Choledocal Cyst as a Cause of Abdominal Pain Clinic Case: Choledocal Cyst
A 37-year-old female patient with abdominal pain in the right hypochondrium of chronic evolution, history of mild acute pancreatitis 3 months ago. Normal laboratory tests except for slight elevation of bilirubins; Radiological and endoscopic studies (ultrasound, abdominal tomography, colangioresonance, endoscopic retrograde cholangiopancreatography) report dilation of the main bile duct compatible with choledochal cyst. She underwent laparotomy finding a gallbladder, fibrous wall, cystic duct of 10 cm in length, with several bends, cystic tumor involving common hepatic duct, distal two thirds of the cystic duct and common bile duct to her retropancreatic portion with duct diameter of 5 cm. cm. En bloc resection including gallbladder, cystic duct, common hepatic duct and common bile duct; finally bilioenteric anastomosis in Y of Roux. It evolves satisfactorily; the histopathological report fibrous cystic wall coated by reactive superficial epithelium, focus of pseudopilórica metaplasia and chronic inflammatory infiltration.
Introduction
The choledochal cyst (QC) is a rare pathology in our environment. It is more frequent in Asia, especially in Japan, and predominates in the female sex. It is usually diagnosed in childhood, 80% of cases before 10 years. The etiology is unknown and several hypotheses have been postulated, among which are the anomalies in the biliopancreatic junction, which are frequently associated with biliary cysts [1].
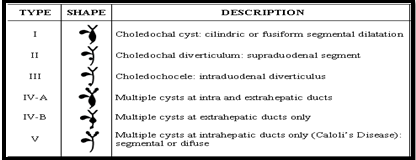
They are divided into 6 types according to the Alonso- Lej classification established in 1954 and modified by Todani in 1977 (Figure 1) [1]. Type I, the most frequent (80-90% of all QC), is a segmental or fusiform dilatation of the common bile duct. Type II or diverticulum in the cystic and type III or choledochocele are the rarest (2%) [2]. Type IV is the second in frequency (10-15%). It is characterized by multiple cystic dilatations of the intra and extrahepatic bile duct (IVa) or only of the extra hepatic bile duct (IVb) [3]. Type V or Caroli's disease is a diffuse cystic involvement of the intrahepatic bile duct.
Clinical Case
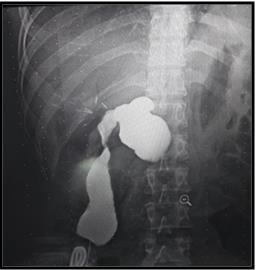
Female patient of 37 years of age, married, indigenous, born and resident in Gatazo Province of Chimborazo in Ecuador [4]. She went to the surgery department because she had mild abdominal pain that was located in the right hypochondrium of a long time. The diagnosis of acute pancreatitis 3 months ago is the only antecedent. Complementary imaging studies were performed, reporting the abdominal ecosonogram of bile duct dilatation, cystic lesion of the head of the pancreas versus choledochal cyst (Figure 2), simple and contrasted computed tomography of the abdomen: common bile duct (Figure 3), colangioresonance Nuclear magnetic field reports 11-mm common bile duct, retropancreatic level shows a 4.5 cm diameter saccular diverticulum in relation to common bile duct (all type III), plus signs suggestive of residual pancreatitis.



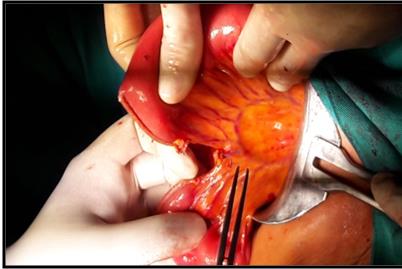
Figure 4: Dilatation of the biliary tree with gallbladder in situ alitiásic. In complementary laboratory tests there is no alteration in the leukocyte formula; however, there is a slight increase in bilirubins due to direct Bilirubin. Physical examination highlights an anicteric patient, painful abdominal level to deep palpation in the right hypochondrium. She underwent laparotomy finding a gallbladder, fibrous wall, cystic duct of 10 cm in length, with several bends, cystic tumor involving common hepatic duct, two distal thirds of the cystic duct and common bile duct to her retropancreatic portion of ducts diameter. cm. En bloc resection involving the gallbladder, cystic duct, common hepatic duct and common bile duct to the retropancreatic portion is performed (Figure 5); finally bilioenteric anastomosis in Roux-en-Y (Figure 6).
Discussion
We can assure that ultrasound is a very important auxiliary method for the diagnosis of type I choledochal cyst. However, one of its limitations is that it depends, to a large extent, on the experience of the radiologist [4]. For this reason, and in the face of the diagnostic doubt, two imaging studies were also evaluated: contrast-enhanced CT of the abdomen and colangioresonance, since they are more sensitive and specific than ultrasound and do not depend so much on the ability of the personnel performing the examination [5]. Study to arrive at an accurate diagnosis. When comparing colangioresonance with tomography, it was found that the first one helps to determine that there is adequate hepatic and biliary functionality, has a sensitivity of 100%, its cost is lower, it is a quick and simple procedure that does not require any special preparation and the risk of presenting side effects to the study is very low. The tomography is very useful to make the diagnosis since it assesses the intra and extrahepatic bile duct, the adjacent structures and the presence and stage of associated malignant tumors [6, 7]. However, one of the disadvantages is the presentation of adverse effects to the contrast medium; another, exposure to radiation. The surgical approach that includes the complete excision of the cyst with reconstruction by means of a bilioenteric anastomosis in Roux-en-Y is the treatment of choice for most types of choledochal cysts [8]. However, if the cyst is large and its complete excision is not possible, a resection of the anterior wall is performed and the mucosactomy is performed to the posterior wall to avoid carcinogenesis. Exceptions to this practice include type III and V approaches. Types I, II, and IV are biliary excision and reconstruction [9]. The choledochocele (type ID) has been treated with transduodenal sphincteroplasty or endoscopic papillotomy. Type V cyst or Caroli's disease can be addressed in three ways: 1. If the intrahepatic cyst has large dimensions, it is drained at a first surgical time, it is expected to decrease and then it is resected.
2. Resection of the cyst with a hepatojejunoanastomosis in Roux-en-Y.
3. If the dilation is very large and the liver presents a significant injury, a liver transplant is performed [10, 11, 12].
Conclusions
The choledochal cysts are a rare entity and have a very varied clinical presentation, which requires a high index of suspicion to avoid delays in diagnosis and complications. The imaging method that should be used is colangioresonance, which allows adequate characterization and facilitates surgical planning. Complete resection of the cyst and cholecystectomy should be performed using an open or laparoscopic technique, as this reduces the risk of complications and malignant degeneration.
References
-
Vaquero Sosa E, Bodas Pinedo A, Llanos D, Soto C, Rivilla F, et al. (2013) Quiste de colédoco como causa de dolor epigástrico. Anales de Pediatría 78: 191-192.
-
Sugiyama M, Haradome H, Takahara T, Izumisato Y, Abe N, et al. (2004) Biliopancreatic reflux via anomalous pancreaticobiliary junction. Surgery 135(4): 457-459.
-
Soares KC, Arnaoutakis DJ, Kamel I, Rastegar N, Anders R, et al. (2014) Choledochal cysts: presentation, Clinical differentiation, and management. Journal of the American College of Surgeons 219(6): 1167-1180.
-
Hill R, Parsons C, Farrant P, Sellars M, Davenport M (2011) Intrahepatic duct dilatation in type 4 choledochal malformation: pressure related, postoperative resolution. J Pediatric Surg 46(2): 299- 303.
-
Ziegler KM, Zyromski NJ (2011) Choledochoceles: are they choledochal cysts?. Adv Surg 45: 211-224.
-
Dong JH, Yang SZ, Xia HT, Duan WD, Ji WB, et al. (2013) Aggressive hepatectomy for the curative treatment of bilobar involvement of type IV-A bile duct cyst. Ann Surg 258(1): 122-128.
-
Pal K, Singh VP, Mitra DK (2009) Partial hepatectomy and total cyst excision is curative for localized type IV-a biliary duct cysts-report of four cases and review of management. Eur J Pediatric Surg 19(3): 148-152.
-
Gong L, Qu Q, Xiang X, Wang J (2012) Clinical analysis of 221 cases of adult choledochal cysts. Am Surg 78(4): 414-418.
-
Yamaguchi M (1980) Congenital choledochal cyst, analysis of 1,433 patients in Japanese literature. Am J Surg 140(5): 653-657.
-
Todani T, Tabuchi K, Watanabe Y, Kobayashi T (1979) Carcinoma arising in the wall of congenital bile duct cyst. Cancer 44(3): 1134-1141.
-
Arroyo Martínez Laura, Montero Carvajal Royner, Ayi Wong José (2004) Quiste del colédoco como causa de dolor abdominal: revisión de un caso y bibliografía. Acta Méd Costarric 46(3): 149-151.
-
Ziegler KM, Pitt HA, Zyromski NJ, Chauhan A, Sherman S, et al. (2010) Choledochoceles: are they choledochal cysts?. Ann Surg 252(4): 683-690.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey