Case Report Neonatal Stroke
Stroke is a brain injury caused by the interruption of blood flowing to part of the brain. A neonatal stroke is a disturbance in the blood supply to an infant’s brain in the first 28 days of life [1]. This includes both ischemic events, which result from a blockage of vessels, and hemorrhagic events, which result when a blood vessel ruptures and bleeds. A neonatal stroke occurs in approximately 1 in 4,000 births.
Najia al H*, Attiaalzahrani, Ibrahiumkotbi, Helalalmalki, Amal
Zubani, Marwayosef, Emad H and Abdulsamee AA
Maternity and Children Hospital, Kingdom of Saudi Arabia
Kingdom of Saudi Arabia, E-mail: najoo_n1@yahoo.com neonatal stroke occurs in approximately 1 in 4,000 births.
Keywords: Neonatal Stroke; Chorioamnionitis; Homocysteine; Coagulopathy; Prothrombin
Introduction
According to the National Institutes of Health (NIH), a neonatal stroke is a medical condition that occurs when an infant’s blood supply is disturbed within the first 28 days of life. If an infant has a stroke within the first 7 days of life, it’s known as a perinatal stroke. Both strokes are described as the brain experiencing both a hypoxic event (oxygen deprivation) and a blockage to the blood vessels. Doctors estimate that about 1 in every 4,000 babies experience a neonatal stroke. One of the causes of neonatal stroke is hypoxia, an event when oxygen deprivation causes the brain to panic.
The health of the mother can sometimes affect whether a child will have a neonatal stroke, especially if she has disorders such as: autoimmune disorders, coagulation disorders, prenatal cocaine exposure, infection, congenital heart disease, diabetes, and trauma. Factors that can affect a neonatal stroke during pregnancy include: placental abruption, placental infection, and chorioamnionitis [2]. Other miscellaneous disorders affecting the mother and/or baby’s health and resulting in a neonatal stroke include: blood, homocysteine, and lipid disorders (such as polycythemia, disseminated intravascular coagulopathy, prothrombin mutation, lipoprotein a deficiency, factor VIII deficiency, and factor V Leiden mutation.
A neonatal stroke can also be caused by maternal infection through infections affecting the central nervous system or other systemic infections. However, several parents and doctors are worried as the cause of a neonatal stroke isn’t always obvious: some healthy children born after an uncomplicated pregnancy and normal labor and delivery may still experience a neonatal stroke. Prenatal stork can occur in any times between 20 weeks gestation and 28 days [1]. Incidance: 0.2 -1 per 1000 live birth
Types
Perinatal arterial Ischemic stork is the most types of stork are the middle cerebral arteries. Hemorrhagic: may be parenchyma. Subarachnoid, intraventricular. Cerebral Sino venous thrombosis can be causes infarction with hemorrhage. Based on neuroimaging, Stock can be classified as prenatal if occur before delivery, Neonatal stroke if occur in 1st 4 weeks of life smother on breast feeding had convulsion at the age of 16 hour old neonatology at a glance [3]. Etiology: The etiology of perinatal stroke is thought to be multi factorial. There have been studies associating neonatal stroke with intrapartum factors such as prolonged rupture of membranes, maternal fever, prolonged second stage of delivery, and tight nuchal cord. In addition, both maternal- and infant-related prothrombotic conditions have been implicated. another major group of risk factors are pathologies of the placenta. It has been observed that the placentas of neonates with arterial ischemic stroke have signs of blood supply problems, which could exacerbate during delivery. Unfortunately, the role of the placenta is relatively poorly exposed, because the placenta is often unavailable by the time the stroke is diagnosed [3]. Risk Factor: Many different risk factors play a role in causing a neonatal stroke. Some maternal disorders that may contribute to neonatal strokes include: autoimmune disorders, coagulation disorders, prenatal cocaine exposure, infection, congenital heart disease, diabetes, and trauma. Placental disorders that increase the risk of stroke include placental thrombosis, placental abruption placental infection, and chorioamnionitis. Other disorders that may increase the risk of a neonatal stroke are blood homocysteine and lipid disorders, such as polycythemia, disseminated intravascular coagulopathy, prothrombin mutation lipoprotein (a) deficiency, factor VIII deficiency (hemophilia A), and factor V Leiden mutation, Infectious disorders such as central nervous system (CNS) infection or systemic infection may also contribute. Many infants
who suffer a neonatal stroke also follow an uncomplicated pregnancy and delivery without identifiable risk factors, which exemplifies the necessity for further research on this subject [4].
Case
Full term delivered by C/section due antepartum hemorrhage with good Apgar shifted beside mother, noticed at age of 12 hours she had convulsion admitted direct to NICU, Immediately, RBS, CALCIUM, MG, NA, check it was normal, no history of maternal fever no prolonged rupture of membrane.
On Examination
No dimorphic feature. No skin rash, no hypo or hyperpigmentation. Vital sign is normal temperature =37HeartR ate =140/min RR=40 SAT=99BP= Normal. Chest is good breath sound bilateral. Cardiovascular 1st and 2nd heart sound is normal no murmur CRT =2 Second BP IS normal for age. Abdomen is soft no hepatosplenomegaly. Neurological exam he hypertonic seizure aborted by iv phenobarbitone, pupil is reactive and normal size and shape No muscle weakness.
Investigation
CBG is normal, CBC within normal limit, Chemistry within normal limit, Coagulation profile within normal, protein S was normal, Protein C was normal. Fibrinogen was normal, Urgent CT scan brain done showed infarction of middle cerebral artery with subarachnoid hemorrghe.
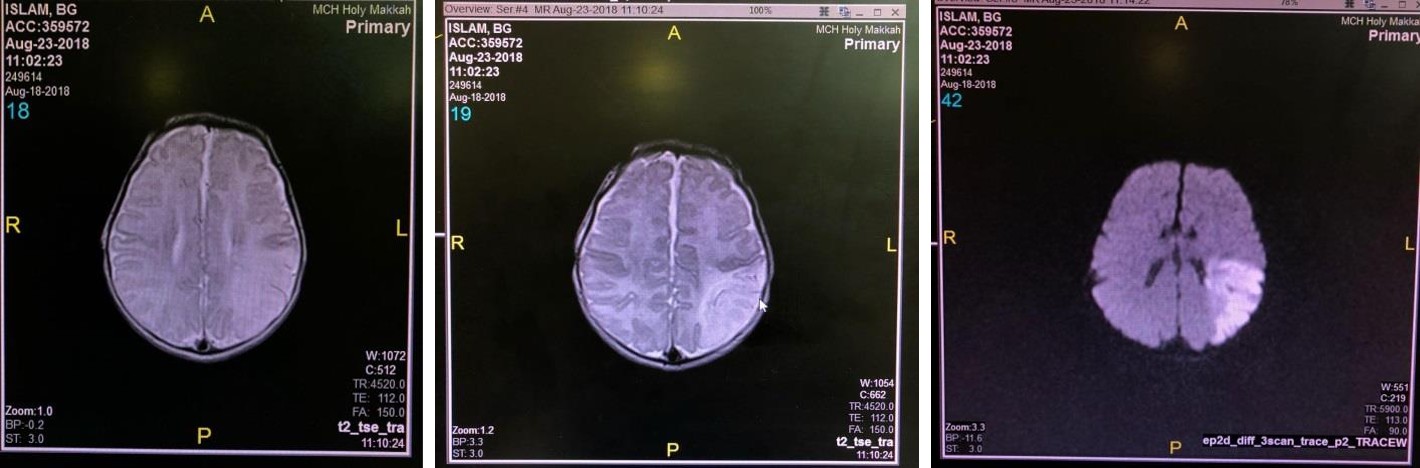
Figure: MRI Report.
There is redemonstration of acute ischemic stock with restricted diffusion noted involving left parietal cortico- subcortical region left MCA territory with effacement of adjacent b cortical sulci.
Management
Baby admitted in NICU convulsion aborted by phenobarbitone hematologist consultation order for MRE Brain showed infarction of middle cerebral artery, baby doing well sucking well, Therapeutic Hypothermia. Hypothermia treatment induced by head cooling or systemic cooling administered within 6 hours of birth for 72 hours has proven beneficial in reducing death and neurological impairments at 18 months of age. This treatment does not completely protect the injured brain and may not improve the risk of death in the most severely hypoxic-ischemic neonates and has also not been proven beneficial in preterm infants [5]. Combined therapies of hypothermia and pharmacological agents or growth factors to improve neurological outcomes are most likely the next direction for damaged neonatal brains, such as after a stroke other Treatments [5]. A successful use of urokinase in a newborn with an aortic clot has been reported, but the bleeding risks associated with thrombolytic agents are still unclear. Heparin, an anticoagulant, treatments have been used in cases of cerebro-venous sinus thrombosis (CVST) in order to stop thrombosis extension and recurrence, to induce thrombosis resolution, and to prevent further brain damage [5]. In the case of extremely high intracranial pressure, surgical removal of hematoma may be beneficial [2].
Outcome Prediction
Early prediction of long-term neurological outcome is important to families and facilitates patient selection for clinical trials. The ability of clinical, laboratory, and EEG measures to predict outcomes has been limited. 22, 46 Neuroimaging findings may be more predictive including lesion size and location. 5,23,46,47 Diffusion magnetic resonance imaging markers of corticospinal tract Wallerian degeneration seem to predict adverse motor outcomes. 48,49 Acute diffusion imaging may also demonstrate changes in connected brain structures, so- called diaschisis or network injury, associated with outcome.50 Early diffusion tensor imaging may also assess functional tract integrity in NAIS with implications for long-term outcome prediction
Discussion
As the mother she does not follow up she did not suffer from any disease, she is not diabetics, no blood disease, no infection, no congenital heart disease, she was UN book placenta infection and placenta thrombosis cannot roll out. Many infants who suffer a neonatal stroke also follow an uncomplicated pregnancy and delivery without identifiable risk factors, which exemplifies the necessity for further research on this subject.
References
-
Aden U (2009) Neonatal Stroke Is Not a Harmless Condition. Stroke 40(6): 1948-1949.
-
Neonatal stroke Birth injury guide.
-
Tom Lissauer, Avroy A Fanaroff, Lawrence Miall, Jonathan Fanaroff (2015) Neonatology at a Glance, 3rd (Edn.).
-
Sehgal A (2012) Perinatal Stroke: a case-based review. Eur J Pediatr 171(2): 225-234.
-
Rees S, Harding R, Walker D (2011) The biological basis of injury and neuroprotection in the fetal and neonatal brain. Int J Dev Neurosci 29(6): 551-556.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey