Metacognitive Rehabilitation in the Elderly: the Mind the Gap Metacognitive Program
This paper introduces the Mind the Gap Metacognitive Program (MGM-P), an innovative rehabilitation approach to contrast and prevent anosognosia. Anosognosia, or impaired self-awareness of illness and related deficits, is a pretty frequent phenomenon in Alzheimer's Disease, even in pre-clinical stages, which may have detrimental effects on clinical course, therapy compliance, risky behaviors, not to say caregivers’ stress and burden. Stemming from a complex bio-psycho-social perspective and firmly rooted in accredited neuropsychological models on self-awareness and metacognition, the MGM-P aims at improving patients’ realistic self-appraisal, facilitating the adoption of self-safety behaviors and compensatory strategies, thus lessening patients’ and caregivers’ stress. Theoretical models, structure of sessions, and methodology are illustrated. The MGM-P can be administered to the Elderly with dementia but also with Mild Cognitive Impairment and Subjective Cognitive Complaint. Thus, the MGM-P has been developed as a therapeutic approach and as a preventive tool to buffer cognitive decline and facilitate identifying elderly at-risk subjects. Another original aspect of MGM-P is the presence of quantitative indices, which allow the clinician to objectively rate the patient’s progress in different metacognitive functions and make the MGM-P quite adaptable for research purposes. Last but not least, MGM-P shows a wide range of fruitful next ameliorants and applications in other neuropsychiatric conditions and different contexts, such as in educational and job formation fields.
Introduction
An increasing number of older adults has represented the last decade’s constant demographic trend worldwide. Although a positive sign of the times, the drawback of longer life expectancy is an increasing incidence of age-related Conceptual Paper health diseases, in particular, dementia due to Alzheimer’s Disease (AD). AD is thought to begin 20 years or more before overt symptoms, and it starts with changes in the brain that are unnoticeable to the person affected; only after years of brain changes may individuals experience symptoms such as progressive cognitive, functional, and neuropsychiatric impairment, severe enough to restrict an individual’s autonomy in daily life [1]. Long this continuum between hidden and overt symptoms, there are three broad phases: pre- clinical AD, Mild Cognitive Impairment (MCI), and dementia due to AD. Age, genetics, biological sex, and environmental factors affect the length of each continuum phase [2]. During pre-clinical AD, individuals have measurable brain changes that indicate the earliest signs of AD (biomarkers such as abnormal levels of beta-amyloid, decreased metabolism of glucose, and abnormal form of protein tau); despite the presence of these alterations, they have no obvious cognitive symptoms such as memory loss [3, 4]. MCI represents the prodromal phase, and it is characterized by the emergence of cognitive symptoms, which are noticeable by the subject and family members and they do not interfere with the individual’s ability to do activities of daily living [5, 6].
One of the earliest brain functions vulnerable to cognitive decline is self-awareness. In fact, the core neuropathological features of AD include widespread neurodegeneration encompassing cortical regions and brain-wise networks that are implicated in supporting aspects of self-awareness [7]. In this context, self-awareness is the reasonable or realistic appraisal of a given aspect of one’s situation, functioning, performance, or resulting implications [8]. In AD, alterations in self-awareness, or anosognosia, consist in the undervaluation, or even full unawareness, of impairments in activities of daily living, memory deficits, and behavioral changes [9, 10, 11]. Anosognosia has a detrimental effect on illness course, therapy compliance, and patient’s behavioral symptoms, not to say on patients’ and caregivers’ burden and care costs [12, 13, 14]. Moreover, anosognosia dramatically hampers the probability of risky behaviors, such as wandering, forgetfulness while preparing meals, inadequate medicine assumption, difficulties in money handling, and risky car driving [15, 16, 17, 18, 19, 20].
Notably, impairments in self-awareness have also been highlighted in MCI, where they may represent a predictor for conversion to AD and worse clinical outcome [7, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30]. Even in Subjective Cognitive Decline (SCD) [31], alterations of realistic self-appraisal may precede and accelerate cognitive decline [32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42].
Far from being a trivial issue, a realistic understanding of new cognitive limitations can crucially contribute to a well-timed identification of subjects at risk of dementia to encourage patients to adopt self-safety behaviors and to better comply with medical treatment. Eventually, caregivers’ burden and patients’ quality of life would benefit. This is why self-appraisal rehabilitative programs for the Elderly, mostly if affected by cognitive decline, are strongly warranted.
Altered Mechanisms Underpinning Self- Awareness Deficits in the Elderly
Anosognosia is a failure in metacognition, i.e., the ability to self-reflect, self-monitor, and self-correct one’s performance [42, 43, 44]. Metacognition includes several sub- functions (e.g., semantic and episodic mnestic components, implicit awareness, online self-monitoring, self-correction, emotional relevance, etc). The abundance of clinical and neurological evidence has contributed to cast light on the multifaceted nature of metacognition and self-awareness, thus stimulating the development of multilevel models [45, 46]. Overall, evidence suggests a continuum of self- awareness phenomena across the stages of AD, ranging from realistic insight to hypernosognosia and anosognosia [35, 47].
Several studies have pointed out a relevant involvement in anosognosia of global cognitive impairment and memory deficits [29, 48, 49, 50, 51, 52] functional and/or structural alterations in the right anterior insula, prefrontal and temporal brain areas [42, 53, 54, 55, 56, 57, 58, 59, 60] and some neuropsychiatric symptoms, mainly psychotic symptoms, and apathy [25, 61, 62, 63, 64, 65, 66]. Last but not least, the role of environmental, motivational, and emotional factors [67, 68, 69, 70] cannot be overlooked when challenging such a multi-determined phenomenon [71, 72, 73].
Rehabilitative Interventions for Anosognosia
Most of the rehabilitative approaches to contrast anosognosia are based on education, experiential feedback, behavioral therapy approach, individual or group counseling, psychotherapy, strength and weakness lists, and rating task performances, while others are mainly centered on cognitive stimulation [74, 75, 76, 77]. Some studies selected specific classes of tasks and manipulated specific characteristics of information [78, 79, 80, 81], although sometimes disregarding ecological validity for the sake of a molecular understanding of the phenomena. Despite their relevance, these efforts have not yet merged into a systematic and standardized rehabilitation program specifically developed to boost metacognitive functions in older adults.
The Mind the Gap Metacognitive Program (MGM-P)
Reference background: In this paper, we introduce the model of the Mind the Gap Metacognitive Program (MGM-P), which is based on the most accredited contributions in neuropsychology and neuroscience. The core hypothesis of MGM-P is that self-awareness is the ultimate product of metacognitive activity, which, in turn, deals with autonoetic knowledge. Autonoetic knowledge can be defined as the pool of information, beliefs, and judgments related to the self and one’s abilities [82]. Throughout the lifespan, information drawn from personal experience and external feedback is stored in the episodic and semantic dimensions of autobiographical memory, thus merging with autonoetic knowledge [83].
Metacognitive function, to regulate actions and to make provisions about the self, not only gleans information from autonoetic knowledge but also deals with updating it based on incoming information. In the elderly, especially those with cognitive decline, metacognitive dysfunction prevents a correct update process so that autonoetic knowledge, and finally, self-awareness, relies on a sort of fixed-in-time concept [84].
In this perspective, we mainly referred to the Pyramidal Model of Awareness [81, 85]. Although initially developed concerning anosognosia following traumatic brain injury, it can be generalized to other neuropsychiatric conditions. It considers three interdependent levels of self-awareness: i) at the bottom of the pyramid there is Intellectual Awareness (IntAw), i.e., the cognitive capacity of the subject to conceive at least notionally that a particular function has diminished from premorbid activities; ii) at an intermediate level there is Emergent Awareness (EmAw), or the ability to recognize a deficit as it occurs, while the subject is making his/her performance or immediately after having completed the action; iii) at the top of the pyramid there is Anticipatory Awareness (AntAw), i.e. the ability to make realistic previsions about one’s performances also weighing impairments, thus adopting appropriate compensatory strategies. We postulate a circular and integrated relationship between these levels of awareness and hypothesize that deficits in self-appraisal may depend on failures occurring at each level (Figure 1).
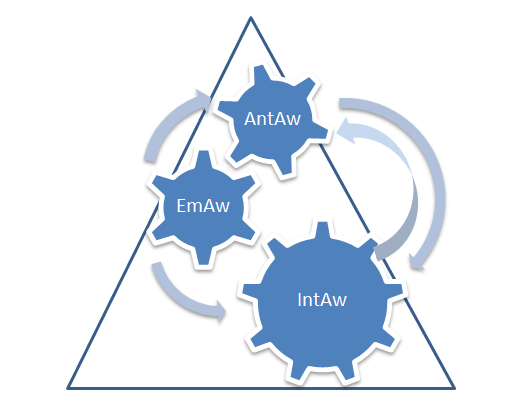
Source: IntAw= Intellectual Awareness; EmAW= Emergent Awareness; AntAw= Anticipatory Awareness. Figure 1: Pyramidal Model of Awareness.
Another essential in the field is the Cognitive Awareness Model (CAM) [86], which suggests specific neural mechanisms to verify consistency between incoming data and self-representations stored in a personal database (PDB). In case of a mismatch, the PDB should be updated based on this comparison, and the product of this process is conveyed via the Metacognitive Awareness System to provide conscious decision-making. Further, Central Cognitive Comparator Mechanisms, underpinned by executive control, would be designated to detect current functional deficits compared to stored information. Thus, impairments in mental functions may prevent the consolidation of new information and, thus, the correct updating of self-image.
In addition to these models, we considered the previously cited evidence about neuropsychological and neuropsychiatric correlates of anosognosia in dementia. Last, we fully subscribed to the bio-psycho-social framework [71, 87] emphasizing the role in anosognosia development of the social environment, stigma, and caregivers.
Metacognitive Functions Involved
Each session starts with a pre-task procedure designed to elicit IntAw and AntAw, including:
- Exhaustive instructions, also providing pre-task examples, so that the subject is enabled to frame a mental hypothesis of the situation.
- A subject’s prevision about his/her future performance (e.g., the number of words expected to remember and a sort of vote from 0 to 10), which the clinician records.
- An estimate of the same task performed ten years ago to stimulate a realistic update of self-image.
This phase stimulates ongoing self-monitoring, error learning, feeling-of-knowing, judgment of learning, and self- image adjustment. Once the task is completed, a post-task procedure is administered to boost EmAw: the subject is required to judge his/her performance again by the above- described twofold judgment system (e.g., the actual number of words he/she correctly recalled and a vote from 0 to 10). Also, some tasks include questions about possible mistakes made in the task (e.g., the inclusion of intrusive words in a list to recall).
After the post-task inquiry, the subject is informed about his/her actual results in terms of objective scores [88], number of errors, possible intrusions, and omissions, as well as objective terms of comparison (e.g., the minimum and maximum score reachable at each task). Thus, the subject is asked to re-estimate his/her result based on objective information received. The subject is also encouraged to compare his pre-task expectations and post-task judgments with actual results. This final stage of the session aims to improve the Integration of External Feedback (IEF), which in turn is hypothesized to improve IntAw and AntAw, thus a correct update of self-knowledge. The introduction of this IEF index is due to evidence of difficulty in efficiently using external corrective information in neuropsychiatric patients with poor awareness of deficits [89, 90, 91]. The pre-, post, and external feedback procedures are reported in Table 1.
| Task Stimuli | Description | Metacognitive Function |
|---|---|---|
| Pre-Task Inquiry | The subject is asked to decide about his next task performance. | The subject is stimulated to rely on his present knowledge about the self. Elicitation of IntAw. and AntAw. |
| Post-Task Inquiry | The subject is asked to make a judgment after his performance | The subject is stimulated to gain awareness about his/her actions, regardless of previous expectations. Elicitation of EmAw. |
| External Feedback | The subject is informed about his objective results and is asked to adjust his post-task judgment and compare it with previous estimations. | The subject is confronted with objective evidence and his/her own subjective biases in self-appraisal. Elicitation of Em.Aw. and IEF, an adjustment in IntAw and AntAw |
Table 1: Metacognitive Indices, Task Description, and Related Awareness Functions Elicited.
Some sessions require the patient to watch a video with a third unknown person performing some tasks to stimulate the first-vs-third person appraisal. In the end, the patient is asked to express post-task judgments and to compare the third person’s result with his/her results. This type of intervention is justified by the evidence in the literature of the tendency of anosognosic patients to evaluate more correctly third- person performance than one’s own [43, 92, 93], supporting the hypothesis that perspective taking and agency represent independent but interacting constituents of self-awareness [94, 95]. Some sessions also include exercises of imagery boosting self-reflection and inner attention, which underpin self-awareness function [96, 97, 98, 99, 100].
The MGM-P Protocol
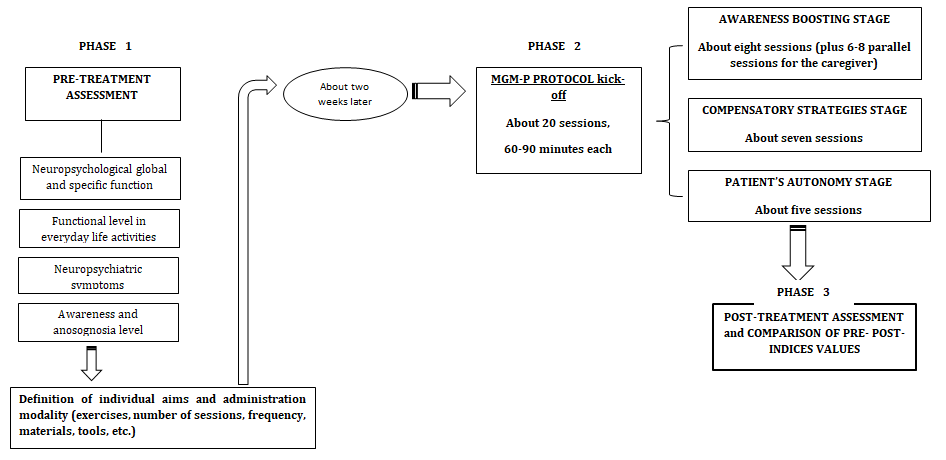
Before starting rehabilitative training, a comprehensive multidimensional assessment is strongly recommended. This information will then be used to formulate a diagnostic hypothesis and to tailor the sessions and the exercises according to individual needs. In particular, we suggest investigating: i) In addition to the global level of cognition, the presence of specific deficits in mnestic and executive function, working memory, abstract thinking, praxis, and language; ii) Residual functional abilities relative to daily life; iii) Depressive, apathetic or other neuropsychiatric symptoms frequently associated with anosognosia.
Note that, at this stage, a multifaceted awareness assessment is mandatory. Questionnaires investigating the main facets of self-awareness and anosognosia, e.g., semantic and episodic dimensions of illness, beliefs about memory and illness and related stigma, psychological denial, and implicit awareness, should always be considered [8, 78, 101, 102]. Also, a post-treatment re-administration would be desirable to verify changes in self-awareness and related constructs. Structure of the Sessions: The MGM-P consists of about twenty individual sessions of 60-90 minutes each, with a suggested frequency of twice a week for mild-to-moderate AD and once a week for SCC and MCI. In each session, the subject is presented with a minimum of one to a maximum of three tasks, according to his/her cognitive level. The tasks pertain to mnestic function (semantic, episodic/autobiographical, prospective, procedural, declarative), language (production, comprehension), executive function (selective and sustained attention, resistance to interferences, working memory), praxis skills and ideomotor learning and imitation (e.g., copy and recall of drawings, gestures imitation), cognitive control, cognitive flexibility (generation of alternative hypothesis, choice of the best alternative, stimulation of divergent thinking, problem-solving), spatial and temporal orientation, Theory of Mind. Verbal (auditory and written) and visual (e.g., pictures, videos) content are alternated. Some exercises are pen-and-pencil, while others require specific equipment. Touchscreen technology can also execute others.
This adaptation allows for lightening the equipment and recording results and data with greater precision. However, these exercises can be performed according to the patient’s cognitive level and cultural background. Some tasks are structured to facilitate an approach that is as ecological as possible, such as shopping, housekeeping, cooking, money handling, and orienting in space. Notably, the protocol can be subdivided into three stages: i) The awareness boosting stage, which represents the initial phase of the protocol. It is aimed to compel the patient to become aware of subjective biases in self-appraisal and to correct them; ii) The compensatory strategies stage: to overcome cognitive difficulties and to adjust to spared cognitive resources, compensatory cognitive strategies are introduced during each session. The therapist suggests various cognitive and pragmatic strategies to apply in different everyday contexts and situations to select and reinforce the best-fitting ones for the individual. In this stage, active cooperation between the therapist and the patient is crucial. Moreover, learning new ways to manage everyday difficulties and mainly focusing on makings rather than on failures promotes the patient’s empowerment, thus buffering possible anxious and depressive reactions; iii) Patient’s autonomy stage: the patient is asked to perform a series of tasks, not only estimating his/ her results but also applying the learned strategies without an active intervention of the therapist. The respective length of each of these stages of the protocol is only approximately fixed, as it is managed by the therapist based on individual cognitive demands and resources (Figure 2).
Active Involvement of Caregivers: Caregivers’ correct understanding of the patient’s deficits is fundamental for befitting assistance and proper preventative measures. However, judgments on patients’ deficits can be conditioned by burden and stress or by psychological denial, so some caregivers can overestimate or underestimate patients’ cognitive deficits and functional difficulties [45, 72, 103]. The first stage of the MGM-P includes six parallel sessions dedicated to the caregiver. Specifically, the caregiver is required to perform the same tasks the patient previously performed and formulate post-task judgments about his/her performance. Then, the caregiver has to guess the patient’s result at the same task. Eventually, the caregiver is told about the actual result obtained by the patient and is asked to make a new evaluation. This process is supposed to compel the caregiver to gain a realistic perspective on the patient’s capabilities.
Conclusion
In this paper, we have introduced the MGM-P model, an innovative rehabilitation protocol aimed at boosting self- awareness function and thus contrasting anosognosia in the elderly. The suggestion to intervene in self-awareness dysfunction in dementia had previously been highlighted [43, 45]. For instance, according to the CAM model [86], patients with executive anosognosia may benefit from treatments focused on error monitoring. In contrast, patients with mnemonic anosognosia may benefit from memory rehabilitation techniques enhancing recollection and consolidation of current personal knowledge. However, to our knowledge, this is the first rehabilitative approach to contrast anosognosia characterized by a scheduled program of sessions.
Furthermore, MGM-P can be fruitfully adopted as a preventive measure, too. The MGM-P protocols are specific not only for AD patients but also for pre-dementia subjects (i.e., SCD and MCI) have been developed. Given the increasing evidence of anosognosia as a predictor of conversion into AD [47, 104, 105], self-monitoring enhancement in pre-clinical and pre-symptomatic stages of the illness hampers the possibility to detect as early as possible changes in cognitive function.
The Specific Aims of the MGM-P are
• To stimulate correct self-image adjustments and
semantic knowledge about the self (IntAw). In turn, this is expected to overcome the frequent limit of previous approaches to unawareness, the temporary effect of rehabilitation.
- To promote an aware and willful adoption of strategies to face and overcome deficits. We all learn some cognitive compensative strategies, but most can be used unconsciously [106]. We hypothesize that changes in cognitive resources due to aging make this automatic use of strategies progressively less efficient. Thus, encouraging the subject to adopt aware solutions best tailored to the new needs is expected to ameliorate his/ her adaption in daily life.
- To favor better compliance to treatment and improved quality of life in terms of greater self-safety, autonomy in daily life activities, sense of self-efficacy, reduced self- stigma, and decreased caregivers’ stress and burden.
Although easily adoptable in different clinical contexts, the MGM-P administration requires a specialized training course, as it postulates specific knowledge in aging neuroscience and neuropsychology, high-order metacognitive processes, and self-awareness processes. Last but not least, it is characterized by a peculiar clinical attitude. The complex relationship between higher awareness of deficits and increased depression [45, 107] is frequently pointed out in AD [64, 101, 102, 108, 109] as well as in other neuropsychiatric conditions, such as Parkinson’s Disease [110], psychosis [111, 112, 113] and brain injured subjects [114, 115], cannot be disregarded. Depression may entail a negative bias when reporting problems, as subjects with low mood would better recall their failures and thus would tend to exaggerate the perception of deficit [116, 117, 118]. On the other hand, it is very intuitive that subjects aware of their new deficits may be more susceptible to depressive mood [72] and thus defensive denial. Thus, rehabilitation of metacognitive function must consider mood and motivational aspects [68, 119] and requires the ability to identify different components of denial of deficits. Experimental trials to provide data supporting the efficacy of MGM-P in clinical populations are required. Indeed, the inclusion in the protocol of quantitative indices (i.e., IntAw, EmAw. and IEF) facilitates the development of appropriate research designs.
Conflict of Interest Disclosure
The authors have no conflicts of interest to declare.
References
-
Dubois B, Villain N, Frisoni GB, Rabinovici GD, Sabbagh M, et al. (2021) Clinical diagnosis of Alzheimer’s disease: Recommendations of the International Working Group. The Lancet Neurology 20(6): 484-496.
-
Vermunt L, Sikkes SAM, Den Hout AV, Handels R, Bos I, et al. (2019) Duration of pre-clinical, prodromal, and dementia stages of Alzheimer’s disease in relation to age, sex, and APOE genotype. Alzheimers Dement 15(7): 888-898.
-
Lane CA, Hardy J, Schott JM (2018) Alzheimer’s disease. European Journal of Neurology 25(1): 59-70.
-
Dubois B, Hampel H, Feldman HH, Scheltens P, Aisen P, et al. (2016) Pre-clinical Alzheimer’s disease: Definition, natural history, and diagnostic criteria. Alzheimer’s & Dementia 12(3): 292-323.
-
Jongsiriyanyong S, Limpawattana P (2018) Mild Cognitive Impairment in Clinical Practice: A Review Article. Am J Alzh Dis Other Demen 33(8): 500-507.
-
Sanford AM (2017) Mild Cognitive Impairment. Clin Geriatr Med 33(3): 325-337.
-
Cacciamani F, Houot M, Gagliardi G, Dubois B, Sikkes S, et al. (2021) Awareness of Cognitive Decline in Patients With Alzheimer’s Disease: A Systematic Review and Meta-Analysis. Frontiers in Aging Neuroscience 13: 697234.
-
Clare L (2004) The construction of awareness in early- stage Alzheimer’s disease: a review of concepts and models. Br J Clin Psychol 43(2): 155-175.
-
Lacerda IB, Santos RL, Belfort T, Neto JPS, Dourado MCN (2018) Patterns of discrepancies in different objects of awareness in mild and moderate Alzheimer’s disease. Aging & Mental Health 26(5): 789-796.
-
Kaszniak A, Edmonds E (2009) Anosognosia and Alzheimer’s Disease: Behavioral studies. In: Prigatano GP (Ed.), The study of anosognosia. Oxford University Press, New York, USA, pp: 189-227.
-
Babinski J (1914) Contribution to the study of mental disorders in organic cerebral hemiplegia (Anosognosia). Rev Neurol 27: 845-847.
-
Conde Sala JL, Turro Garriga O, Pinan Hernandez S, Portellano Ortiz C, Vinas Diez V, et al. (2016) Effects of anosognosia and neuropsychiatric symptoms on the quality of life of patients with Alzheimer’s disease: a 24-month follow-up study. Int J Geriatr Psychiatry 31(2): 109-119.
-
Turro Garriga O, Garre Olmo J, Rene Ramirez R, Calvo Perxas L, Gascon Bayarri J, et al. (2016) Consequences of Anosognosia on the Cost of Caregivers’ Care in Alzheimer’s Disease. J Alzheimers Dis 54: 1551-1560.
-
Turro Garriga O, Garre Olmo J, Vilalta Franch J, Conde Sala JL, Gracia Blanco MD, et al. (2013) Burden associated with the presence of anosognosia in Alzheimer’s disease. Int J Geriatr Psychiatry 28(3): 291-297.
-
Lopez A, Caffò AO, Bosco A (2018) Topographical disorientation in aging. Familiarity with the environment does matter. Neurological Sciences 39(9): 1519-1528.
-
Okonkwo OC, Spitznagel MB, Alosco ML, Tremont G (2010) Associations among measures of awareness of cognitive deficits in dementia. Alzheimers Dement 6(4): 312-318.
-
Gallassi R, Bisulli A, Oppi F, Poda R, Di Felice C (2008) Subjective cognitive complaints, neuropsychological performance, affective and behavioral symptoms in non- demented patients. International Journal of Geriatric Psychiatry 23(1): 95-101.
-
Starkstein SE, Jorge R, Mizzahi R, Adrian J, Robinson RG (2007) Insight and danger in Alzheimer’s disease. Eur J Neurol 14(4): 455-460.
-
Clare L (2003) Managing threats to self: awareness in early-stage Alzheimer’s disease. Soc Sci Med 57(6): 1017-1029.
-
Cotrell V, Wild K (1999) Longitudinal study of self- imposed driving restrictions and deficit awareness in patients with Alzheimer’s disease. Alzheimer Dis Assoc Disord 13(3): 151-156.
-
Therriault J, Ng KP, Pascoal TA, Mathotaarachchi S, Kang MS, et al. (2018) Anosognosia predicts default mode network hypometabolism and clinical progression to dementia. Neurology 90(11): e932-e939.
-
Fragkiadaki S, Kontaxopoulou D, Beratis IN, Andronas N, Economou A, et al. (2016) Self-awareness of cognitive efficiency: Differences between healthy elderly and patients with mild cognitive impairment (MCI). J Clin Exp Neuropsychol 38(10): 1144-1157.
-
Ryu SY, Lee SB, Kim TW, Lee TJ (2016) Subjective memory complaints, depressive symptoms, and instrumental activities of daily living in mild cognitive impairment. Int Psychogeriatr 28(3): 487-494.
-
Scherling CS, Wilkins SE, Zakrezewski J, Kramer JH, Miller BL, et al. (2016) Decreased Self-Appraisal Accuracy on Cognitive Tests of Executive Functioning Is a Predictor of Decline in Mild Cognitive Impairment. Frontiers in Aging Neuroscience 8: 120.
-
Mak E, Chin R, Ng LT, Yeo D, Hameed S (2015) Clinical associations of anosognosia in mild cognitive impairment and Alzheimer’s disease. Int J Geriatr Psychiatry 30(12): 1207-1214.
-
Tremont G, Alosco ML (2011) Relationship between cognition and awareness of deficit in mild cognitive impairment. Int J Geriatr Psychiatry 26(3): 299-306.
-
Orfei MD, Varsi AE, Blundo C, Celia E, Casini AR, et al. (2010) Anosognosia in mild cognitive impairment and mild Alzheimer’s disease: frequency and neuropsychological correlates. Am J Geriatr Psychiatry 18(12): 1133-1140.
-
Hanyu H, Sato T, Akai T, Shimizu S, Hirao K, et al. (2008) Neuroanatomical correlates of unawareness of memory deficits in early Alzheimer’s disease. Dement Geriatr Cogn Disord 25(4): 347-353.
-
Collie A, Maruff P, Currie J (2002) Behavioral characterization of mild cognitive impairment. J Clin Exp Neuropsychol 24(6): 720-733.
-
Tabert MH, Albert SM, Borukhova Milov L, Camacho Y, Pelton G, et al. (2002) Functional deficits in patients with mild cognitive impairment: prediction of AD. Neurology 58(5): 758-764.
-
Jessen F, Amariglio RE, Buckley RF, Van Der Flier WM, Han Y, et al. (2020) The characterization of subjective cognitive decline. Lancet Neurol 19(3): 271-278.
-
Lin Y, Shan PY, Jiang WJ, Sheng C, Ma L (2019) Subjective cognitive decline: Pre-clinical manifestation of Alzheimer’s disease. Neurol Sci 40(1): 41-49.
-
Cheng YW, Chen TF, Chiu MJ (2017) From mild cognitive impairment to subjective cognitive decline: Conceptual and methodological evolution. Neuropsychiatr Dis Treat 13: 491-498.
-
Abner EL, Kryscio RJ, Caban Holt AM, Schmitt FA (2015) Baseline subjective memory complaints associated with increased risk of incident dementia: The preadvise trial. J Prev Alzheimers Dis 2(1): 11-16.
-
Dalla Barba G, La Corte V, Dubois B (2015) For a Cognitive Model of Subjective Memory Awareness. J Alzheimers Dis 48(1): 57-61.
-
Kaup AR, Nettiksimmons J, LeBlanc ES, Yaffe K (2015) Memory complaints and risk of cognitive impairment after nearly 2 decades among older women. Neurology 85(21): 1852-1858.
-
Slavin MJ, Sachdev PS, Kochan NA, Woolf C, Crawford JD, et al. (2015) Predicting Cognitive, Functional, and Diagnostic Change over 4 Years Using Baseline Subjective Cognitive Complaints in the Sydney Memory and Ageing Study. Am J Geriatr Psychiatry 23(9): 906-914.
-
Jessen F, Wolfsgruber S, Wiese B, Bickel H, Mosch E, et al. (2014) AD dementia risk in late MCI, in early MCI, and in subjective memory impairment. Alzheimers Dement 10(1): 76-83.
-
Mitchell AJ, Beaumont H, Ferguson D, Yadegarfar M, Stubbs B (2014) Risk of dementia and mild cognitive impairment in older people with subjective memory complaints: meta-analysis. Acta Psychiatr Scand 130(6): 439-451.
-
Tales A, Wilcock GK, Phillips JE, Bayer A (2014) Is there more to subjective cognitive impairment than meets the eye? A perspective. J Alzheimers Dis 41(3): 655-661.
-
Wang Y, Risacher SL, West JD, McDonald BC, Magee TR, et al. (2013) Altered default mode network connectivity in older adults with cognitive complaints and amnestic mild cognitive impairment. J Alzheimers Dis 35(4): 751- 760.
-
Bertrand E, Azar M, Rizvi B, Brickman AM, Huey ED, et al. (2018) Cortical thickness and metacognition in cognitively diverse older adults. Neuropsychology 32(6): 700-710.
-
Bertrand E, Landeira Fernandez J, Mograbi DC (2016) Metacognition and Perspective-Taking in Alzheimer’s Disease: A Mini-Review. Front Psychol 7: 1812.
-
Flavell J (1979) Metacognition and cognitive monitoring: A new area of cognitive-developmental inquiry. Am Psychol 34(10): 906-911.
-
Starkstein SE (2014) Anosognosia in Alzheimer’s disease: Diagnosis, frequency, mechanism and clinical correlates. Cortex 61: 64-73.
-
Caddell LS, Clare L (2013) Studying the self in people with dementia: how might we proceed? Dementia (London) 12(2): 192-209.
-
Vannini P, Amariglio R, Hanseeuw B, Johnson KA, McLaren DG, et al. (2017) Memory self-awareness in the pre-clinical and prodromal stages of Alzheimer’s disease. Neuropsychologia 99: 343-349.
-
Senturk G, Bilgic B, Arslan AB, Bayram A, Hanagasi H, et al. (2016) Cognitive and anatomical correlates of anosognosia in amnestic mild cognitive impairment and early-stage Alzheimer’s disease. Int Psychogeriatrics 29(2): 293-302.
-
Hannesdottir K, Morris RG (2007) Primary and secondary anosognosia for memory impairment in patients with Alzheimer’s disease. Cortex 43(7): 1020-1030.
-
Salmon E, Perani D, Herholz K, Marique P, Kalbe E, et al. (2006) Neural correlates of anosognosia for cognitive impairment in Alzheimer’s disease. Hum Brain Mapp 27: 588-597.
-
Starkstein SE, Jorge R, Mizrahi R, Robinson RG (2006) A diagnostic formulation for anosognosia in Alzheimer’s disease. J Neurol Neurosurg Psychiatry 77(6): 719-725.
-
Marková IS, Berrios GE, Hodges JR (2004) Insight into memory function. Neurol Psychiatry and Brain Res 11: 115-126.
-
Hallam B, Chan J, Sergi GC, Bhome R, Huntley J (2020) What are the neural correlates of meta-cognition and anosognosia in Alzheimer’s disease? A systematic review. Neurobiol Aging 94: 250-264.
-
Tondelli M, Barbarulo AM, Vinceti G, Vincenzi C, Chiari A, et al. (2018) Neural Correlates of Anosognosia in Alzheimer’s Disease and Mild Cognitive Impairment: A Multi-Method Assessment. Front Behav Neurosci 12: 100.
-
Berlingeri M, Ravasio A, Cranna S, Basilico S, Sberna M, et al. (2015) Unrealistic representations of the self: A cognitive neuroscience assessment of anosognosia for memory deficit. Conscious Cogn 37: 160-177.
-
Perrotin A, Desgranges B, Landeau B, Mezenge F, La Joie R, et al. (2015) Anosognosia in Alzheimer disease: Disconnection between memory and self-related brain networks. Ann Neurol 78(3): 477-486.
-
Zamboni G, Drazich E, McCulloch E, Filippini N, Mackay CE, et al. (2013) Neuroanatomy of impaired self- awareness in Alzheimer’s disease and mild cognitive impairment. Cortex 49(3): 668-678.
-
Amanzio M, Torta DM, Sacco K, Cauda F, D’Agata F, et al. (2011) Unawareness of deficits in Alzheimer’s disease: role of the cingulate cortex. Brain 134(4): 1061-1076.
-
Rosen HJ, Alcantar O, Rothlind J, Sturm V, Kramer JH, et al. (2010) Neuroanatomical correlates of cognitive self- appraisal in neurodegenerative disease. Neuroimage 49(4): 3358-3364.
-
Shibata K, Narumoto J, Kitabayashi Y, Ushijima Y, Fukui K (2008) Correlation between anosognosia and regional cerebral blood flow in Alzheimer’s disease. Neurosci Lett 435(1): 7-10.
-
Tondelli M, Galli C, Vinceti G, Fiondella L, Salemme S, et al. (2021) Anosognosia in Early-and Late-Onset Dementia and Its Association With Neuropsychiatric Symptoms. Front Psychiatry 12: 658934.
-
Yoon B, Shim YS, Hong YJ, Choi SH, Park HK, et al. (2017) Anosognosia and Its Relation to Psychiatric Symptoms in Early-Onset Alzheimer Disease. J Geriatr Psychiatry Neurol 30(3): 170-177.
-
Turro Garriga O, Garre Olmo J, Calvo Perxas L, Rene Ramirez R, Gascon Bayarri J, et al. (2016) Course and Determinants of Anosognosia in Alzheimer’s Disease: A 12-Month Follow-up. J Alzheimers Dis 51(2): 357-366.
-
Horning SM, Melrose R, Sultzer D (2014) Insight in Alzheimer’s disease and its relation to psychiatric and behavioral disturbances. Int J Geriatr Psychiatry 29(1): 77-84.
-
Spalletta G, Girardi P, Caltagirone C, Orfei MD (2012) Anosognosia and neuropsychiatric symptoms and disorders in mild Alzheimer’s disease and mild cognitive impairment. J Alzheimers Dis 29(4): 761-772.
-
Starkstein SE, Brockman S, Bruce D, Petracca G (2010) Anosognosia is a significant predictor of apathy in Alzheimer’s disease. J Neuropsychiatry Clin Neurosci 22(4): 378-383.
-
Markova IS, Clare L, Whitaker CJ, Roth I, Nelis SM, et al. (2014) Phenomena of awareness in dementia: heterogeneity and its implications. Conscious Cogn 25: 17-26.
-
Rosen HJ (2011) Anosognosia in neurodegenerative disease. Neurocase 17(3): 231-241.
-
Marková IS, Berrios GE (2006) Approaches to the assessment of awareness: conceptual issues. Neuropsychol Rehabil 16(4): 439-455.
-
Antoine C, Antoine P, Guermonprez P, Frigard B (2004) Awareness of deficits and anosognosia in Alzheimer’s disease. L Encephale 30(6): 570-577.
-
Ownsworth T, Clare L, Morris R (2006) An integrated biopsychosocial approach to understanding awareness deficits in Alzheimer’s disease and brain injury. Neuropsychol Rehabil 16(4): 415-438.
-
Clare L, Wilson BA, Carter G, Roth I, Hodges JR (2004) Awareness in early-stage Alzheimer’s disease: relationship to outcome of cognitive rehabilitation. J Clin Exp Neuropsychol 26: 215-226.
-
Trouillet R, Gely Nargeot MC, Derouesne C (2003) Unawareness of deficits in Alzheimer’s disease: a multidimensional approach. Psychol Neuropsychiatr Vieil 1(2): 99-110.
-
Zimmermann N, Mograbi DC, Hermes Pereira A, Fonseca RP, Prigatano GP (2017) Memory and executive function correlates of self-awareness in traumatic brain injury. Cogn Neuropsychiatry 22(4): 346-360.
-
Al Aloucy MJ, Cotteret R, Thomas P, Volteau M, Benmaou I, et al. (2011) Unawareness of memory impairment and behavioral abnormalities in patients with Alzheimer’s disease: relation to professional health care burden. J Nutr Health Aging 15(5): 356-360.
-
Logsdon RG, Pike KC, McCurry SM, Hunter P, Maher J, et al. (2010) Early-stage memory loss support groups: outcomes from a randomized controlled clinical trial. J Gerontol B Psychol Sci Soc Sci 65(6): 691-697.
-
Prigatano GP (2005) Disturbances of self-awareness and rehabilitation of patients with traumatic brain injury: a 20-year perspective. J Head Trauma Rehabil 20(1): 19- 29.
-
Mograbi DC, Morris RG (2013) Implicit awareness in anosognosia: clinical observations, experimental evidence, and theoretical implications. Cogn Neurosci 4(3-4): 181-197.
-
Souchay C, Isingrini M (2012) Are feeling-of-knowing and judgment-of-learning different? Evidence from older adults. Acta Psychol (Amst) 139(3): 458-464.
-
Thomas AK, Bulevich JB, Dubois SJ (2012) An analysis of the determinants of the feeling of knowing. Conscious Cogn 21(4): 1681-1694.
-
Barco PP, Crosson B, Bolesta MM, Werst D, Stout R (1991) Training awareness and compensation in post- acute brain injury rehabilitation. Kreutzer J, Wehman P, (Eds.), In: Cognitive rehabilitation for persons with traumatic brain injury: a functional approach. Baltimore, Maryland: Paul H. Brookes Publishing Company, USA, pp: 129-147.
-
Metcalfe J, Son L (2012) 18 Anoetic, Noetic and Autonoetic Metacognition. Beran M, Brandl J, et al. (Eds.), In: The Foundations of Metacognition. Oxford, Oxford University Press, UK, pp: 289-301.
-
Fossati P, Hevenor SJ, Lepage M, Graham SJ, Grady C, et al. (2004) Distributed self in episodic memory: neural correlates of successful retrieval of self-encoded positive and negative personality traits. Neuroimage 22(4): 1596-1604.
-
Mograbi DC, Brown RG, Morris RG (2009) Anosognosia in Alzheimer’s disease--the petrified self. Conscious Cogn 18(4): 989-1003.
-
Crosson C, Barco PP, Velozo C, Bolesta MM, Cooper PV, et al. (1989) Awareness and compensation in post-acute head injury rehabilitation. J Head Trauma Rehabil 4(3): 46-54.
-
Morris RG, Mograbi DC (2013) Anosognosia, autobiographical memory and self-knowledge in Alzheimer’s disease. Cortex 49(6): 1553-1565.
-
Clare L, Markova IS, Roth I, Morris RG (2011) Awareness in Alzheimer’s disease and associated dementias: theoretical framework and clinical implications. Aging Ment Health 15(8): 936-944.
-
DeLozier SJ, Davalos D (2016) A Systematic Review of Metacognitive Differences Between Alzheimer’s Disease and Frontotemporal Dementia. Am J Alzheimers Dis Other Demen 31(5): 381-388.
-
Spalletta G, Piras F, Sancesario G, Iorio M, Fratangeli C, et al. (2014) Neuroanatomical correlates of awareness of illness in patients with amnestic mild cognitive impairment who will or will not convert to Alzheimer’s disease. Cortex 61: 183-195.
-
Orfei MD, Spoletini I, Banfi G, Caltagirone C, Spalletta G (2010) Neuropsychological correlates of cognitive insight in schizophrenia. Psychiatry Res 178(1): 51-56.
-
Beck AT, Baruch E, Balter JM, Steer RA, Warman DM (2004) A new instrument for measuring insight: the Beck Cognitive Insight Scale. Schizophr Res 68(2): 319- 329.
-
Marcel AJ, Tegner R, Nimmo-Smith I (2004) Anosognosia for plegia: specificity, extension, partiality, and disunity of bodily unawareness. Cortex 40(1): 19-40.
-
Ramachandran VS (1995) Anosognosia in parietal lobe syndrome. Conscious Cogn 4(1): 22-51.
-
David N, Bewernick BH, Cohen MX, Newen A, Lux S, et al. (2006) Neural representations of self versus other: visual-spatial perspective taking and agency in a virtual ball-tossing game. J Cogn Neurosci 18(6): 898-910.
-
Vogeley K, May M, Ritzl A, Falkai P, Zilles K, et al. (2004) Neural correlates of first-person perspective as one constituent of human self-consciousness. J Cogn Neurosci 16(5): 817-827.
-
Synofzik M, Vosgerau G, Newen A (2008) I move, therefore I am: a new theoretical framework to investigate agency and ownership. Conscious Cogn 17(2): 411-424.
-
Northoff G, Heinzel A, de Greck M, Bermpohl F, Dobrowolny H, et al. (2006) Self-referential processing in our brain--a meta-analysis of imaging studies on the self. Neuroimage 31(1): 440-457.
-
Newen A, Vogeley K (2003) Self-representation: searching for a neural signature of self-consciousness. Conscious Cogn 12(4): 529-543.
-
Johnson SC, Baxter LC, Wilder LS, Pipe JG, Heiserman JE, et al. (2002) Neural correlates of self-reflection. Brain 125(pt 8): 1808-1814.
-
Kjaer TW, Nowak M, Lou HC (2002) Reflective self- awareness and conscious states: PET evidence for a common midline parietofrontal core. Neuroimage 17(2): 1080-1086.
-
Mograbi DC, Morris RG (2014) On the relation among mood, apathy, and anosognosia in Alzheimer’s disease. J Int Neuropsychol Soc 20(1): 2-7.
-
Mullen R, Howard R, David A, Levy R (1996) Insight in Alzheimer’s Disease. Int J Geriatr Psychiatry 11(7): 645-651.
-
Paton J, Johnston K, Katona C, Livingston G (2004) What causes problems in Alzheimer’s disease: attributions by caregivers. A qualitative study. Int J Geriatr Psychiatry 19: 527-532.
-
Cacciamani F, Tandetnik C, Gagliardi G, Bertin H, Habert MO, et al. (2017) Low Cognitive Awareness, but Not Complaint, is a Good Marker of Pre-clinical Alzheimer’s Disease. J Alzheimers Dis 59(2): 753-762.
-
Gerretsen P, Chung JK, Shah P, Plitman E, Iwata Y, et al. (2017) Anosognosia Is an Independent Predictor of Conversion From Mild Cognitive Impairment to Alzheimer’s Disease and Is Associated With Reduced Brain Metabolism. J Clin Psychiatry 78(9): 1187-1196.
-
Kentridge RW, Heywood CA (2000) Metacognition and awareness. Conscious Cogn 9(2): 308-312.
-
Smith CA, Henderson VW, McCleary CA, Murdock GA, Buckwalter JG (2000) Anosognosia and Alzheimer’s disease: the role of depressive symptoms in mediating impaired insight. J Clin Exp Neuropsychol 22(4): 437- 444.
-
OConnell ME, Dal Bello Haas V, Crossley M, Morgan D (2014) Clinical correlates of awareness for balance, function, and memory: evidence for the modality specificity of awareness. J Aging Res 2014(674716): 1-12.
-
Verhulsdonk S, Quack R, Hoft B, Lange Asschenfeldt C, Supprian T (2013) Anosognosia and depression in patients with Alzheimer’s dementia. Arch Gerontol Geriatr 57(3): 282-287.
-
Ouzir M, Azorin JM, Adida M, Boussaoud D, Battas O (2012) Insight in schizophrenia: from conceptualization to neuroscience. Psychiatry Clin Neurosci 66(3): 167- 179.
-
Saeedi H, Addington J, Addington D (2007) The association of insight with psychotic symptoms, depression, and cognition in early psychosis: a 3-year follow-up. Schizophr Res 89(1-3): 123-128.
-
Moore O, Cassidy E, Carr A, O’Callaghan E (1999) Unawareness of illness and its relationship with depression and self-deception in schizophrenia. Eur Psychiatry 14(5): 264-269.
-
Orfei MD, Robinson RG, Prigatano GP, Starkstein S, Rusch N, et al. (2007) Anosognosia for hemiplegia after stroke is a multifaceted phenomenon: a systematic review of the literature. Brain 130(12): 3075-3090.
-
Prigatano GP, Klonoff PS (1998) A Clinician’s Rating Scale for evaluating impaired self-awareness and denial of disability after brain injury. Clin Neuropsychol 12(1): 56-67.
-
Oba H, Matsuoka T, Imai A, Fujimoto H, Kato Y, et al. (2018) Interaction between memory impairment and depressive symptoms can exacerbate anosognosia: a comparison of Alzheimer’s disease with mild cognitive impairment. Aging Ment Health 23(5): 595-601.
-
Bertrand E, Dourado MC, Laks J, Morris RG, Landeira Fernandez J, et al. (2016) Mood-congruent recollection and anosognosia in Alzheimer’s disease. Cortex 84: 55- 62.
-
Bower GH (1981) Mood and memory. Am Psychol 36(2): 129-148.
-
Misdrahi D, Denard S, Swendsen J, Jaussent I, Courtet P (2014) Depression in schizophrenia: the influence of the different dimensions of insight. Psychiatry Res 216(1): 12-16.
-
Sitek EJ, Soltan W, Wieczorek D, Robowski P, Slawek J (2011) Self-awareness of memory function in Parkinson’s disease in relation to mood and symptom severity. Aging Ment Health 15(2): 150-156.
- Systematic Review and Meta-analysis Investigating the Prevalence of Depression, Anxiety, Loneliness and Help seeking among International Students
- Family Experiences and their Interpretations as a Source of Adaptive Behaviour in Young Adults: A Qualitative Model of Adaptive Behaviour
- The Development of Responsibility in Teenage Mothers: A Qualitative Model
- Post-Truth Reality: Worldwide Infodemia and Mental Health Concerns during and Post COVID-19 Pandemic Scenarios
- Psycho-Emotional Rehabilitating Means of Overcoming Extreme and Stressful Impact
- The Paradox of Humbleness, Arrogance and the Concept of Fluid Individuality