epidemiologic Studies Depression Scale (CESD) | ||
| Score ≤ 16 | ||
| No Symptoms of Depression | 70 | 8.51 |
| Score ≥ 16 ≤ 30 | ||
| At Risk for Clinical Depression | 546 | 66.34 |
| Score ≥ 30 | ||
| Major Clinical Depression Episode | 207 | 25.15 |
| Mean Score (SD) | 24.18(7.62) | |
| Suicide Behaviors Questionnaire-Revised | ||
| Score ≤ 6 | ||
| No Significant Risk of Suicidal Behaviour | 606 | 73.63 |
| Score ≥ 7 | ||
| Significant Risk of Suicidal Behaviour | 217 | 26.37 |
| Mean Score (SD) | 4.77(2.71) |
Table 5: Rosenberg Self-esteem Scale, Centre for Epidemiologic Studies Depression scale (CESD) and the Revised Suicide Behaviours
Source: field data, 2018 Table 5: Rosenberg Self-esteem Scale, Centre for Epidemiologic Studies Depression scale (CESD) and the Revised Suicide Behaviours Questionnaire.
Examining the Relationship between Self- Esteem, Depression and Suicidal Tendencies among Students at KNUST
The study also examined the relationship that exists between self-esteem, depression and suicidal behaviour of students. There was a negative correlation between self-esteem and suicidal behaviour (r= -0.22, p<0.001), such that low self- esteem was seen to have an inverse relationship with suicidal behaviour among students and vice versa. High self-esteem score also negatively correlates with high suicide scores as presented graphically in Figure 1.
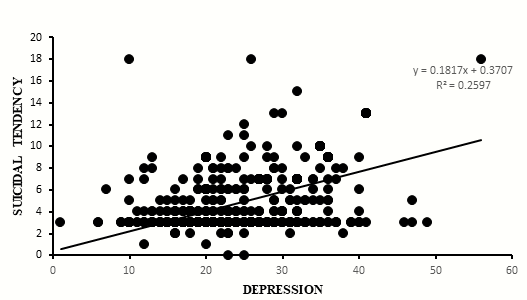
On the contrary depression showed a positive correlation with suicidal behaviour (r= 0.18, p<0.001), among students.
As the score for depression increases, the score for suicidal behaviour also increases. Thus, depression score and suicide score move in tandem.
A regression analysis was conducted to ascertain the effects of self-esteem and depression on the behaviour of the students regarding suicide. Both self-esteem and depression contributed to twenty-eight percent variance in the suicidal behaviour [adj. R2 = 0.28] of the students.
Self-esteem was significantly related to suicidal behaviour. There was an inverse relationship between the two. Every increase in self-esteem score caused suicide behaviour score to decrease by 0.16 [95% CI = -0.22, 0.98; p<0.001]. But depression on the other hand showed a significant positive relationship with suicide behaviour among the students. The results showed that every single increase in depression score caused a 0.18 increase in suicidal behaviour score [95% CI = 0.15, 0.19; p<0.001] as presented in Table 6.
Discussion
Demographic Characteristics of Students
The study achieved a response rate of 81%, against the ninety percent response rate envisaged. However, this response rate was significantly higher, which enables findings of the study to be generalized to other student population with similar characteristics. The age distribution among the students ranged between 18 years to 44 years, with the majority been in their youthful age brackets. Also, the study had an equal gender distribution. The ratio of gender distribution in this study is similar to reports from several studies conducted elsewhere among college or university students in the country, even though is higher than the current national distribution of male to female student population is a ratio of 3:2 among tertiary students [8].
The majority of the students were within the age range of which reflects the both global trend and national trend of tertiary students being basically youth (18-24 years) which reflects the national demographics of our tertiary institutions [8]. The average years a student spends throughout his schooling from the basic to the university is 18 years in Ghana. Taking into consideration the standard six years a child is require to attain before starting school explains why most people enter the university at age 18 and complete at 24 years with all other things being equal [8, 9].
The youthful age group (18-24years) dominated the prevalence of self-esteem level, depression and suicidal tendency evaluation. It has been widely reported that depression and suicidal tendencies has a significant relationship with age and gender [10]. Depression levels and suicidal tendencies are much higher among young adults and but remain consistently same with gender as both male and the female population did not exhibit any disparity in their depression levels and suicidal tendencies [8, 11, 12].
Evaluation of Self-Esteem, Level of Depression and Suicidal Behaviour among Students
In evaluating the student’s level of self-esteem, some questions from Rosenburg’s scale were asked to test their personal feeling about their worthiness. These questions have been extensively used and have proven to be effective in self-rating of an individual’s level of self-esteem by several social researches [13, 14, 15]. Almost all the positive statements about a person’s self-worth were strongly agreed by half of the population studied and the negative statements which act as check on the positive statements also had similar number of students strongly disagreeing to them. This implied that, the students genuinely understood the statements and what they meant, translating to the reason why majority of the students were classified as having high self-esteem.
Depression levels of students were similarly measured with Centre for Epidemiologic Studies Depression Scale. This tool has been established to exhibit high level of internal consistency across samples and worked perfectly in most African settings. Baron EC, et al. [16] concluded that this scale is a valid and reliable screening tool for depression among Africans.
The scale evaluated the individual’s behaviour through a number of subscales, with each scale measuring a particular human behaviour. The behaviours ranged from Dysphoria, Anhedonia, Appetite, sleep, concentration, guilt, fatigue, movement and suicidal ideation. The scale was made up of twenty statements which were all examining these negative felling of the individual, except four of them connoting a positive feeling to act as a check on some of the sensitive issues.
The students were asked to rate how they feel from time to time and how frequently they experience that in a month; ranging from less than a day (rarely); 1-2 days (little of the time); 3-4 days (occasionally) and 5-7 days (all of the time). About forty percent of the students consistently felt as good as other people, hopeful about the future, enjoyed life, happy all of the time, throughout the response. This probably explained why the scale recorded relatively high prevalence of major depression episode (25.15%) and mild or at risk for clinical depression (66.34%) respectively.
In the assessment of suicidal tendencies among the students, a final tool known as the suicide behaviour questionnaire was used. The tool contained four questions assessing individual’s suicidal behaviour. The individuals are asked questions relating to their attempts to kill themselves, frequency of these thoughts, sharing of these thoughts with someone and the likelihood of them committing the act.
The majority of the students never thought of killing themselves ever (63.56%), however less than a percentage had at least plan once to commit the act, whiles almost seven percent nearly succeeded in committing the act but were afraid to die, another five students really had attempted the act and are really hoping to die one day (0.61%).
Some of the students with these thoughts had actually thought about it for about 3-4 times (5.74%) and more than five times (0.37%) respectively. Some of the students who were bent on committing suicide had informed people at one time about their intentions and really wanted to do it (3.46%), whiles others informed people more than once and really wanted to commit the act (2.75%). Consistently five students believe they are very likely going to commit the act in the near future.
Evaluating Self-Esteem Level, Prevalence of Depression and Suicidal Tendency Among Students at KNUST Self- Esteem: Self-esteem is an important factor that influence a person’s general behaviour and mental wellbeing. Psychological conditions like depression and suicidal tendencies are affected in various ways an individual’s feeling on his/her self-worth. Therefore, the study in an attempt to evaluate depression among students had to first assess the level of self-esteem among the students at KNUST. Chen, et al. [17] reported in their study among college students that, self- esteem is a moderating factor that affect depression directly or indirectly. Other similar studies investigating self-esteem and depression have conclude on the relation between the two [18].
Assessing depression among a particular group becomes practically impossible without taking into consideration their level of self-esteem. The study found out that majority of the students had high level of self-esteem (84.20%). This figure is relatively higher compared to other studies which investigate interaction between self-esteem and other behaviour related conditions among university students elsewhere [19, 20], Demo DH, et al. [19] and colleagues in their study of academic performance and self-esteem among British college students reported low self-esteem among college students in general, even though there was no significant variation among the various race involve in the study. The variation of difference in level of self-esteem could be influence by several factors ranging from genetics, environmental, social, psychological and economic status among others as reported by several studies [21, 22, 23]. This aspect was not investigated in our study as it falls outside its focus.
Depression Level: Depression is known to be one of the most common mental health problems globally, which has a grave impact of the quality of life on an individual and affecting their susceptibility to also self-induce injuries, crimes and even murder at the extreme cases. Being a condition that affects nearly one out of every twenty people globally and about percent of the American population, it has become necessary for it to be classified as a public health problem [24, 25, 26]. It is a condition that’s is widely experience among the younger age and university students and has some form of relations with suicidal behaviour [17, 25, 27, 28].
According to the 2016, American Foundation for Suicide Prevention a higher percentage of all the victims who experience depression are not given any attention or do not seek for treatment including those living in the high- income countries such as America. This probably accounts for the sixty percent cause of the suicide cases recorded. Most individual suffering from depression without proper guidance and counselling is on the record to commit suicide. Therefore, any attempt to control the rate of suicidal tendencies and behaviour requires a careful consideration of depression as an important variable. Reducing the rate of depression is one of the surest ways to minimize its effect on suicide.
The prevalence of depression among students in this study was 25.15% for major depression episode and 66.34% for people who at risk of depression or with mild depression. This implies that about a quarter of the student population studied could have a tendency of thinking of any suicide attempt at some point in times. The findings from this study was not consistent with a similar study that was conducted in Nigeria, Brazil and Thailand among general university students [8, 23, 24, 29, 30]. Their study prevalence of depression ranged between 8-15.6% among the university students which is lower than figures from current study. But interestingly, there were other studies conducted in United States and Peru reported a depression higher rate of 31% -36% among the students [11]. However, those studies were directed towards medical students only, this could be the possible explanation for the variation. Also, the methodological differences and the populations involved in the various studies could affect the findings.
Suicidal Tendency: The study revealed a prevalence of 26.37% suicidal tendency and its related behaviour among the students as presented in table 4.5. This rate was estimated from the suicidal behaviour scores obtained from the study. Students who scored above the accepted threshold classified as no risk of suicidal behaviour or tendency (score ≤ 6) were included in the estimation. This rate is alarming as far as student safety are concerned, because the rate of suicidal tendency reported elsewhere is lower than the rate in this current study. For instance [30] in their study of correlated of depressive syndrome, anxiety, suicidal thoughts and behaviour among university and college students reported a rate of 2%. Other study on the contrary also reported higher rate of suicidal ideation at 43.7% among the students and 14.5% as those who actually attempted committing the act [31].
Relatively to either of the cases, the rate recorded in the current study cannot be overlooked since they represent a higher number. More than a quarter of the study population, holding all other circumstance constant, any real attempt or occurrence of suicide could be detrimental to the general wellbeing of a student. Suicidal thoughts are likely to reoccur to people who have had at least one experience of suicide attempts or thoughts and such people are to be expected to have such thoughts again [32]. According to Joiner, et al. [33] thought about suicide and its related behaviour are critical indicators and precursors of both suicide attempt and actual suicide, therefore it is important to take a precautionary action as soon as any symptom like that identified among any population.
Examining the Relationship between Self- Esteem, Depression and Suicidal Tendencies Among Undergraduate Students of KNUST
The study employed a regression analysis to test whether self-esteem, depression and suicidal tendencies are correlates. Several studies across the globe have given varied reports on the trio for having direct interaction and otherwise. This makes their relationship a blur one which needs an investigation [17, 25, 27, 28] For instance, Self- esteem has been reported to be a mediating or moderating factor between depression and suicidal tendency by investigators like Chen, et al. [34, 17]. On the contrary others studies have also reported that self-esteem and depression to be risk factors for suicidal tendencies [18, 35]. With all these conflicting reports the researcher for this study narrowed their focus to investigate their interaction with each other.
The study found out the self-esteem negatively correlated with suicidal tendency and depression on the other hand correlate positively with suicidal tendency. The relationship between the two (self-esteem and suicidal tendency) was an inverse one. In other words, a low individual self-esteem influence significantly the rate of suicidal tendency and vice versa. For instance, the diathesis model assumes that barring all other circumstances, individuals with low self-esteem usually do not have much coping strategies to life stressors and easily gets into a depressive state, which obviously could lead to suicidal state if not properly managed. An individual with low self-esteem has a negative picture about his self- worth and also about how people perceive him. This self- assessment can sometimes be disturbing thereby activating some form of depression, which when not managed properly can end up in a suicidal tendency [36]. This finding does not vary from a conclusion reported by [37] in their study of depressive symptoms, their role in violence among African- American students.
Depression on the other hand positively relate to suicidal tendencies in the sense that high depressive mode is considered as critical and has been documented in other studies to have a direct relationship with the individual behaviour and actions [37]. Findings from this study correlates with the above report. Depression and Suicidal tendency demonstrated a significant correlation of r= 0.18, p<0.001) [38, 39, 40, 41, 42, 43, 44, 45].
The regression model revealed that self-esteem had negative effect of 0.16 times on the rate of suicide when the rate for self-esteem drops by a unit and also the rate of suicide reduces by same margin when a self-esteem score increases [46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58]. This implies that high self-esteem becomes protective against individual suicidal tendency, therefore activities aimed at empowering and promoting self-esteem is required if we need to control suicidal tendency among university students [59, 60, 61, 62, 63, 64, 65, 66, 67]. The model also revealed that depression score also contributes to an increase in suicidality by 0.18 times with an increase in depression rate [68, 69, 70, 71, 72, 73, 74, 75, 76], all these relationships were statistically significant [0.18; 95% CI = 0.15, 0.19; p<0.001]. This confirms reports by [18, 77, 78, 79, 80, 81, 82] in septate studies that both self-esteem and depression as predictive factors to suicide behaviour among individuals [83, 84, 85, 86].
Recommendations
The following recommendations in respect to this study goes to the Dean of Student, Head of Counselling unit of KNUST, Head of mental health Services of the university’s hospital as well as individuals, associations, and clubs within KNUST:
- Focus on depression and suicide screening exercises at least once in a year for the students. This will help to identify students who are highly depressed and also those are likely to commit suicide and refer them to appropriate counselling or treatment centre.
- Organise regular education and awareness creation to increase students’ knowledge on availability of depression and suicide supportive services such as suicide hotlines/helplines and other suicide supportive services on campus. The university’s SMS platform can be helpful by sending students messages on suicide preventive services on campus and suicidality tips such as signs and symptoms of suicidal behaviour and suicide reporting format and channels.
- Develop depression and suicide prevention policy for KNUST.
- Aimed activities that empower and reduces depression should be encouraged among KNUST undergraduate students and in campus activities. Such as spending time with people (socialisation), encouraging students to do things that make use of one’s own special talents and abilities and learn something new or improve your skills.
References
-
Lereya ST, Winsper C, Heron J, Lewis G, Gunnell D, et al. (2013) Being bullied during childhood and the prospective pathways to self-harm in late adolescence. Journal of the American Academy of Child and Adolescent Psychiatry 52(6): 608-18.e2.
-
Garlow SJ, Rosenberg J, Moore JD, Haas AP, Koestner B, et al. (2008) Depression, desperation, and suicidal ideation in college students: results from the American Foundation for Suicide Prevention College Screening Project at Emory University. Depression and anxiety 25(6): 482-488.
-
World Health Organisation (2014) Preventing suicide: a resource for non-fatal suicidal behaviour case registration.
-
World Health Organization (2012) Public health action for the prevention of suicide: a framework.
-
Gray Little B, Williams VSL, Hancock TD (1997) An item response theory analysis of the Rosenberg Self-Esteem Scale. Personality and Social Psychology Bulletin 23: 443-451.
-
Baumeister RF, Campbell JD, Krueger JI, Vohs KD (2003) Does high self-esteem cause better performance, interpersonal success, happiness, or healthier lifestyles? Psychological Science in the Public Interest 4(1): 1-44.
-
Ciarrochi J, Heaven PCL, Fiona D (2007) The impact of hope, self-esteem, and attributional style on adolescents’ school grades and emotional well-being: A longitudinal study. Journal of Research in Personality 41(6): 1161- 1178.
-
National Accreditation Board N (2013) Tertiary Education Statistics Report: Ghana. National Accreditation Board.
-
Ghana Statistical Services (2010) Ghana Labour Statistics: Economic activity status of persons 15 years and older by region. Labour Statistics.
-
Nock MK, Borges G, Bromet EJ, Cha CB, Kessler RC, et al. (2008). Suicide and suicidal behavior. Epidemiologic Reviews 30: 133-154.
-
Hojat M, Glaser K, XU G, Veloski JJ, Christian EB (1999) Gender comparisons of medical students’ psychosocial profiles. Medical Education 33: 342-349.
-
Brent DA (1995) Risk factors for adolescent suicide and suicidal behavior: mental and substance abuse disorders, family environmental factors, and life stress. Suicide and Life‐Threatening Behavior 25: 52-63.
-
Gosling SD, Rentfrow PJ, Swann WB (2003) A very brief measure of the Big-Five personality domains. Journal of Research in Personality 37: 504-528.
-
Robins RW, Hendin HM, Trzesniewski KH (2001) Measuring global self-esteem: Construct validation of a single-item measure and the Rosenberg Self-Esteem Scale. Personality and Social Psychology Bulletin 27(2): 151-161.
-
Rowley SJ, Sellers RM, Chavous TM, Smith MA (1998) The relationship between racial identity and self-esteem in African American college and high school students. Journal of Personality and Social Psychology 74: 715- 724.
-
Baron EC, Davies T, Lund C (2017) Validation of the 10- item centre for epidemiological studies depression scale (CES-D-10) in Zulu, Xhosa and Afrikaans populations in South Africa. BMC Psychiatry 17(1): 6.
-
Chen C, Hong YH, Yang S (2010) Relationships among adolescents’ life events, self-esteem, depression and suicide ideation. Chin J Clin Psychol 18: 191.
-
Orth U, Robins RW, Trzesniewski KH, Maes J, Schmitt M (2009) Low self-esteem is a risk factor for depressive symptoms from young adulthood to old age. Journal of Abnormal Psychology 118(3): 472-478.
-
Demo DH, Parker KD (1987) Academic achievement and self-esteem among Black and White college students. The Journal of Social Psychology 127: 345-355.
-
Friedlander LJ, Reid GJ, Shupak N, Cribbie R (2007) Social support, self-esteem, and stress as predictors of adjustment to university among first-year undergraduates. Journal of College Student Development 48: 259-274.
-
Ko CH, Yen JY, Chen CC, Chen SH, Yen CF (2005) Gender differences and related factors affecting online gaming addiction among Taiwanese adolescents. The Journal of Nervous and Mental Disease 193(4): 273-277.
-
Morrow KB, Sorell GT (1989) Factors affecting self- esteem, depression, and negative behaviors in sexually abused female adolescents. Journal of Marriage and the Family 51(3): 677-686.
-
Adewuya AO, Ola BA, Aloba OO, Mapayi BM, Oginni OO (2006) Depression amongst Nigerian university students. Social Psychiatry and Psychiatric Epidemiology 41(8): 674-678.
-
Phimarn W, Kaewphila P, Suttajit S, Saramunee K (2015) ‘Depression screening and advisory service provided by community pharmacist for depressive students in university’, Springer Plus 4: 1-12.
-
White L, Klinner C, Carter S (2012) Consumer perspectives of the Australian Home Medicines Review Program: benefits and barriers. Research in Social and Administrative Pharmacy 8(1): 4-16.
-
World Federation for Mental Health. World Mental Health Day (October 10, 2012) ‘Depression: A Global Crisis.
-
Lam T, Stewart SM, Yip PS, Leung GM, Ho L, et al. (2004) Suicidality and cultural values among Hong Kong adolescents. Social Science & Medicine 58(3): 487-498.
-
Chiles JA, Strosahl KD, Zheng YP, Michael MC, Hall K, et al. (1989) Depression, hopelessness, and suicidal behavior in Chinese and American psychiatric patients. The American Journal of Psychiatry 146(3): 339-344.
-
Cavestro JDM, Rocha FL (2006) Depression prevalence among university students. Brazilian Journal of Psychiatry 55: 264-267.
-
Eisenberg D, Gollust SE, Golberstein E, Hefner JL (2007) Prevalence and correlates of depression, anxiety, and suicidality among university students. American Journal of Orthopsychiatry 77(4): 534-542.
-
Rudd MD (1989) The prevalence of suicidal ideation among college students. Suicide and Life‐Threatening Behavior 19(2): 173-183.
-
Drum DJ, Brownson C, Denmark AB, Smith SE (2009) New data on the nature of suicidal crises in college students: shifting the paradigm. Professional Psychology: Research and Practice 40(3): 213-222.
-
Joiner TE, Steer RA, Brown G, Beck AT, Pettit JW, et al. (2003) Worst-point suicidal plans: A dimension of suicidality predictive of past suicide attempts and eventual death by suicide. Behaviour Research and Therapy 41(12): 1469-1480.
-
Abela JR (2002) Depressive mood reactions to failure in the achievement domain: A test of the integration of the hopelessness and self-esteem theories of depression. Cognitive Therapy and Research 26: 531-552.
-
Franck E, De Raedt R (2007) Self-esteem reconsidered: Unstable self-esteem outperforms level of self-esteem as vulnerability marker for depression. Behaviour research and therapy 45: 1531-1541.
-
Bhar S, Ghahramanlou Holloway M, Brown G, Beck AT (2008) Self-esteem and suicide ideation in psychiatric outpatients. Suicide and Life-Threatening Behavior 38(5): 511-516.
-
Fitzpatrick KM, Wright DR., Piko BF, Lagory M (2005) Depressive symptomatology, exposure to violence, and the role of social capital among African American adolescents. American Journal of Orthopsychiatry 75(2): 262-274.
-
Arria AM, O’grady KE, Caldeira KM, Vincent KB, Wilcox HC, et al. (2009) Suicide ideation among college students: A multivariate analysis. Archives of Suicide Research 13(3): 230-246.
-
Au ACY, Lau S, Lee MTY (2009) Suicide ideation and depression: The moderation effects of family cohesion and social self-concept. Adolescence 44(176): 851-868.
-
Axelson DA, Birmaher B (2001) Relation between anxiety and depressive disorders in childhood and adolescence. Depression and anxiety 14(2): 67-78.
-
Borowsky IW, Resnick MD, Ireland M, Blum RW (1999) Suicide attempts among American Indian and Alaska Native youth: Risk and protective factors. Archives of Pediatrics & Adolescent Medicine 153(6): 573-580.
-
Brent DA, MANN JJ (2005) Family genetic studies, suicide, and suicidal behavior. American Journal of Medical Genetics 133(1): 13-24.
-
Carleton RN, Thibodeau MA, Teale MJ, Welch PG, Abrams MP, et al. (2013) The Center for Epidemiologic Studies Depression Scale: A review with a theoretical and empirical examination of item content and factor structure. PLOS ONE 8(2): e58067.
-
Colluci E, Martin G (2007) Ethnocultural aspects of suicide in young people: A systematic literature review. Part 2: Risk factors, precipitating agents, and attitudes toward suicide. Suicide and Life-Threatening Behavior 37(2): 222-237.
-
Cerel J, Padgett JH, Conwell Y, Reed GA, (2009) A call for research: The need to better understand the impact of support groups for suicide survivors. Suicide and Life- Threatening Behavior 39(3): 269-281.
-
Durkheim E (1895) Suicide as Social Fact. Pp: 1-6.
-
Furr SR, Westefeld JS, McConnell GN, Jenkins JM (2001) Suicide and depression among college students: A decade later. Professional Psychology: Research and Practice 32(1): 97-100.
-
Ginges J, Hansen I, Norenzayan A (2009) Religion and support for suicide attacks. Psychological science 20(2): 224-230.
-
Gladstone TR, Koenig LJ (1994) Sex differences in depression across the high school to college transition. Journal of Youth and Adolescence 23: 643-669.
-
Gould MS, Fisher P, Parides M, Flory M, Shaffer D (1996) Psychosocial risk factors of child and adolescent completed suicide. Archives of General Psychiatry 53(12): 1155-1162.
-
Gross EB (1972) Gender differences in physician stress. Journal of the American Medical Women’s Association 47(4): 107-112.
-
Harris TL, Molock SD (2000) Cultural orientation, family cohesion, and family support in suicide ideation and depression among African American college students. Suicide and Life-Threatening Behaviour 30(4): 341-343.
-
Harter S, Marold DB, Whitesell NR (2008) Model of psychosocial risk factors leading to suicidal ideation in young adolescents. Development and Psychopathology 4(1): 167-188.
-
Hojat M, Robeson MR, Veloski JJ, Blacklow RS, Xu G, et al. (1994) Gender comparisons prior to, during, and after medical school using two decades of longitudinal data at Jefferson Medical College. Evaluation & the Health Professions 17(3): 290-330.
-
Huang KL, Wei HT, Hsu JW, Bai YM, Su TP, et al. (2018) Risk of suicide attempts in adolescents and young adults with attention-deficit hyperactivity disorder: a nationwide longitudinal study. The British Journal of Psychiatry 212(4): 1-5.
-
Johnson J, Wood AM, Gooding P, Taylor PJ, Tarrier N (2011) Resilience to suicidality: The buffering hypothesis. Clinical Psychology Review 31(4): 563-591.
-
Kisch J, Leino EV, Silverman MM (2005) Aspects of suicidal behavior, depression, and treatment in college students: Results from the Spring 2000 National College Health Assessment Survey. Suicide and Life Threatening Behavior 35(1): 3-13.
-
Konick LC, Gutierrez PM (2005) Testing a model of suicide ideation in college students. Suicide and Life- Threatening Behavior 35(2): 181-192.
-
Lewinsohn PM, Rohde P, Seeley JR (1994) Psychosocial risk factors for future adolescent suicide attempts. Journal of consulting and clinical psychology 62(2): 297- 305.
-
Matlin SL, Molock SD, Tebes JK (2011) Suicidality and depression among African American adolescents: The role of family and peer support and community connectedness. American journal of orthopsychiatry 81(1): 108-117.
-
Matlin SL (2008) The relationship between exposure to violence and depression: An ecological model of protective factors among African American adolescents Doctoral dissertation, The George Washington University.
-
Merchant C, Kramer A, Joe S, Venkataraman S, King CA (2009) Predictors of multiple suicide attempts among suicidal Black adolescents. Suicide and Life-Threatening Behavior 39(2): 115-124.
-
Naylor M, Brooten D, Jones R, Lavizzo Mourey R, Mezey M, et al. (1994) Comprehensive discharge planning for the hospitalized elderly. A randomized clinical trial. Ann Intern Med 120(12):999-1006.
-
O’donnell L, O’donnell C, Wardlaw DM, Stueve A (2004) Risk and resiliency factors influencing suicidality among urban African American and Latino youth. American Journal of Community Psychology 33(1): 37-49.
-
O’keefe VM, Tucker RP, Wingate LR, Rasmussen KA, (2012) American Indian hope: a potential protective factor against suicidal ideation. Journal of Indigenous Research 1(2).
-
Osman A, Bagge CL, Gutierrez PM, Konick LC, Kopper BA, et al. (2001) The Suicidal Behaviors Questionnaire- Revised (SBQ-R): Validation with clinical and nonclinical samples. Assessment 8(4): 443-454.
-
Paladino D, Minton CA (2008) Comprehensive college student suicide assessment: application of the BASIC ID. Journal of American College Health 56(6): 643-650.
-
Radloff LS (1977) The CES-D Scale: A self-report depression scale for research in the general population. Applied Pscyhological Measurement 1(3): 385-401.
-
Rogers J, Sheldon A, Barwick C, Letofsky K, Lancee W (1982) Help for families of suicide: survivors support program. The Canadian Journal of Psychiatry 27(6): 444-449.
-
Rosenberg, M (1965) Society and the adolescent self- image. Princeton University Press, Princeton, NJ, USA, pp: 338.
-
Ross M (1966) The Practical Recognition of Depressive and Suicidal States. Ann Intern Med 64: 1079-1086.
-
Schwartz AJ (2006) Four eras of study of college student suicide in the United States: 1920-2004. Journal of American College Health 54: 353-366.
-
Sinclair SJ, Blais MA, Gansler DA, Sandberg E, Bistis K, et al. (2010) Psychometric properties of the Rosenberg Self-Esteem Scale: Overall and across demographic groups living within the United States. Evaluation and the Health Professions 33(1): 56-80.
-
Stansbury JP, Ried LD, Velozo CA (2006) Unidimensionality and bandwidth in the Center for Epidemiologic Studies Depression (CES-D) Scale. Journal of Personality Assessment 86(1): 10-22.
-
Tebes JK, Kaufman JS, Adnopoz J, Racusion GR, (2001) Resilience and family psychosocial processes among children of parents with serious mental disorders. Journal of Child and Family Studies 10: 115–136.
-
Thomas AL (2015) Suicidal Thoughts and Behaviour among Black College Students: Examining the Impact of Distress Tolerance and Social Support on Suicidality. Masters Theses & Specialist Projects pp: 1531.
-
Ustun TB, Ayuso Mateos JL, Chatterji S, Mathers C, Murray CJL (2004) Global burden of depressive disorders in the year 2000. The British Journal of Psychiatry 184: 386- 392.
-
Walker RL, Wingate LR, Obasi EM, Joiner TE (2008) An empirical investigation of acculturative stress and ethnic identity as moderators for depression and suicidal ideation in college students. Cultural Diversity and Ethnic Minority Psychology 14(1): 75-82.
-
Wang C (2013) Depression and Suicide Behaviour among College Students: Understanding the Moderator Effects of Self-Esteem and Suicide Resilience. Electronic Thesis and Dissertations pp: 686.
-
Westefeld JS, Furr SR (1987) Suicide and depression among college students. Professional Psychology: Research and Practice 18(2): 119.
-
Westefeld JS, Homaifar B, Spotts J, Furr S, Range L, et al. (2005) Perceptions concerning college student suicide: Data from four universities. Suicide and Life-Threatening Behavior 35: 640-645.
-
Winters NC, Myers K, Proud L (2002) Ten-year review of rating scales. III: Scales assessing suicidality, cognitive style, and self-esteem. American Academy of Child and Adolescent Psychiatry 41(10): 1150-1181.
-
http://citifmonline.com
-
https://myjoyonline.com
-
https://mobile.ghanaweb.com/GhanaHomePage/ NewsArchive/KNUST-student-commits-suicide-586549
-
https://myjoyonline.com/
- Systematic Review and Meta-analysis Investigating the Prevalence of Depression, Anxiety, Loneliness and Help seeking among International Students
- Family Experiences and their Interpretations as a Source of Adaptive Behaviour in Young Adults: A Qualitative Model of Adaptive Behaviour
- The Development of Responsibility in Teenage Mothers: A Qualitative Model
- Post-Truth Reality: Worldwide Infodemia and Mental Health Concerns during and Post COVID-19 Pandemic Scenarios
- Psycho-Emotional Rehabilitating Means of Overcoming Extreme and Stressful Impact
- The Paradox of Humbleness, Arrogance and the Concept of Fluid Individuality