Mucocele: A Case Report with Literature Review
Mucoceles (Muco-mucus and coele-cavity) are cavities filled with mucus. They are one of the most common benign soft tissue masses that occur in the oral cavity. Two types of distinct entities described in relation to the mucoceles include the true mucous retention cysts which are lined with epithelium and the mucous extravasation cysts which occur because of pooling of the mucus into the adjacent tissues in case of trauma to the conducting passages or, ducts. The two main etiological factors for mucoceles are obstruction of salivary gland ducts leading to the so-recognized true mucous retention cysts and traumatic injuries to the mucous carrying ducts leading to the creation of the so-called mucous extravasation cysts. Mucoceles are commonly seen in relation to the lower lip often because of the lip-biting habit leading to the formation of mucous extravasation cysts. The lesions can be solitary or, multiple, often rupturing and leaving, slightly painful erosive areas that usually heal within a span of few days. The lesions may rupture spontaneously with the liberation of a viscous fluid, however, after a few days to weeks, additional fluid accumulates and the lesion is seen to recur. This cycle of rupture, collapse and refilling may continue for months. The present case report presents one such case of a mucocele that was reported in the Department for diagnosis and further, needful.
Introduction
Mucoceles (Muco-mucus and coele-cavity) are cavities filled with mucus. They are one of the most common benign soft tissue masses that occur in the oral cavity. Two types of distinct entities described in relation to the mucoceles include the true mucous retention cysts which are lined with epithelium and the mucous extravasation cysts which occur because of pooling of the mucus into the adjacent tissues in case of trauma to the conducting passages or, ducts [1]. Mucous extravasation cysts do not have an epithelial lining and are surrounded by compressed connective tissue cells. In some cases, only granulation tissue is present surrounding the pooled mucous. The two main etiological factors for mucoceles are obstruction of salivary gland ducts leading to the so- recognized true mucous retention cysts and traumatic injuries to the mucous carrying ducts leading to the formation of the so-called mucous extravasation cysts [2]. Mucoceles are commonly seen in relation to the lower lip often because of the lip-biting habit leading to the formation of mucous extravasation cysts [3].
The said lesions are, also, rarely seen in relation to the upper lip, retro molar area and/or, palatal area. Mucoceles may occur at any age but are seen most frequently in the second and third decade of life [2]. These lesions have no sex predilection and occur more frequently in children, adolescents and young adults. The lesions can be solitary or, multiple, often rupturing and leaving, slightly painful erosive areas that usually heal within a span of few days. The diagnosis of mucoceles is not difficult [4]. Generally, mucoceles are small in size, often approximately 1 to 2 mm in size, appearing as painless, superficial, well-circumscribed swellings on the mucosa. The color of the lesions is variable, often, translucent or, bluish. The lesions may rupture spontaneously with the liberation of a viscous fluid, however, after a few days to weeks, additional fluid accumulates and the lesion is seen to recur. This cycle of rupture, collapse and refilling may continue for months. The present case report presents one such case of a mucocele that was reported in the Department for diagnosis and further, needful with a short overview of the existing literature regarding the origin, the etio- pathogenesis and a review of the possible treatment modalities available [5].
Case Report
A male patient aged 32 years reported to the Department with a chief complaint of an intra-oral Abhishek Singh Nayyar, et al. Mucocele: A Case Report with Literature Review. Med J Clin Trials Case Stud 2018, 2(5): 000177.
swelling over right side of the lower lip for past 20 days. The history of presenting illness revealed similar lesions in the past that resolved on their own. On examination, a solitary, well-circumscribed, oval-shaped swelling measuring about 0.5 to 1cm in its largest diameter with a smooth, shiny surface and having a slightly bluish hue, was present in relation to the lower right labial mucosa in # 43,44 region. The swelling was painless and was reported to be initially small in size by the patient at the onset which gradually increased in size to attain the present size (Figure 1). On palpation, all the inspectory findings were confirmed. The swelling was soft in consistency, non- tender and fluctuant. The temperature of the overlying surface was normal and the associated lymph nodes of the region were non-palpable. The patient had no significant medical history. Extra-oral examination revealed no remarkable findings. The patient reported accidental biting of the lower lip while having food about 4 months ago. Based on above history and clinical examination of the patient, a provisional diagnosis of mucocele was arrived-at while the important differentials included a fibroma, lipoma and hemangioma.
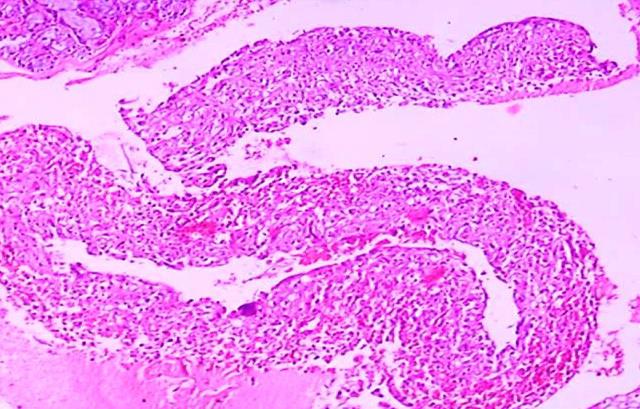
For making the differential, the relatively, well-known and simple, clinical slip sign for lipomas and diascopy procedure for lesions of vascular origins including hemangiomas was performed and were found to be negative. The patient was, thus, advised with excisional biopsy of the lesion along with removal of the affected adjacent minor salivary gland tissue. Routine blood investigations came-out to be within normal range. A written, informed consent was obtained from the patient to proceed with the surgical treatment for the excision of the lesion under aseptic conditions. Surgical excision of the lesion was performed under local anesthesia by placing a horizontal incision over the lesion (Figure 2). The cystic lesion was separated from the underlying mucosa and connective tissue carefully so that the chances of recurrence were reduced while hemostasis was achieved (Figure 3). The lesional site was, then, sutured (Figure 4) and requisite post-operative instructions were provided to the patient avoiding any further injury to the operative and lesional area. The patient was, also, prescribed with antibiotic and analgesic coverage for a period of 5 days and the patient was recalled for suture removal after a week. The excised tissue was sent for histopathological examination which revealed the lesional tissue to be composed of minor salivary gland tissue with pooled mucinous areas and Copyright© Abhishek Singh Nayyar, et al.
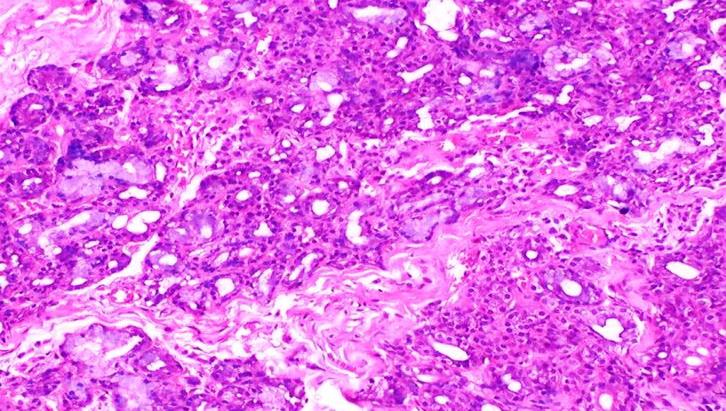
chronic inflammatory cell infiltration (Figure 5). Granulation tissue was, also, seen with proliferating and engorged blood vessels interspersed with chronic inflammatory cells and with abundance of mucinophages (Figure 6) suggestive of mucous extravasation cyst. Correlating the history and clinical examination of the patient with the histopathological findings, a final diagnosis of mucous extravasation type of mucocele was made. The patient was found with uneventful recovery and is still on follow-up for checking for any possible recurrences of the lesion.


Abhishek Singh Nayyar, et al. Mucocele: A Case Report with Literature Review. Med J Clin Trials Case Stud 2018, 2(5): 000177.


Copyright© Abhishek Singh Nayyar, et al.
Discussion
Mucocele is a benign cystic lesion of the oral cavity that has been ranked the seventeenth most common benign salivary gland lesion and the second most common benign soft tissue tumor occurring in the oral cavity. The incidence of mucocele is generally high, 2.5 per 1000 patients, frequently occurring in the second decade of life and rarely in children and infants under one year of age [1]. Various etiological factors that have been put forth for the occurrence of mucoceles include obstruction of the salivary gland ducts, traumatic injuries to the ducts which are either pinched or, severed, trauma to the secretory acini and rarely, congenital atresia of the duct orifices apart from a plethora of other abnormalities and cysts and tumors [4]. There is no specific age or, sex predilection for the occurrence of these lesions, however, it has been reported that mucous retention cysts occur more frequently in the elderly patients while extravasation cysts occur more commonly in the younger age groups [2]. Majority of mucoceles are seen in relation to the lower lip while they can occur anywhere in the oral cavity with the exception of the anterior areas of the hard palate which are devoid of salivary glands [4, 5]. Mucous extravasation cysts do not have an epithelial lining and are often seen as poorly defined mucinous pools containing eosinophilic mucinous material and vacuolated macrophages, granulation tissue and condensed fibrous tissue. In some cases, only granulation tissue is present surrounding the pooled mucous Abhishek Singh Nayyar, et al. Mucocele: A Case Report with Literature Review. Med J Clin Trials Case Stud 2018, 2(5): 000177.
containing lymphocytes, polymorphonuclear leukocytes and eosinophils. Mucous retention cysts, on the contrary, are partly or, completely lined by epithelium, stratified squamous epithelium or, cuboidal cells or, pseudostratified columnar epithelium with macrophages often associated with the epithelium lining. Mucous extravasation cysts are more common in children and are seen because of traumatic injuries to the mucous carrying ducts leading to extravasation of saliva and mucous often surrounded by inflammatory cells followed by granulation tissue composed mainly of fibroblasts [2, 3]. Due to absence of a well defined, epithelial lining, these lesions are categorized as pseudo- and/or, false cysts. Conventional treatment for mucoceles is the surgical extirpation of the cystic lesions, surrounding mucosa and the glandular tissue [2, 4]. With a simple, stab incision of the mucocele, the content would drain-out but the lesion has high chances of recurrence. Surgical excision of the lesion with removal of the affected accessory salivary glandular tissue is, thus, suggested as the treatment of choice for avoiding recurrence of the lesion. Laser ablation, cryosurgery and electrocautery are the other suggested treatment options that have a conservative, non-invasive approach that further avoids trauma to the adjacent minor salivary gland tissues which is the main cause cited for the recurrence of such lesions with surgical treatment, though; they have been used for the treatment of mucoceles with variable success [5]. Mucoceles are one of the most common soft tissue lesions of the oral cavity which cause distress and discomfort to the patients [6, 7]. Majority of the lesions are often diagnosed clinically, however, biopsy is sometimes found mandatory to rule-out other possible rarities [1]. The possible differential diagnoses include fibromas, lipomas and hemangiomas. For differentiating a mucocele from these lesions, further investigations are often found necessary including the relatively, well-known and simple, clinical slip sign for differentiating mucoceles from lipomas and the relatively simple, diascopy procedure used to differentiate mucoceles from and characteristic for lesions of vascular origins like hemangiomas. In the present case, too, such rarities were ruled-out on the basis of these simple, chair side diagnostic adjuncts and thus, excisional biopsy was advised and performed [1, 3]. The management of mucoceles becomes challenging because of high possibility of recurrence, however, if no spontaneous regression occurs, surgical excision with dissection of the surrounding and contributing minor salivary gland tissue often leads to clinical success without recurrence and better prognosis [5, 6].
Copyright© Abhishek Singh Nayyar, et al.
References
-
Yamasoba T, Tayama N, Syoji M, Fukuta M (1990) Clinico-statistical study of lower lip mucoceles. Head Neck 12(4): 316-320.
-
Sugerman PB, Savage NW, Young WG (2000) Mucocele of the anterior lingual salivary glands (glands of Blandin and Nuhn): Report of 5 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 90(4): 478-482.
-
Anastassov GE, Haiavy J, Solodnik P, Lee H, Lumerman H (2000) Submandibular gland mucocele: Diagnosis and management. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 89(2): 159-163. Abhishek Singh Nayyar, et al. Mucocele: A Case Report with Literature Review. Med J Clin Trials Case Stud 2018, 2(5): 000177.
-
Martins-Filho PR, Santos Tde S, da Silva HF, Piva MR, Andrade ES, et al. (2001) A clinicopathologic review of 138 cases of mucoceles in a pediatric population. Quint Int 42(8): 679-685.
-
Bodner L, Tal H (1991) Salivary gland cysts of the oral cavity: Clinical observation and surgical management. Compendium 12(3): 150,152,154-156.
-
Yagüe-García J, España-Tost AJ, Berini-Aytés L, Gay- Escoda C (2009) Treatment of oral mucocele: Scalpel versus CO2 laser. Med Oral Patol Oral Cir Bucal 14(9): e469-474.
-
Huang IY, Chen CM, Kao YH, Worthington P (2007) Treatment of mucocele of the lower lip with carbon dioxide laser. J Oral Maxillofac Surg 65(5): 855-858. Copyright© Abhishek Singh Nayyar, et al.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey