A Rare Case of Acute Ischemic Stroke in a Healthy Female Child
Acute ischemic stroke in a pediatric patient is a complex disease with a variety of etiologies that differ from adults. Though rare, delayed diagnosis is results in potentially devastating consequences. There are no clear guidelines for the management of stroke in children. We report a healthy 6 year old female child who presented with headache, unable to speak, deviation of mouth to left side, inability to use her right upper and lower limb when she woke up in the morning. She was evaluated and found to have acute middle cerebral artery territory infarcts. The patient was treated with antiplatelet drugs (aspirin), physiotherapy and recovered without any neurological deficit. The etiology of her stroke found to be arterial ischemic stroke due to arteriopathy. It is important to diagnose early and initiation of treatment results in good prognosis.
Introduction
Acute ischemic stroke (AIS) in a pediatric patient is a rare medical emergency with an incidence of 2-3 per 100,000 children [1]. The etiologies of stroke in children are more varied than in adults and are not always due to acute clot formation or hemorrhage. Studies in the adult population show anti-thrombotic drugs, including aspirin, are effective when administered using recommended guidelines [2]. The role of thrombolytics is controversial with conflicting evidence [3, 4, 5]. We report a case of 6 year old female child with middle cerebral artery territory infarcts. After exhaustive workup, the etiology of her stroke found to be arterial ischemic stroke due to arteriopathy.
A 6-year-old female presented to the emergency department of Chalmeda Ananda Rao Institute of Medical Sciences, Karimnagar which is a tertiary care center, with history of headache in the evening around 8pm. Next day morning when she woke up, unable to speak but was able to obey oral commands, and she developed weakness of right upper and lower limbs with deviation of mouth to left side. There is no history of fever, seizures, head injury, ear discharge, and no contact with Koch’s patient. Child was born to nonconsanguinous parents. Birth history is normal and there is no family history of similar complaints. On general physical examination child was moderately build, mild pallor, no icterus, clubbing, No
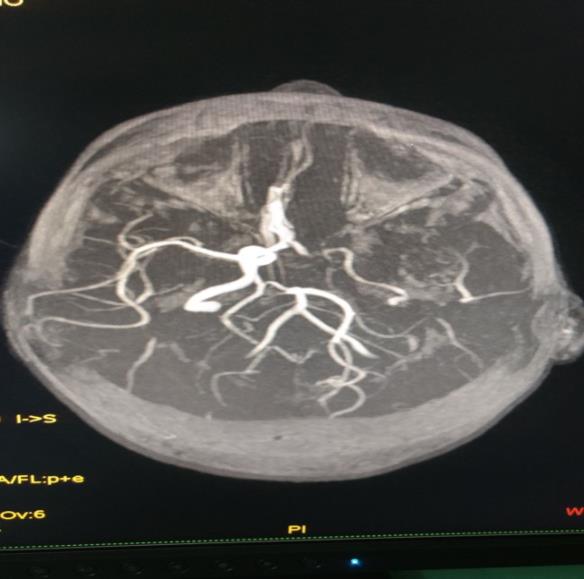
bleeding manifestations, no dysmorphic features, and no neurocutaneous markers. Her vital signs were within normal limits. On central nervous system examination power in right arm and leg were 2/5 with a noticeable facial droop. Other systems examination is normal. At the time of admission blood glucose with glucometer is normal. A CT scan of the head showed edema to the left frontoperitotemporal region without evidence of hemorrhage. An emergency MRI was done for further evaluation her imaging showed left middle cerebral artery territory infarcts (Figure 1). A thorough work-up ensued in the pediatric intensive care unit. An MRA of the brain showed atherosclerotic narrowing of left middle cerebral artery segments (Figure 2). Carotid Doppler and echocardiogram were normal. The CBC, chemistry panel, LFT, RFT, was normal. Coagulation profile including Protein C and S, Factor V Leiden, anti-phospholipid antibodies, and anti-thrombin III were normal.

The patient was treated with aspirin, intravenous antibiotics, fluids and physiotherapy. The child started showing improved within a week, child was discharged, and on follow up, no persistent neurological deficits found.
Discussion
AIS in a pediatric patient are defined as a stroke occurring between the ages of one month and 18 years. The reported annual incidence of cerebral infarction in children all over the world varies between 1.2 to 2.7 for 100, 000 [6, 7]. There is no population based published data about the incidence or prevalence of pediatric stroke in India. In the hospital based studies from India, pediatric stroke have constituted less than 1 percent of all pediatric admissions and 5 to 10 percent of all strokes in young (<40 years) [8, 9]. Eighty percent of adult strokes are due to ischemia. While ischemic strokes in adults are usually thrombotic or embolic in nature, they may also be caused by hypo perfusion states. Cryptogenic strokes comprise 30 to 40% of all adult ischemic strokes and approximately 50% in children [10, 11]. Acute ischemic strokes in children most commonly occur between the ages of 1-5 years and least common in the < 1 year and > 15 years [12]. Focal neurological signs occur in three quarters of patients; with hemiplegia is the most common [12]. Despite the fact that infection accounts for 26% of cases, fever is present only 11% of the time [12]. The risk factors for stroke in children are congenital heart disease, infection, prothrombotic disorders, trauma, acquired, congenital vascular disease, sickle cell disease, metabolic disorders, and mitochondrial disease. Vascular disease alone accounts for one-third of cases, while metabolic disorders and prothrombotic disorders comprise 18% and 13% of cases respectively [12]. Trauma makes up an additional 11% of cases [12]. At least one risk factor is present in 90% of patients with almost 25% of patients having more than one [12]. There appears to be demographic variation with a predilection for both gender and ethnicity. A seasonal variation may exist, as the disease most commonly occurs during the summer and least commonly during the winter. [12]. Males carry a significantly higher risk of suffering all stroke subtypes compared to females [13]. ED management of a child suffering from an ischemic stroke should focus on stabilization. Stabilization begins with securing the airway, providing supplemental oxygen, establishing IV access, monitoring vital signs and mental status. An emergency CT of the head in the ED should not be delayed. An ECG, CXR and lab work should be sent, including a complete blood count, blood and CSF cultures, chemistry, liver enzymes, cardiac markers, coagulation factors, urine analysis and urine drug screen. Empiric intravenous antibiotics and antivirals, maintenance fluid with an isotonic, non-dextrose containing fluid must be initiated in the ED. Anti-platelet drugs are widely used in adults literature has shown they reduce the rate of strokes [10]. Although randomized controlled trials with children have not been conducted, anti-platelet drugs are used in some centers to reduce the recurrence rate of stroke [10]. Adverse effects, such as severe bleeding or the precipitation of Reye’s syndrome, are rare. The use of anti-thrombotic drugs remains controversial in the pediatrics and is not the standard of care [10]. However, anti-thrombotic drugs are being given to pediatric patients at some institutions despite a paucity of supporting literature [2]. The benefits are unclear, and it seems their use is based on adult studies, case reports and expert opinion. One study showed 1.6% of pediatric AIS patients admitted between 2000 and 2003 received thrombolytic therapy [14]. The children receiving thrombolytics had significantly higher medical costs, were less likely to be discharged home and had higher overall mortality rates [1]. Shortcomings of these findings were noted, including the small sample size and unknown severity of any of the patients at the time of presentation [1]. Conversely, several case reports have been published showing potential benefits using thrombolytic therapy in children, including success stories across a wide age range and administration of thrombolytics well outside of the standard three-hour window used in adults [14, 15]. There are numerous etiologies for acute ischemic stroke in the pediatric population. Arterial dissection is one important cause. While most dissections occur in the internal carotid artery, children may dissect intracranially. MRI and contrast MRA show the anatomy without the risks of traditional angiography or radiation. Duplex ultrasonography is useful, but CT angiogram still remains the gold standard for further investigation for suspected arterial dissection [16]. Secondly, cerebral venous sinus thrombosis may cause strokes in children. This commonly develops from extension of infections, including acute otitis media, mastoiditis, pharyngitis, sinusitis, or meningitis. If infection is suspected, appropriate intravenous third generation cephalosporins, vancomycin and acyclovir should be initiated. Additionally, infectious vasculitis may occur from chronic infections such as tuberculous meningitis, rickettesial, varicella, and coxsackie infection. Lastly, cerebral vasculitis should be considered in children with either ischemic or hemorrhagic stroke, as well as strokes associated with fever or rash. While erythrocyte sedimentation rate may be used as a screening tool, its interpretation should be used with caution since it does not exclude all vascular etiologies for ischemic stroke [16]. There is no literature to support the empiric use of steroids; however, they may be given to treat cerebral edema or a vasculitic cause of stroke. The rate of recurrence for childhood stroke may be as high as 30% and is dependent upon the etiology of the stroke. 2 Children with a hypercoagulable disorder or a vascular diagnosis have a higher likelihood of recurrent stroke [10]. Sickle cell disease patients have a 40% chance of repeat stroke, while children with arterial dissection have a recurrence rate of 12% [16]. Children who suffer AIS generally recover better than adults, but the effects may still be long lasting and detrimental. While children who suffer a stroke have good educational and mobility outcomes, they have poorer outcomes when it comes to communication, socialization and activities of daily living [17]. Social and economic consequences, including decreased ability to work and lifelong disability, may arise. This is even more profound in children having a recurrence [17].
Conclusion
AIS in the pediatric patient are a rare but potentially devastating disease. The lack of research in this area is apparent. The sudden onset of focal neurological deficit in children is stroke until proven otherwise. Due to the high rate of recurrence, anti-platelet drugs should be considered and initiated in the ED. Acute stroke is an emergency, however delay in recognition is common and delayed diagnosis and treatment outcome is poor.
References
-
Janjua N, Nasar A, Lynch JK, Qureshi AI (2007) Thrombolysis for ischemic stroke in children: data from the nationwide inpatient sample. Stroke 38(6): 1850- 1854.
-
The International Stroke Trial (IST) (1997) A randomized trial of aspirin, subcutaneous heparin, both, or neither among 19435 patients with acute ischaemic stroke. International Stroke Trial Collaborative Group. Lancet 349(9065): 1569-1581.
-
National Institute of Neurological Disorders and Stroke rtPA Stroke Study Group (1995) Tissue plasminogen activator for acute ischemic stroke. N Engl J Med 333: 1581-1587.
-
Hacke W, Kaste M, Fieschi C, Toni D, Lesaffre E, et al. (1995) Intravenous thrombolysis with recombinant tissue plasminogen activator for acute hemispheric stroke. The European cooperative acute stroke study. JAMA 274(13): 1017-1025.
-
Multicentre Acute Stroke Trial—Italy (MAST-I) Group (1995) Randomised controlled trial of streptokinase, aspirin, and combination of both in treatment of acute ischaemic stroke. Lancet 346(8989): 1509-1514.
-
Broderick J, Talbot GT, Prenger E, Leach A, Brott T (1993) Stroke in children within a major metropolitan area: The surprising importance of intracerebral hemorrhage. J Child Neurol 8(3): 250- 255.
-
Roach ES (1993) Cerebrovascular disorders and trauma in children. Curr Opin Pediatr 5(6): 660-668.
-
Nagaraja D, Verma A, Taly AB, Veerendra Kumar M, Jayakumar PN (1994) Cerebrovascular disease in children. Acta Neurol Scand 90(4): 251-255.
-
Mehndiratta MM, Aggarwal P, Gupta M, Puri V, Aggarwal S (1998) Stroke in 127 young people. Proceedings of the Lancet Stroke Conference, Montreal.
-
Nowak-Gottl, Sträeter R, Sébire G, Kirkham F (2003) Antithrombotic drug treatment of pediatric patients with ischemic stroke. Pediatric Drugs 5(3): 167-175.
-
Lee BI, Nam HS, Heo JH, Kim DI, Yonsei Stroke Team (2001) Yonsei Stroke Registry. Analysis of 1,000 patients with acute cerebral infarctions. Cerebrovasc Dis 12(3): 145-151.
-
Lee Y, Lin KL, Wang HS, Chou ML, Hung PC, et al. (2008) Risk factors and outcomes of childhood ischemic stroke in taiwan. Brain and Development 30(1): 14-19.
-
Fullerton HJ, Wu YW, Zhao S, Johnston SC (2003) Risk of stroke in children: ethnic and gender disparities. Neurology 61(2): 189-194.
-
Carpenter J, Tsuchida T, Lynch JK (2007) Treatment of arterial ischemic stroke in children. Expert Review of Neurotherapeutics 7(4): 383-392.
-
Shuayto MI, Lopez JI, Greiner F (2006) Administration of intravenous tissue plasminogen activator in a pediatric patient with acute ischemic stroke. Journal of Child Neurology 21(7): 604-606.
-
Roach SE, Golomb MR, Adams R, Biller J, Daniels S, et al. (2008) Management of Stroke in Infants and Children: A Scientific Statement from a Special Writing Group of the American Heart Association Stroke Council and the Council on Cardiovascular Disease in the Young. Stroke 39(9): 2644-2691.
-
Hurvitz E, Warschausky S, Berg M, Tsai S (2004) Long-term functional outcome of pediatric stroke survivors. Topics in Stroke Rehabilitation 11(2): 51- 59.
-
Williams GR (2001) Incidence and Characteristics of total stroke in the United States. BMC Neurol 1: 2.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey