Mental Health of Refugees from Syria, Afghanistan in Collective Centers in Macedonia, 2016
<p>Introduction: The examination was conducted in order to evaluate the mental health of the refugees coming to Macedonia from Syria, Afghanistan in 2016.</p> <p>Material and Methods: The mental health assessment was done with interviews and Child & Youth Mental Health General Questionnaire, for the children and the adolescents, and with interviews and Mental Health General Questionnaire, for the adults. All questionnaires were administered to 70 refugees, with a goal to determine risks factors, appeared mental disorders and to develop special psychosocial programs according their needs.</p> <p>Results: The results showed high percentage of generalized anxiety, separation anxiety, depression, aggression, behavioral problems.</p> <p>Conclusion: These findings confirm that general mental health in adults and especially in children and adolescents is attacked by the survived trauma, parents feelings, unstructured day activities, and mostly by the feeling of uncertain future.</p>
Introduction
Refugees have high risk factors for mental disorders. It is undoubtedly that most of the refugees arriving in Macedonia, in 2016, experienced traumatic events, persecution, and violence, loss of identity and culture, and often loss of a family member. Such experiences have a direct impact on the symptoms of psychological disorders on individual, family and group level. On the other hand, the difficulties they face in their everyday life additionally contribute to the disturbance of the psychological state [1, 2].
Estimates of the post-traumatic stress disorder-PTSD in adult refugees in various researches carried out so far in the world ranged from 3% to 86% of the refugees, and for depression the ranging is from 3% to 80% of the refugees [3, 4, 5]. Accepting only the lowest rates as valid is a step towards neglecting the refugee's mental health, and the reverse, accepting always the upper end of the expected prevalence of psychiatric disorders leads to the stigmatization of refugees as a population with very high psychiatric morbidities. Heterogeneity persists even in the findings of larger studies. Serious meta-analysis suggests that about 1 out of 10 adult refugees in Western countries have PTSD, 1 out of 20 has a major depression, and about 1 in 25 have a generalized anxiety disorder, with likelihood that these disorders often overlap. PTSD and depression, or their symptoms, are primarily associated with surviving traumas, stressful events during displacement, but psychological symptoms increase further by uncertainty and unresolved status. Aggression and behavioral problems that are often seen in refugees are indicative for the mental health concerns and they negatively affect their social functioning. The somatisation is often resented by: headache, abdominal pain, stomach problems, myalgia, and so on. These symptoms are actually a significant component of the symptomatology that points to psychological problems. Disturbances such as insomnia, hypersomnia, anorexia refer to psychological suffering also [6, 7, 8, 9]. Without a doubt, special attention should be paid to the mental health of refugee children and adolescents who are the most vulnerable group because their overall mental development is significantly affected. It is important to emphasize that traumatic experience for refugee children and adolescents have acute-immediate, but also long-lasting consequences on their mental health. Many recent studies suggest that the most common problem is PTSD followed by depression, behavioral disorders and emotional disorders are common, including aggression and affective disorders. The presence of such disorders in conditions such as a refugee camps without a supportive and nursing environment, especially with the absence of their parents (killed, missing) additionally and significantly increases the danger of serious mental health consequences throughout their lives. PTSD and depression are the most frequently observed mental health problem in refugee children and adolescents, and it disrupts everyday interactions with their families, friends and peers. Over 25% of refugee children show signs of PTSD, 44% of refugee children reporting symptoms of depression. It is also important that female ratio is 54% and male ratio is 26% that have symptoms of depression. Undoubtedly, girls are at a much greater risk of depression. Large percentage of refugee children is with psychosomatic symptoms (pain in different parts of the body), 25% of refugee children have body pain, and 15% of children have psychosomatic pains). In the context of the cultural norms of emotional expression and manifestation of psychological stress, somatisation is an important component in refugee children and adolescents lives. Problems with attention, hyperactivity, aggression and social retreat in formal groups are also noticed in refugee children and adolescents [3, 4, 6, 10, 11].
Method and Materials
In this study an assessment was made in order to evaluate the mental health of the refugees coming to Macedonia from Syria, Afghanistan in 2016, in the two refugee camps in Macedonia (Vinojug Gevgelija and Tabanovci, Kumanovo). A specially structured questionnaire for self- assessment by refugees for psychological condition was used. Mental Health General Questionnaire was used for adult refugees, and Child & Youth Mental Health General Questionnaire Recommendations was used for refugee children. The questionnaires were filled by 1/3 of the refugees in both camps. The basic objectives of the examination are to determine: 1) The frequency of psychological-psychiatric disorders in children and adult refugees. 2) Assessment of the need for treatment of these disorders and its specification in the conditions of refugee camps.
Results
There are 81 refugees in the refugee camp in Tabanovtsi-Kumanovo, out of which 40 children under the age of 18 and 40 adults, while in the camp "Vinojug" Gevgelija there are 130 refugees, 60 of them under the age of 18 and 70 adults. The frequency of PTSD among adult refugees in both camps is identical (9%), the mean depression rate is 25% (significantly more significant among the refugees placed in Vinojug-Gevgelija camp), and the mean frequency of anxiety is the highest, represented in 44% (something more pronounced among the refugees in the camp Vinojug-Gevgelija) (Graph 1).
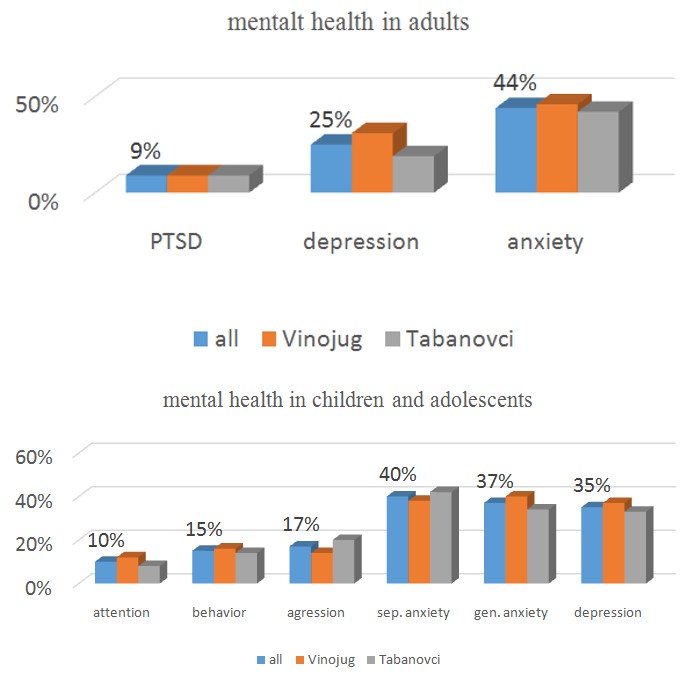
Graph 1: Mental health in adults.
In refugee children, the separation anxiety is most pronounced, which is shown by 40% of children (something more pronounced in children in Tabanovce). Generalized anxiety is present in 37% of children (more pronounced in children in Vinojug). Depression is present in 35% of children (more pronounced with children in Vinojug). Aggression is present in 17% (more emphasized in children in Tabanovci), behavioral problems in 15%, and disturbance in 10% (more emphasized in children in Vinojug) (Graph 2).
Graph 2: Mental health in children and adolescents.
Discussion
Refugees who are faced with displacement, abandonment of their home, immediate and wider surrounding and their way of life have suffered separation from their wider families, some of them also from their primary family, and were initially primarily targeted to basic survival, such as providing food, water and shelter. In other words, they were faced with primary fears of survival and security for themselves and their loved ones. After their placement in a safe environment (collective centers), their primary concern is directed to the uncertainty, associated with their future. They are currently experiencing anxiety, fear, helplessness, depression, a sense of loss of control, apathy, fatigue, grief, isolation, etc. In the context of this, it is necessary that the focus of care for them have to be put on their mental health. Certainly surviving trauma during displacement is an initial trigger for mental health disorder, but current worries and uncertainty about the future and the lack of everyday constructive activities further aggravate their mental health [12, 13].
The higher prevalence of depression and anxiety among refugees in Macedonia despite the representation of PTSD points to a more pronounced impact on the current situation in which they are affected by the impact of the traumas of wars in their countries and transport to Macedonia. Namely, the long-term stay in these camps causes a very pronounced level of anxiety and depression following the great uncertainty about the realization of their emigration plan in the desired destinations in Western countries. Adult refugees from Vinojug-Gevgelija collective center are more depressed and anxious due to the pronounced restriction in the possibility of leaving the camp and their awareness of the physical distance from the boundary leading them to the desired destination. On the other hand, among the refugees in the camp Tabanovci-Kumanovo there is more hope and more expectations for faster departure from the collective center and leaving to the desired destination, which is happening occasionally with some of the refugees.
Children and adolescent refugees from Vinojug-Gevgelija collective center have more generalized anxiety and depression that lead in a more serious disorder of their attention and behavior. The reason for this is probably the transmission of high anxiety and depression from their parents with the phenomenon of psychological induction. Namely, children and adolescent tend to directly take negative emotional experiences from their loved ones. On the other hand, the children and adolescent refugees from the camp in Tabanovci-Kumanovo have more pronounced separation anxiety and aggressiveness, which is probably due to the more frequent waves in the situation in the camp in terms of new arrival and departure of a part of the refugees.
Threats to the psychological health of refugees arising from surviving traumatic experiences and from the current conditions in which they are found could be summarized in:
- High incidence of depression, anxiety, PTSD and fears for the family, especially in those who are separated from loved ones.
- Uncertainty in the future.
- Affordable dependence on the system, lack of autonomy. Constant care and uncertainty for further legal and immigration procedures, especially for those who are not in the asylum procedure.
- The need for your home away from others.
- Any problems that arise due to linguistic and cultural barriers.
- Conflicts in the camp because of ethnic and national differences between refugees.
- Lack of individual or group counseling, psychotherapy.
When it comes to children and adolescents mental health, they also suffer from an aspect about their education. It is very important for them that their parents are involved in their education, because in this way they will have certain constructive activities that are making their bonding stronger, and the children and adolescents will have the experience that they are important, and certain educational activities can be better coordinated with the current educators themselves. It would also positively affect children and adolescents in their school engagements and social adaptation.
For adults, apart from the possibility of learning a language, there are no organized educational and psychosocial activities. Introducing psychosocial activities for adults would be of great importance for the improvement of the overall psychological state. In this context, creating a particular occupational-work therapy for would have a significant positive impact for improving the image for themselves, their sense of satisfaction and reducing frustration. By reducing the annoyance and feeling of loneliness, the symptoms of depression, anxiety, PTSD would also be reduced, and at the same time a feeling of greater security for their new life would be built and would have contributed to building a sense of power, as opposed to insecurity, the powerlessness and the uncertainty that they currently feel. In this way, they are helped to build a new identity, because they are lost, they are helped to socialize in a culture in which they want to continue their lives. The increased sense of autonomy and freedom with the ability to partially live the way they want can reduce regressive dependence and experience is determined by the outside [14, 15, 16, 17].
Conclusion
For refugees who manifest symptoms of PTSD, anxiety and depression, a combined psychiatric-psychological drug and psychotherapy treatment is necessary. Taking into consideration the fact that refugee children and adolescents are the most vulnerable group among refugees, their mental health disorders can leave very significant consequences for the overall psychological development and further psychological functioning, seems that the most urgent need for them is proper psychological-psychiatric treatment. Psychotherapeutic treatment of the children and adolescents is necessary to be carried, but also with their parents or families, as well as with the staff working with them. In this context, additional psychosocial programs for refugee children and adolescents are also necessary for the purposes of: (1) Establishing safety and security (2) Integration into a new cultural context (3) Redefinition of individual identity, including acculturation and acquiring new skills for coping, solving problems and conflicts, new competence skills.
References
-
Abou-Saleh M, Mobayad M (2013) Mental Health in Syria. International Psychiatry 10(3): 58-60.
-
Adams KM, Gardiner LD, Assefi N (2004) Healthcare challenges from the developing world: post- immigration refugee medicine. BMJ 328(7455): 1548- 1552.
-
Al Ammar K (2009/2010) [Post Traumatic Stress Disorder resulting from the war in Iraq: Diagnostic study with a sample of displaced Iraqis.] Unpublished master’s thesis, University of Damascus, Damascus, Syria.
-
Al Obaidi A S, Atallah SF (2009) Iraqi refugees in Egypt: An exploration of their mental health and psychosocial status. Intervention 7(2): 145-151.
-
Carballo M (2011) The Health of Migrants. École-Club Migros, Nyon, Switzerland.
-
Silove D (2004) Mental health problems in migrants and refugees. Australian Doctor 31-38.
-
Weinstein HM, Sarnoff RH, Gladstone E, Lipson JG (2000) Physical and Psychological Health Issues of Resettled Refugees in the United States. Journal of Refugee Studies 13(3): 303-326.
-
Gorst-Unsworth C, Goldenberg E (1998) Psychological sequelae of torture and organized violence suffered by refugees from Iraq: Trauma- related factors compared with social factors of exile. British Journal of Psychiatry 172(1): 90-94.
-
International Medical Corps (IMC) & Jordan Health Aid Society (JHAS) (2012) Displaced Syrians in Jordan: A Mental Health and Psychosocial Information Gathering Exercise. Analysis and Interpretations of Findings. Amman: IMC, JHAS.
-
Berman H (2001) Children and war: Current understandings and future directions. Public Health Nursing 18(4): 243-252.
-
International Medical Corps (IMC) (2011) Psychosocial Assessment of Displaced Syrians at the Lebanese-Syrian Northern Border. Beirut: IMC.
-
El-Shaarawi N (2012) Living an Uncertain Future: An Ethnography of Displacement, Health, Psychosocial Well-being and the Search for Durable Solutions among Iraqi Refugees in Egypt. Dissertation Abstracts International Section A 73(6-A): 2191.
-
Quosh C (2013) Mental health, forced displacement and recovery: integrated mental health and psychosocial support for urban refugees in Syria. Intervention 11(3): 295-320.
-
Arnetz J, Rofa Y, Arnetz B, Ventimiglia M, Jamil H (2013) Resilience as a Protective Factor Against the Development of Psychopathology Among Refugees. Journal of Nervous and Mental Disease 201(3): 167- 172.
-
Birman D, Trickett EJ (2001) The process of acculturation in first generation Immigrants: A study of Soviet Jewish Refugee Adolescents and Parents. Journal of Cross-Cultural Psychology 32: 456-477.
-
Hárdi L, Kroó A (2011) Psychotherapy and psychosocial care of torture survivor refugees in Hungary. Torture 21(2): 84-97.
-
Quosh C (2011) Takamol: Multi-professional capacity building in order to strengthen the psychosocial and mental health sector in response to refugee crises in Syria. Intervention 9(3): 249-264.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey