Hirschsprung Diseases should be Treated by Single or Two Stage Operations? A Case Report in a Resource-Low Setting in Cameroon
Background: Hirschsprung disease is a developmental disorder characterized by the absence of ganglia in the distal colon, resulting in a functional obstruction. Hirsch sprung disease is common in the paediatric age group (neonatal period). They represent worldwide 1/1500-1/7000 new-born. The male: female ratio is 4:1. Case Report: We report the case of Hirsch sprung diseases diagnosed in a one month old neonate who presented with abdominal distension and recurrent constipation since birth. The past history was relevant for delay emission of meconium. A rectosigmoid contrast enema transition zone was observed and a diagnosis of hirschsprung disease was made. The patient was treated through asingle stage operation, trans-anal pull throughin YGOPH. Conclusion: Accurate reporting and creation of registry and data bases are important measures to curb the mortality and morbidity associated with this paediatric surgical condition
Marcelin3, Paul Nkemtedong Tolefac2 , Ngo Nonga Bernadette1 and Ze Minkande Jacqueline1,2
Cameroon
Cameroon, E-mail: gaeldongmo7@gmail.com
period). They represent worldwide 1/1500-1/7000 new-born. The male: female ratio is 4:1.
made. The patient was treated through asingle stage operation, trans-anal pull throughin YGOPH.
morbidity associated with this paediatric surgical condition
Introduction
Hirsch sprung disease was first described Ruysch in 1691 and popularized by Hirsch sprung in 1886. Aganglionic cell was visualized by Whitehouse and Kernohan in the middle 20th century. Many therapeutic procedures exist: Swenson procedure, Duhamel procedure, Soave procedure, anorectal myomectomy, procedure for long segment Hirsch sprung disease, laparoscopic approach, transanal pull-though and novel strategies. Hirsch sprung diseases represent worldwide 1/1500-1/7000 new-born [1], more common in boys than in girls [1]. In a study done in Cameroon, 43.3% of intestinal obstruction in children was due to Hirsch sprung disease [2]. Hirsch sprung disease is mainly a sporadic disease with only 10% being genetic. The Wu and colleagues diagnostic scoring system helps to make a diagnosis (age < 3years, failed/delayed passage of meconium, male child) [3]. On examination there is usually a patentanus and a distended abdomen. Investigations include: Erect plain abdominal x-ray (distended bowel loops and a restriction zone), barium enema (transition zone), 24 hr erect abdominal x-ray after barium enema (retension of rectal contrast) [4]. Today, the goal standard suction biopsy along the presumed pathologic colon could be done to delimitate the resection point. The treatment is surgical with transanal pull-through predominating at the YGOPH. Transanal pull-through is aesthetic, has less surgical site incisions, less risk of post-operative incontinence and a shorter operative time. The prognosis after treatment is good [5]. This report describes the case of Hirsch sprung diseases diagnosed in a one-month old neonate and treated in YGOPH by a single stage operation, trans-anal pull through.
Case Report
This is E.P. a 1month old male who presented with abdominal distension and recurrent constipationsince birth. The past history was relevant for delay emission of meconium(bulky mucoid stool) on day 4 of life. Several rectal lavage was performed by the parents at home. There was no vomiting, no bloody stool and no fever. On examination there were signs of respiratory distress. The conjunctivae were pink, sclere anicteric. Breath sound was vesicular. There was no added heart sound. Abdomen was distended (abdominal circumference 54cm) and soft. There was no abdominal tenderness, no hepatomegaly nor splenomegaly. Hernia orifices were free. Digital rectal examination reveiled bulky mucoid stool on removal of the examining finger. The presumptive diagnosis ofhirschsprung disease was made. With differentials of congenital megacolon and dolicocolon. The results of the investigations were as follows: erect plain abdominal x- ray shows hyper distended bowels with a recto sigmoid transition zone no sign of intestinal obstruction nor perforation (Figure 1), barium enema shows a rectosigmoid contrast enema transition zone (Figure 2), stool analysis (normal flora), FBC (normal leucocyte, erythrocyte and platelets count), PT (28sec), APTT (30sec), BUN (21mg/dl), Creatinine (1.1mg/dl), serum electrolyte (Na+: 132mEq/L, K+: 3.6 mEq/L), Blood group/ rhesus (A/+).
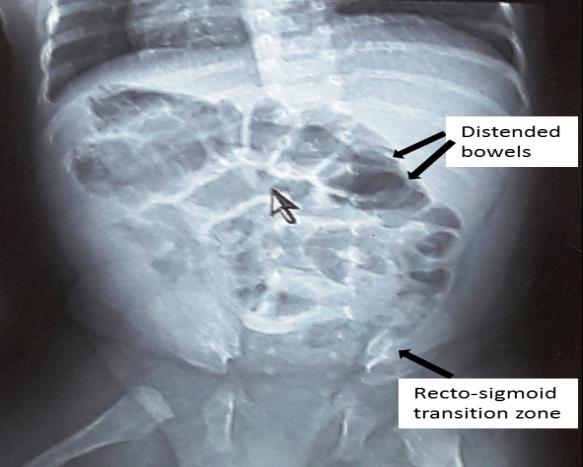
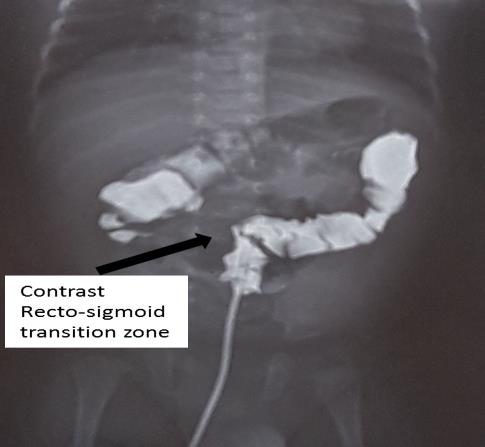
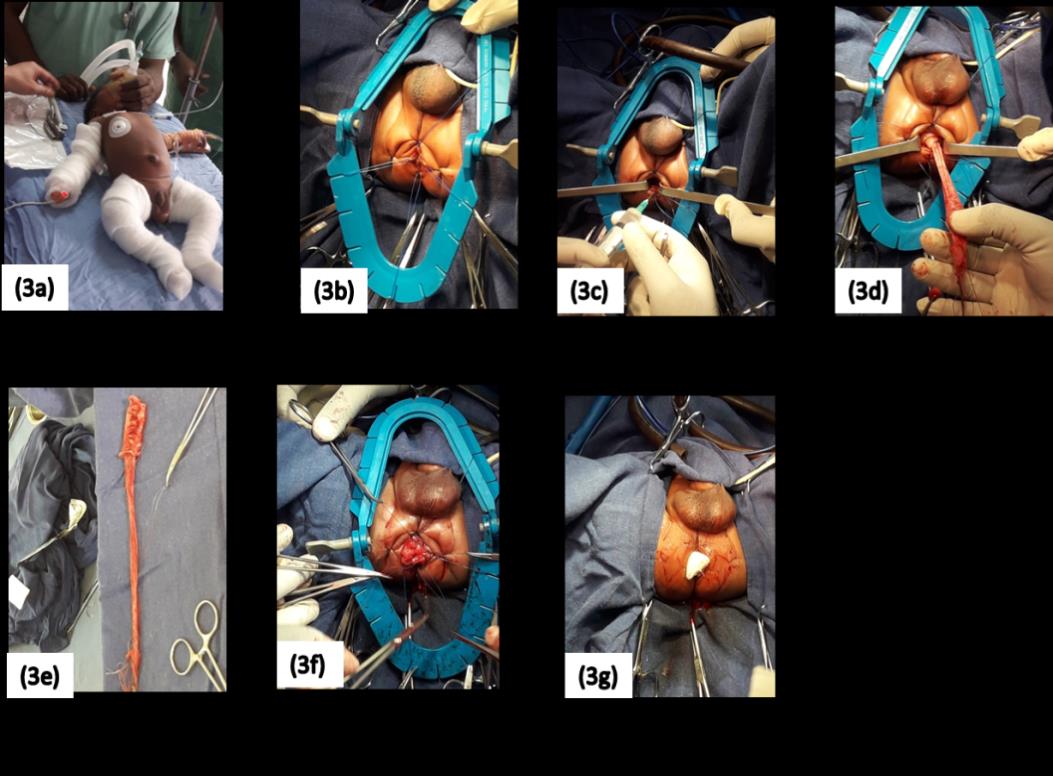
Figure 2: Contrast enema transition zone at the recto- sigmoid from YGOPH. Working diagnosis: Hirsch sprung disease. The management consisted of: pre-operatory hospitalisation, preoperatory bowel preparation, preoperative anesthetist consultation, senior paediatric surgeon’s reassessment, and peroperatory antibiotic prophilaxis. The surgical intervention (Figure 3) consisted of: transanal pull through during which with the patient lying on a paediatric surgical table in a lithotomy position with the limbs flexed and the anal orifice exposed, traction sutures are placed at the 4 cardinal points to allow eversion of the mucosa. In filtration of the submucosa 1cm above the pectineus line so as to ease dissection. 1cm of the anal mucosa is left in place. The rectum including its muscularis mucosa is pulled through the anal orifice and resected at the end of the sigmoidal dilatation followed by coloanal anastomosis by full thickness interrupted suture and finally removal of traction sutures.
Discussion
Epidemiology
Hirsch sprung disease represent worldwide 1/1500- 1/7000 new-born [1]. The male: female ratio is 4:1. Studies done in Cameroon (in a tertiary hospital) identified hirsch sprung disease as 43.3% of intestinal obstruction in children [2]. The main presenting complaints are: delayed passage of meconium, severe constipation, abdominal distension and bilious vomiting [6]. However, 60-90% of children with Hirsch sprung disease fail to pass meconium within 24-48 hours [5].
Diagnosis
Distendedabdomen is seen in 63-91% of neonates with, Hirsch sprung disease andbiliousvomitingin19-37%of children [5]. The indexed case described herein presented with distended abdomen. The Wu and colleagues diagnostic scoring system helps to make a clinical diagnosis [3]. Investigations include: Erect plain abdominal x-ray, barium enema, 24hr erect abdominal x- ray after barium enema and anorectalmanometry which identifies the presence of high base lineresting pressures and absence frecto-anal inhibitory reflex [5]. Plain abdominal x ray and barium enema were diagnostic in our index case. Anorectalmanometry is unnecessary to diagnose Hirsch sprung disease [7]. Sometime contrast enema could show a number of false negative Hirsch sprung disease (no transition zone) because this zone could easily be distended and distorted [8]. Multiple full thickness biopsy and rectal suction biopsy along the presumed pathologic colon could be done to delimitate the resection point. The findings are that of aganglionic cells and the presence acetylcholinesterase (AChE) as in the case described herein and positive hypertrophic nerve fiber [5]. Other histologic finding like hematology and eosin are cheaper, friendly and reliable although acetylcholinesterase is a useful diagnostic tool [7]. Signs of large bowel obstructions may not always be observed due to the repeated manual emptying of the rectum. Adequate intraoperative biopsy could help reduce the risk of false resection point [7].
Treatment
The treatment is surgically done in a single operation or a two stage operation by transanal, trans abdominal, laparoscopic, or open surgery [7]. Many technics are uses in the management of Hirsch sprung disease: swenson procedure, Duhamel procedure, soave (endorectal) procedure, anorectal myomectomy, procedure for long segment hirschs prung disease, laparoscopic approach, transanal pull-through procedure, modified transanal approach with trans abdominal open or laparoscopic assistance, single incision laparoscopicendorectal pull- through and natural orifice transluminal endoscopic surgery. Experimental technic include sterm cell transplantation and regenerative strategies [9]. In the indexed case described herein, we opted for a trans-anal pull through in a single stage operation. The limitation in the approach of management here is mainly due to a relatively blind resection of the defected colon. After post operatory biopsy the presence of aganglionic cells at the proximal segment could necessitate a second intervention.
Conclusion
Though relatively rare, the authors describe their experience in the management of this very important cause of neonatal and infantile intestinal obstruction. Creation of registry and data bases on the management of this disease in Africa are important starting points to improve the management and curb the morbidity and mortality of this disorder.
References
-
Meza-Valencia BE, de Lorimier AJ, Person DA (2005) Hirschsprung disease in the U.S. associated Pacific Islands: more common than expected. Hawaii Med J 64(4): 96-8, 100-1.
-
Mouafo FF Tambo, J Ditope, MV Tamtchap, G Fossi, BD Nyanit, et al. (2015) Facteurs de mortalite des occlusions neonatales a l’Hopital Gyneco-Obstetrique et Pediatrique de Yaounde. Revue Africaine de Chirurgie et Spécialités 9(3).
-
Wu XJ, Zhang HY, Li N, Yan MS, Wei J, et al. (2013) A new diagnostic scoring system to differentiate Hirschsprung's disease from Hirschsprung's disease- allied disorders in patients with suspected intestinal dysganglionosis. Int J Colorectal Dis 28(5): 689-696.
-
Justin P Wagner (2017) Hirschsprung disease.
-
Ramanath NH, Keith E Georgeson (2008) Hirschsprung disease. Seminarsin Pediatric Surgery 17(4): 266-275.
-
Tariq Burki, Liina Kiho, Irene Scheimberg, Simon Phelps, Devesh Misra, et al. (2011) Neonatal function alintestinal obstruction and the presence of severely immature ganglion cells on rectal biopsy: 6 year experience. Pediatr Surg Int 27(5): 487-490.
-
Giuseppe Martuccielloa, Alessio Pini Pratob, PremPuric, Alexander M. Holschneiderd, et al. (2005) Controversies concerning diagnostic guidelines for anomalies of the enteric nervous system: A report from the fourth International Symposium on Hirschsprung’s disease and related neurocristopathies. Journal of Pediatric Surgery 40(10): 1527-1531.
-
G Martucciello (2008) Hirschsprung’s Disease, One of the Most Difficult Diagnoses in Pediatric Surgery: A Review of the Problems from Clinical Practice to the Bench. Eur J Pediatr Surg 18(3): 140-149.
-
Thapar N (2009) New frontiers in the treatment of hirschsprung disease. J Pediatr Gastroenterol Nutr 48(2): S92-S94.
-
Heanue TA, Pachnis V (2007) Enteric nervous system development and Hirschsprung's disease: advances in genetic and stem cell studies. Nat Rev Neurosci 8(6): 466-479.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey