Prophylaxis for Occupational HIV Exposure in Healthcare Workers
<p style="text-align: justify;">Human Immunodeficiency virus (HIV) infection is one of the world’s most serious health hazards with a great impact on society. Health care workers are at a significant risk from occupational exposure to HIV due to their constant contact with potentially infectious body fluids from HIV patients mainly via percutaneous blood exposure. Hence, every health care worker including medical and dental professionals, nurses, laboratory personnel etc. should have utmost care and precise knowledge regarding the preventive measures, pre and post exposure prophylaxis on accidental exposure and use of anti retroviral therapy. The present review informs us about the current risk of healthcare workers, making them aware of the precautions and prophylaxis available in case of occupational HIV exposure.</p>
Introduction
Human Immunodeficiency Virus (HIV), the virus that causes Acquired Immuno Deficiency Syndrome (AIDS) is one of the world’s most serious health and development challenges. According to UNAIDS (United Nations Programme on HIV and AIDS), there was approximately 36.7 million people worldwide living with HIV/AIDS at the end of 2016. Of these, 1.8 million were children (<15
years). Because of risky behaviors, heterosexuality, development of civilization and declining boundaries between people, a chance of HIV contagion is a real threat in everyday life [1]. This is particularly true of health care workers. A health care worker can be any person whose activities involve contact with patients or with blood or other body fluids from patient in a health care or laboratory setting. Health care workers (HCWs) are defined as all paid and unpaid persons working in health care settings with the potential for exposure to infectious materials (e.g., blood, tissue, and specific body fluids) or contaminated medical supplies, equipment, or environmental surfaces. HCWs can include but are not limited to physicians, nurses, dental personnel, laboratory personnel, students and trainees, and persons not directly involved in patient care (e.g., housekeeping, security, and volunteer personnel). According to Centre for Disease Control and Prevention (CDC), during 1985–2013, 58 confirmed and 150 possible cases of occupationally acquired HIV infection among HCWs were reported in the United States [2]. Nurses report the most frequent blood and body exposures (48.6 percent), followed by physicians who are residents or fellows (7.7 percent), attending physicians (7.7 percent), non-lab technologists (4.5 percent), respiratory therapists (3.6 percent), and certified nursing assistants/home health aides (3.2 percent) [3].
Need for HIV Prophylaxis for Healthcare workers
When HIV infection advances to AIDS, the body becomes prone to opportunistic infections affecting the whole body system due to weakened immunity [4]. Common infections associated with AIDS are bacterial and fungal infections like tuberculosis, oral candidiasis, cryptococcal meningitis, toxoplasmosis, malignancies like Kaposi’s sarcoma, lymphomas etc. Hence preventive measures like earlier HIV diagnosis and the use of antiretroviral therapy (ART) as pre- and postexposure prophylaxis (PrEP and PEP) need to be administered at the earliest. Both have been shown to be effective in preventing human immunodeficiency virus (HIV) transmission in humans [5].
Transmission and Risk of HIV in Healthcare Workers
HIV is transmitted in human body fluids by three major routes: (1) sexual intercourse through vaginal, rectal, or penile tissues; (2) direct injection with HIV-contaminated drugs, needles, syringes, blood or blood products; and (3) from HIV-infected mother to fetus in utero, through intrapartum inoculation from mother to infant or during breast-feeding. Potentially infectious contacts that may place a health worker at risk are [6]:
- A percutaneous injury (e.g., a needle stick or cut with a sharp object).
- Contact of mucous membrane or nonintact skin (e.g., exposed skin that is chapped, abraded, or afflicted with dermatitis).
- Body fluids of concern include: blood, semen, vaginal secretions, other body fluids contaminated with visible blood.
- Potentially infectious body fluids (undetermined risk for transmitting HIV): cerebrospinal, synovial, pleural, peritoneal, pericardial, and amniotic fluids. In addition, any direct contact (i.e., without barrier protection) to concentrated HIV in a research laboratory or production facility is considered as an "exposure" that requires clinical evaluation. Table 1 provides an estimate of the risk of HIV transmission through different routes. The risk of HIV transmission through body fluids such as urine, sputum, feces, vomits, nasal secretions, sweat, and tears is low or even does not exist if visible blood is not present. Human milk is considered as a potential risk factor for HIV but not for health care workers (except nursing neonate), especially surgeons or anesthesiologists, since the chances of exposure to this body fluid is considerably low or absent. Saliva of HIV patient also does not pose any threat to the daily works of surgeons and anesthetists [5, 7, 8, 9].
| Exposure route | HIV (%) | ||||
|---|---|---|---|---|---|
| Blood transfusion | 90-95 | ||||
| Perinatal | 20-40 | ||||
| Sexual intercourse | 0.1-10 | ||||
| Vaginal | 0.05-0.1 | ||||
| Anal | 0.065-0.5 | ||||
| Oral | 0.005-0.01 | ||||
| Injecting drugs | 0.67 | ||||
| Needle stick exposure | 0.3 | ||||
| Mucous membrane splash to eye, oro-nasal | 0.09 |
Table 1: Risk percentage of HIV transmission through different routes [10]. (Adapted from Post Exposure Prophylaxis (PEP) – NACO
The risk of transmission of HIV infection following inadvertent exposure is increased when the source has a high viral load, the volume is large, and the exposure is deep. It was estimated that the average risk for HIV transmission after a percutaneous exposure to HIV infected blood is approximately 0.3% and after a mucous membrane exposure is 0.09% but there can be variation depending on the inoculum size, the depth of penetration, and exposure to a hollow bore versus suture needle [11, 12]. Also, long work hours and sleep deprivation among medical trainees result in fatigue, which is associated with a threefold increase in the risk of needle-stick injuries [13].
It was found that approximately 62.7% of needle stick and sharps injury occurred in the first 6 months of postgraduate education. The most vulnerable groups of residents being dental, obstetrics and gynecology, and surgery residents, where exposure to needlestick or sharps injury was 30.6%, 28.9%, and 18.5%, respectively.
Every patient is not treated as a potential HIV positive. Only when the patient is from the risk group (male homosexuals and bisexuals, intravenous drug abusers, hemophiliacs, and the child of parents who are HIV positive), precautions are started. According to a study done by Kelen, et al., it was observed that lying on clinical suspicions is insufficient to recognize patients from these groups and that the surgeons who are relying on clinical suspicion will be underestimating the numbers of their patients at risk [14, 15].
Many healthcare professionals think that HIV testing should be performed before invasive procedures like surgeries. Also, a negative HIV test in a patient at risk group could reduce vigilance and care of health care workers by the conviction that there is no risk in such patients, who still exhibit high-risk behavior and who in the recent past could have become HIV positive or is in the serological window [5].
**Prevention of Infection**
The Center for Disease Control and Prevention from Atlanta presents some general precautions, to prevent transmission of HIV and other blood borne pathogens among medical staff [16]. The general precautions are as follows:
- Washing hands before and after examining a patient; to immediately wash the other parts of the body, if they have been soiled with any body fluid from the patient.
- Using disposable gloves during every examination of the patient. Wearing double gloves during surgery reduces contamination of the skin by blood, tissue, and other fluids from the patient to the entire surgical team, especially the surgeon though it is not a general rule.
- Use of a thimble or other protective shield over the distal left index finger (for right-handed surgeons) to avoid needle stick injury during suturing since it is the most often penetrated site. Tying of sutures in tissues after cutting needles and use of staples for bowel anastomosis and skin closure can also reduce the risk of needle stick injuries [17].
- Wearing protective eyewear reduces chance of contamination of the conjunctiva with blood during surgical procedure.
- Using impervious gowns and wearing protective footwear.
- Use of cautery or hand diathermy instead of a scalpel to perform incision in the operating field.
- Avoiding hand-to-hand passage of sharps, particularly scalpels by means of using a kidney dish.
Pre Exposure Prophylaxis (PrEP)
Pre-exposure prophylaxis or PrEP is the use of antiretroviral medications to prevent the acquisition of HIV infection by uninfected persons to reduce their risk of acquiring HIV. The New York State Department of Health AIDS Institute (NYSDOH AI) in 1991 and the Centers for Disease Control and Prevention (CDC) recommended a combination of antiretroviral agents for pre-exposure prophylaxis (PrEP) as an evidence-based intervention to prevent HIV transmission [18, 19].
In July 2012, the Food and Drug Administration (FDA) approved the use of Truvuda [a fixed dose combination of Tenofovir Disoproxil Fumarate (TDF) and Emtricitabine (FTC)] for HIV PrEP in adults who are at high risk for becoming HIV-infected. It is approved for daily use to prevent an HIV-negative person from getting HIV from a sexual or injection-drug-using partner who’s positive. This regimen consists of one pill taken once per day; when taken consistently, it has demonstrated a high level of protection against HIV infection. If one’s risk of getting HIV infection becomes low because of changes in lifestyle, termination of medication can be considered. PrEP is generally safe and well tolerated. Most people on PrEP report with no side effects, but some side effects were reported in clinical trials primarily nausea, headache, weight loss, mild increase in serum creatinine.
**Post-Exposure Management**
The management of healthcare personnel (HCP) immediately after a significant exposure to blood or body fluids from HIV-infected patients is critically important in reducing the likelihood of transmission and in insuring that the legal rights of the employee and the institution are upheld.
All institutions should have a readily available policy for managing serious exposures. The policy should be distributed to all employees and should be readily available in the Employee Health Service and the Emergency Department.
**Rationale for PEP**
Rationale for PEP include the pathogenesis of HIV infection, mainly
(i) The time course of early infection,
(ii) The biologic plausibility that infection can be prevented or reduced with the use of ART and direct or indirect evidence of the efficacy of specific agents used for prophylaxis;
(iii) The risk/benefit of PEP to exposed HCWs [6].
It may take up to 72 hours for HIV to be detected in regional lymph nodes, up to 5 days to be detected in blood, and about 8 days to be detected in the cerebrospinal fluid which can prevent acquisition of HIV infection after exposure by inhibiting viral replication or preventing dissemination of infection, if ART is started early [20, 21, 22, 23].
**PEP Effectiveness**
Various factors that influence PEP effectiveness include:
Time to start PEP: PEP is likely to be ineffective if initiated more than 72 hours after exposure [24].
Incomplete adherence/ noncompletion: Adherence and completion rates of 4 weeks of PEP among health care workers and individuals exposed nonoccupationally are often poor, which may impact upon its efficacy. Other factors which may decrease the effectiveness are psychological distress and reevaluation of risk [24, 25, 26, 27, 28, 29].
Source virus: Efficacy may be compromised if the source has a virus resistant to one of the agents used. The prevalence of antiretroviral resistance among those with primary HIV infection and those chronically infected with HIV has plateaued at 8% in the UK and Europe unlike the case in low and middle income countries [30, 31, 32].
Penetration of drugs into tissue compartments: Even with optimal viral suppression in the blood, HIV can be detected in other tissue compartments [33].
As different antiretroviral agents penetrate these compartments to different degrees, the choice of drugs could influence its efficacy [34].
- Further high risk sexual exposures.
- Combination therapy with HIV protease inhibitors is considered as highly effective ART. Results from animal studies regarding the efficacy of PreEP and PEP showed that there was suppression of viremia or delayed antigenemia, drug facilitated vaccine-type response (i.e., chemoprophylaxis sufficiently inhibited viral replication to permit formation of a long lasting, protective cellular immune response) and definitive prevention of infection (i.e., chemoprophylactic efficacy) [24].
**Initial actions following exposure**
The initial response to any exposure of HCP to blood should be as follows2:
Immediate Cleansing of the Exposed Site:
i. For skin exposures, the area should be washed with soap and water. Small wounds and punctures may be cleansed with an antiseptic such as an alcohol-based hand hygiene agent, since alcohol is virucidal to HIV, hepatitis B virus (HBV), and hepatitis C virus (HCV). Other antiseptics such as iodophors, chloroxylenol (PCMX) and chlorhexidine (CHG) also inactivate HIV [35].
ii. For mucosal surface exposure, the exposed mucus membranes should be flushed with copious amounts of water. Eyes should be irrigated with saline or water.
Documentation of the Exposure: Clinical information on the source patient for the exposure and the recipient HCP (health care personnel) should be documented. This includes risk factors and serologic tests for HIV, and hepatitis B and C.
Any direct contact (i.e., without barrier protection) to concentrated HIV in a research laboratory or production facility is also considered as exposure that requires clinical evaluation and consideration of PEP.
Note: Intact skin is an effective barrier against HIV infection, and contamination of intact skin with blood or potentially contaminated fluids is not considered an exposure and does not require PEP.
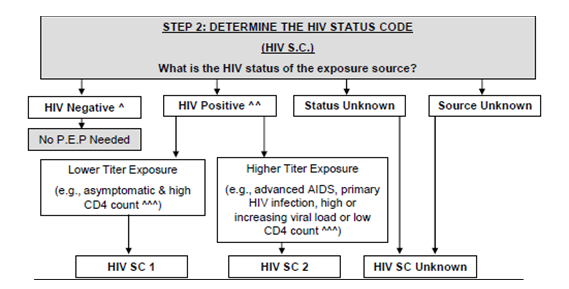
Determining HIV Status of the Source: If unknown, the presence of HIV infection in the source patient should be determined with a rapid HIV test [36]. If testing in the source patient is delayed, PEP should still be initiated while awaiting test results. If the source is found to be HIV-negative, PEP should be discontinued. The CDC recommends routine HIV testing for persons 13 to 64 years of age.
Counseling of Healthcare Worker: Risk assessment is particularly important for HCW to make educated decisions about PEP since the consequences are great and the stress is extraordinary. They should also be well informed of the benefits and risks of PEP and of the importance of close follow-up. • Updated guidelines from the United States Public Health Service (USPHS) and New York State Department of Health AIDS Institute recommend that, after any occupational exposure to HIV, healthcare personnel should immediately receive a post exposure prophylaxis (PEP) of a three drug Regimen [37, 38]. PEP should be initiated as soon as possible, ideally The selection of a drug regimen for HIV PEP must strive to balance the risk for infection against the potential toxicity of the agent(s) used. Because PEP is potentially toxic, its use is not justified for exposures that pose a negligible risk for transmission (Figure 1). Also, there is insufficient evidence to recommend a highly active regimen for all HIV exposures. Therefore, two regimens for PEP are provided (Table 2): a "basic" two drug regimen for most HIV exposures and an "expanded" three drug regimen for exposures that pose an increased risk for transmission or where resistance to one or more antiretroviral agents is known or suspected.
within 2 hours of exposure; A first dose of PEP should be offered to the exposed worker while the evaluation is underway. A PEP supply for 35 days is available for urgent use, and the exposed worker obtains a continuous supply to complete the 28day course. • Follow-up appointments should begin within 72 hours of HIV exposure.
- It should include follow-up HIV testing, monitoring for drug toxicity, and counseling.
- Repeat HIV testing should be obtained at 4 and 12 weeks post exposure.
Recommendations for the selection of drugs for PEP
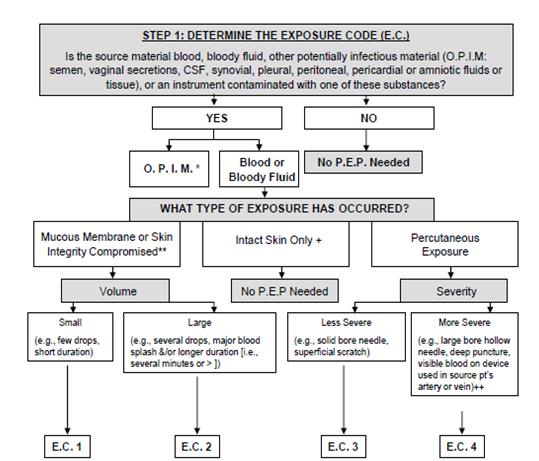
blood), the risk for HIB transmission should be considered. ++The combination of these severity factors (e.g., large bore hollow needle and deep puncture) contribute to an elevated risk for transmission if the source person is HIB positive.
| Step 3: Determine P.E.P. Recommendation | ||||||||
| EC | HIV SC | P.E.P. Recommendation: |
P.E.P. Recommendation: Exposure type does not pose a known risk for HIV transmission. Whether the risk for drug toxicity outweighs the benefit of PEP should be decided by the exposed employee & the treating clinician Consider Basic Regimen: Exposure type poses a negligible risk for HIV transmission. A high HIV titer in the source may justify consideration of PEP. Whether the risk for drug toxicity outweighs the benefits of PEP should be decided by the exposed employee & the treating clinician.
2 1 Recommend basic regimen: Most HIV exposures are in this category; no increased risk for HIV
2 2 Recommend expanded regimen: Exposure type represents as increased HIV transmission risk.
3 1 or 2 Recommend expanded regimen: Exposure type represents an increased HIV transmission risk.
Unknown If the source or. In the case of an unknown source the setting where the exposure occurred, suggests a possible risk for HIV exposure and the E.c. is 2 or 3. Consider P.E.P. basic regimen.
Basic Regimen: 4 weeks Truvada (Tenovir & Emtricitabine) 1 po daily. Truvada is better tolerated than Combivir, it is 1st choiceunless known renal disease. Alternative is Combivir (Zidovudine (AZT) 300mg) and ( Lamivudine (Epivir) 150mg) 1 po BID. Expanded Regimen: Basic regimen PLUS, Kaletra 200/50 (Lopinavir 200 mg and Ritinavir 50 mg) 2 tablets po BID. Figure 1: Determining the need for HIV post exposure prophylaxis (PEP) after an occupational exposure7 (Adapted from MMWR (Morbidity and mortality weekly report) Recommendations and reports Public Health Service Guidelines for the management of health care worker exposures to HIV and recommendations for post exposure prophylaxis) Exposure from a source with a low HIV titer also must be considered.
| Regimen | Duration of drug | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Application | Drug regimen | ||||||||||
| Category | intake | ||||||||||
| Basic | For occupational exposure with recognized transmission risk. | zidovudine (600 mg) 300 b.d. or 200 t.i.d or 100 mg q.i.d. | 4 weeks (28 days) | ||||||||
| lamivudine (150 mg) b.d. | |||||||||||
| Expanded | For occupational HIV exposures with increased risk of transmission. (Eg. larger volume of blood and/or higher virus titre in blood). | Basic regimen plus indinavir 800 mg t.i.d. | 4 weeks (28 days) | ||||||||
| or | |||||||||||
| basic regimen plus nelfinavir 750 mg t.i.d. |
Table 3: Basic and expanded Post Exposure Prophylaxis (PEP) regimens [6].
(Adapted from MMWR (Morbidity and mortality weekly report) Recommendations and reports Public Health Service Guidelines for the management of healthcare worker exposures to HIV and recommendations for post exposure prophylaxis)
PEP Toxicity
Antiretrovirals may be associated with side effects and in some cases are tolerated less well by HIV negative individuals. Possible side-effects include nausea, diarrhea, muscular pain and headache. Most side-effects are mild and transient, though possibly uncomfortable. Symptomatic management may improve tolerability of PEP; mostly antiemetics and antidiarrheal medications are prescribed with PEP starter packs. Proximal renal tubular dysfunction and Fanconi’s syndrome have been reported in HIV positive patients receiving tenofovir [24, 39, 40, 41].
Management of PEP Toxicity
Drug toxicity monitoring should be performed at baseline and again 2 weeks after starting PEP. A complete blood count, renal and liver function tests (transaminases) may be performed at the beginning of treatment (as baseline) and after 4 weeks. Side effects should be explained before initiating PEP so that the symptoms are not confused with symptoms of seroconversion to HIV. Regular monitoring is important throughout the course of PEP in order to detect these abnormalities, consistent with guidelines [10]. Clinical judgment, based on medical conditions that may exist in the HCW and any toxicity associated with drugs included in the PEP regimen, should determine the scope of testing. Monitoring include a complete blood count and renal and hepatic chemical function tests. Potential for Drug–Drug Interactions: It is essential to ensure that the potential for drug–drug interactions is considered with the use of PEP. Clinicians are advised to liaise with an HIV specialist pharmacist and/or use online tools. Follow-up measures include:
- Refraining from donation of blood, tissue, semen, or organs especially during the first 6-12 weeks following exposure.
- Avoiding sexual intercourse, becoming pregnant, or breastfeeding.
- Follow-up HIV antibody testing at 4 and 12 weeks.
- Rechecking of CBC, renal function and hepatic function at 2 and 4 weeks.
- Adherance and side effects counseling should be provided and reinforced at every follow-up visit. Laborotory Follow-Up: Testing at 4-6 weeks may not be enough as use of PEP may prolong the time to seroconversion; and there is not enough time to diagnose all persons who sera convert. Therefore, testing at 3
months and again at 6 months is recommended [10] (Table 3).
| Timing | In persons taking PEP (standard regimen) | In persons not taking PEP | ||||||
| Weeks 2 and 4 | Transaminases | Clinical monitoring for hepatitis | ||||||
| Complete blood count | ||||||||
| Week 6 | HIV-Ab | HIV-Ab | ||||||
| Month 3 | HIV-Ab, anti- HCV, HBsAg | HIV-Ab, anti-HCV, HBsAg | ||||||
| Transaminases | ||||||||
| Month 6 | HIV-Ab, anti-HCV, HBsAg | HIV-Ab, anti-HCV, HBsAg | ||||||
| Transaminases |
Table 4: Recommended follow up laboratory tests [10] (Adapted from Post Exposure Prophylaxis (PEP) – NACO Guidelines) The Basic S
Table 3: Recommended follow up laboratory tests [10] (Adapted from Post Exposure Prophylaxis (PEP) – NACO Guidelines) The Basic Services Division of National AIDS Control Organization, India provides HIV Counseling and testing services for HIV infection, the critical first step in detecting and linking people with HIV to access treatment. An integrated counseling and testing center is a place where a person is counseled and tested for HIV, on his own free will or as advised by medical provider and convinced that the test is mandatory. They provide early detection of HIV, basic information related to different modes of transmission and prevention of HIV/AIDS to develop behavioral change and lower vulnerability, helps to link positive people with other HIV prevention, care and treatment services, follow up counselling, prevention of Parent to Child Transmission (PPTCT), Cross referrals (HIV/Tuberculosis collaborative activities). Around 8000 ICTCs are present in India across various states [10].
Conclusion
Every health care worker must observe precautions to prevent transmission of HIV in their daily work. Each patient who undergoes any medical procedure should be treated as a potential carrier of HIV. If, despite the precautions, there is needle stick or any other exposure to potentially infectious material by health care personnel, they need to report it immediately to the appropriate staff in the workplace to assess the risks of infection at the earliest and to implement appropriate steps to prevent the progress of HIV infection, including the PEP prevention. Underestimation of the slightest contamination with infectious material in body may be fatal for health in the future; Hence, it is important to react adequately to possible exposure [5].
1. (2017) HIV.
2. Bartlett JB, Weber DJ (2017) Management of healthcare personnel exposed to HIV. UpToDdate.
3. Joyce PM, Kuhar D, Brooks JT (2015) Notes from the Field: Occupationally acquired HIV infection among Health Care Workers — United States, 1985–2013. MMWR Morb Mortal Wkly Rep 63(53): 1245-1246.
4. International Healthcare Worker Safety Center,
University of Virginia. U.S. EPI Net Sharps Injury and Blood and Body Fluid Exposure Surveillance Research Group. Blood and Body Fluid Exposure Report for 2009; 32 hospitals contributing data, 329 total exposures.
5. Wyżgowski P, Rosiek A, Grzela T, Leksowski K (2016)
Occupational HIV risk for health care workers: risk factor and the risk of infection in the course of professional activities. Ther Clin Risk Manag 12: 989- 994.
6. MMWR (Morbidity and mortality weekly report) Recommendations and reports (1998) Public Health Service Guidelines for the Management of HealthCare Worker Exposuresto HIV and Recommendations for Postexposure Prophylaxis. Centers for Disease Control (CDC) 47: 1-28.
7. (1988) Perspectives in Disease Prevention and Health
Promotion Update: Universal Precautions for Prevention of Transmission of Human Immunodeficiency Virus, Hepatitis B Virus, and Other
Bloodborne Pathogens in HealthCare Settings. MMWR 37(24): 377-388.
8. Lee AK, Ip HM, Wong VC (1978) Mechanisms of maternal fetal transmission of hepatitis B virus J Infect Dis 138(5): 668-671.
9. Lifson AR (1988) Do alternate modes for transmission of human immunodeficiency virus exist? A review. JAMA 259(9): 1353-1356.
10. Post Exposure Prophylaxis (PEP) – NACO Guidelines.
11. Bell DM (1997) Occupational risk of human immunodeficiency virus infection in healthcare workers: an overview. Am J Med 102(5B): 9-15.
12. Ippolito G, Puro V, De Carli G (1993) The risk of occupational human immunodeficiency virus infection in health care workers. Italian Multicenter Study. The Italian Study Group on Occupational Risk of HIV Infection. Arch Intern Med 153(12): 1451- 1458.
13. Fisman DN, Harris AD, Rubin M, Sorock GS, Mittleman
MA (2007) Fatigue increases the risk of injury from sharp devices in medical trainees: results from a case- crossover study. Infect Control Hosp Epidemiol 28(1): 10-17.
14. Avidan MS, Jones N, Pozniak AL (2000) The
implications of HIV for the anaesthetist and the intensivist. Anaesthesia 55(4): 344-354.
15. Kelen GD, Fritz S, Qaqish B, Brookmeyer R, Baker JL,
et al. (1988) Unrecognized human immunodeficiency virus infection in emergency department patients. N Engl Med 318: 1645-1650.
16. Mason JO (1987) Recommendations for Prevention of HIV Transmission in HealthCare Settings. Centers for Disease Control and Prevention MMWR 36(2): 1S- 18S.
17. Miles AJ, Wastell C, Allen Mersh T G (1989) Protection
for the left index finger whilst operating on HIV positive patients. Ann R Coll Surg Engl 71: 225.
18. Centers for Disease Control and Prevention (2014)
Preexposure Prophylaxis for HIV Prevention in the United States –2014. A Clinical Practice Guideline.
19. Centers for Disease Control and Prevention (2014)
Preexposure Prophylaxis for the Prevention of HIV in the United States – 2014. Clinical Providers’ Supplement.
20. Pinto LA, Landay AL, Berzofsky JA, Kessler HA,
Shearer GM (1997) Immune response to human immunodeficiency virus (HIV) in health care workers occupationally exposed to HIV contaminated blood. Am J Med 102(5B): 21-24.
21. Spira AI, Marx PA, Patterson BK, Mahoney J, Koup RA,
et al. (1996) Cellular targets of infection and route of viral dissemination after anintravaginal inoculation of simian immunodeficiency virus into rhesus macaques. J Exp Med 183(1): 215-225.
22. Miller RJ, Cairns JS, Bridges S, Sarver N (2000) Human
immunodeficiency virus and AIDS: insights from animal lentiviruses. J Virol 74(16): 7187-7195.
23. Bourry O, Mannioui A, Sellier P, Roucairol C, Durand-
Gasselin L, et al. (2010) Effect of a shortterm HAART on SIV load in macaque tissues is dependent on time of initiation and antiviral diffusion. Retrovirology 7: 78.
24. Sultan S, Benn P, Waters L (2014) Current
perspectives in HIV post exposure prophylaxis. HIV AIDS (Auckl) 6: 147-158.
25. Roedling S, Reeves I, Copas AJ, Beattie A, Edwards SG,
et al. (2008) Changes in the provision of post exposure prophylaxis for HIV after sexual exposure following introduction of guidelines and publicity campaigns. Int J STD AIDS 19(4): 241-242.
26. Day S, Mears A, Bond K, Kulasegaram R (2006) Post
exposure HIV prophylaxis following sexual exposure: a retrospective audit against recent draft BASHH guidance. Sex Transm Infect 82(3): 236-237.
27. Parkin JM, Murphy M, Anderson J, ElGadi S, Forster G,
et al. (2000) Tolerability and side effects of post exposure prophylaxis for HIV infection. Lancet 355(9205): 722-723.
28. Kahn JO, Martin JN, Roland ME, Bamberger JD,
Chesney M, et al. (2001) Feasibility of postexposure prophylaxis (PEP) against human immunodeficiency virus infection after sexual or injecting drug use exposure: the San Fransisco PEP Study. J Infect Dis 183(5): 707-714.
29. Roland ME, Neilands TB, Krone MR, Katz MH, Franses
K, et al. (2005) Seroconversion following
nonoccupational postexposure prophylaxis against HIV. Clin Infect Dis 41(10): 1507-1513.
30. Jochimsen EM, Luo CC, Beltrami JF, Respess RA,
Schable CA, et al. (1999) Investigations of possible failures of postexposure prophylaxis following occupational exposures to human immunodeficiency virus. Arch Intern Med 159(19): 2361-2363.
31. UK Collaborative Group on HIV Drug Resistance. UK
Collaborative HIV Cohort Study. UK Register of HIV Seroconverters (2007) Evidence of a decline in transmitted HIV-1 drug resistance in the United Kingdom. AIDS 21(8): 1035-1039.
32. Vercauteren J, Wensing AM, van de Vijver DA, Albert J,
Balotta C, et al. (2009) Transmission of drug resistant HIV-1is stabilizing in Europe. J Infect Dis 200(10): 1503-1508.
33. Poles MA, Elliott J, Vingerhoets J, Michiels L, Scholliers
A, et al. (2001) Despite high concordance, distinct mutational and phenotypic drug resistance profiles in human immunodeficiency virus type 1 RNA are observed in gastrointestinal mucosal biopsyspecimens and peripheral blood mononuclear cells compared with plasma. J Infect Dis 183(1): 143- 148.
34. Else LJ, Taylor S, Back DJ, Khoo SH (2011)
Pharmacokinetics of antiretroviral drugs in anatomical sanctuary sites: the male and female genital tract. Antivir Ther 16(8): 1149-1167.
35. Boyce JM, Pittet D, Healthcare Infection Control
Practices Advisory Committee, HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force
(2002) Guideline for Hand Hygiene in Health-Care Settings. Recommendations of the Healthcare Infection Control Practices Advisory Committee and the HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force. Society for Healthcare Epidemiology of America/Association for Professionals in Infection Control/Infectious Diseases Society of America. MMWR Recomm Rep 51(RR-16): 1-45.
36. Landovitz RJ, Currier JS (2009) Clinical practice.
Postexposure prophylaxis for HIV infection. N Engl J Med 361(18): 1768-1775.
37. Zingman BS (2013) HIV Prophylaxis Following
Occupational Exposure. New York Department of Health AIDS Institute.
38. Kuhar DT, Henderson DK, Struble KA, Heneine W,
Thomas V, et al. (2013) Updated US Public Health Service Guidelines for the Management of Occupational Exposures to Human Immunodeficiency Virus and Recommendations for Postexposure Prophylaxis. Infect Control Hosp Epidemiol 34(9): 875-892.
39. Williams I, Churchill D, Anderson J, Boffito M, Bower
M, et al. (2012) British HIV Association guidelines for the treatment of HIV-1-positive adults with antiretroviral therapy 2012. HIV Medicine 13(2): 1- 85.
40. Truvada film coated tablets Gilead Sciences Ltd
(2014).
41. Viread 245 mg film coated tablets Gilead Sciences Ltd
(2014).
42. New York State Department of Health AIDS Institute.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey