Ovarian Granulocytic Sarcoma in a Patient with Philadelphia Chromosome–Positive Acute Biphenotypic Leukemia: Case Report
Granulocytic sarcoma is a rare neoplastic condition consisting of immature myeloid cells at an extra medullary site. We report a very infrequent case of ovarian granulocytic sarcoma in a patient with Philadelphia chromosome-positive acute biphenotypic leukemia who underwent emergency laparoscopic surgery (salpingo-oophorectomy), because an acute abdomen presentation. As far as we know, granulocytic sarcoma and biphenotypic leukemia (BAL) association have been described only four times in literature.
Introduction
Granulocytic sarcoma (GS) is a rare neoplastic condition consisting of immature myeloid cells occurring at an extra medullary site that most frequently corresponds to the bone, skin, peritoneum or lymph nodes, although any part of the body may be affected. It is also called extra medullary myeloblastoma or chloroma, because typical forms have a green color caused by the enzyme myeloperoxydase (MPO) in immature cells [1]. It has been observed more frequently in patients with acute myelogenous leukemia, chronic myelogenous leukemia, and other myeloproliferative disorders [2].
GS may occur at any age both in pediatric and adult patients. The diagnosis is performed by biopsy of the tumor; according to the localization of the tumor, magnetic resonance or computed tomography must be performed. The treatment depends on the localization of the tumor, whether it is a recent diagnosis or a relapse, the performance status and the patient's age [3].
The aim of this study is to present an ovarian GS case in a female patient with Philadelphia chromosome- positive acute biphenotypic leukemia, which is a very uncommon type of leukemia, who underwent emergency surgery, as she presented to the emergency room, with an acute abdomen with a big abdominal mass in the right iliac fossa.
Case Presentation
The patient is a 29-year-old woman with hematologic diagnosis of Philadelphia chromosome–positive acute biphenotypic leukemia in 2017. The bone marrow aspiration showed hypocellular medulla, decreased megakaryocytes, normoblasts 6%, blasts 5%, young granulocytes 16%, adult granulocytes 9%, monocytes 8% with <10% dysplasia. Inversion of the myeloid/erythroid ratio; an immunophenotype positive for both myeloid (CD13, CD33, CD34, CD117 and MPO) and lymphoid (CD19, CD10, CD34 and TdT); positive Philadelphia Chromosome BRC-ABL. The patient received fase 1 BFM induction protocol (weekly doses of anthracycline and vincristine/ nilotinib /steroid), suffering adverse effects such as bradichardia, hematotoxicity and mucositis. At the moment the GS diagnosis was made, the patient was receiving venetoclax and ponatinib (45mg). Recent hospitalizations included Ureaplasma urealyticum infection (November 2017), fase 1 BFM induction protocol (November 2017), cytopenia caused by intratecal treatment and molar extraction (December 2017), C. Difficile related chronic diarrhea (January 2018).
The patient referred beginning current condition one day prior to hospital admission with progressive abdominal pain. Her hematologist saw her the day of her hospitalization with exacerbation of pain, located in the right iliac fossa, accompanied by fever and general malaise, tender abdomen with a painful mass in the same region, with signs of peritoneal irritation. For this reason, she was sent to the ER. On examination, blood pressure 103/67mmHg, heart rate 103bpm, respiratory rate 18bpm, temperature 37ºC. Conscious, oriented, pale with mucous membranes dehydration. Cardiopulmonary examination was within normal limits. Distended abdomen, tenderness in lower right quadrant and a painful mass, as well as positive rebound and McBurney sign. Rest of examination was normal.
A complete blood count (CBC) was performed with the following results: red blood cells 3.45M/µL, hemoglobin (Hb) 10.3g/dL, white blood cells 88.5K/µL, lymphocytes 20%, segmented neutrophils 18%, band neutrophils 10/µL, platelet count 474 K/µL, promyelocytes 32%, myelocytes 12%, metamyelocytes 3%. Other laboratory results showed LDH 1.532 IU/L, Fe 17.9 µ/dL, D dimer 4642.7ng/mL, prothrombin time 19.7sec, activated partial thromboplastin time 36.9 sec, thrombin time 15 sec.
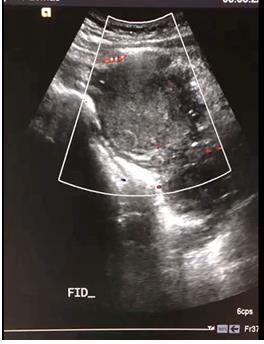
Pelvic USG: ovoid mass in the right iliac fossa, without vascularity at color Doppler, apparently and adnexal mass, considering hemorrhagic cyst or endometrioma (Figures 1 & 2). CT of abdomen and pelvis showed right adnexal mass probably a hemorrhagic cyst. Inflammatory changes of the mesentery towards hypogastrium and both iliac fossae with the presence of free fluid in the posterior cul- de-sac. Increase in left ovarian volume, considering possibility of pelvic inflammatory disease (Figures 3 & 4).

Weber A, et al. Ovarian Granulocytic Sarcoma in a Patient with Philadelphia Chromosome–Positive Acute Biphenotypic Leukemia: Case Report. Med J Clin Trials Case Stud 2019, 3(2): 000203.


For these reasons, an exploratory laparoscopy was performed. During the surgical procedure, a right ovarian ruptured hemorrhagic cyst was found, with an omentum plastron. Laparoscopic right salpingo-oophorectomy with a stapler was performed. Due to a postoperative 7.3g/dL Hb, the patient was transferred to the ICU, where she was transfused, and further assessment was indicated. There were no consequences or complications from surgery (Figures 5-7).


Weber A, et al. Ovarian Granulocytic Sarcoma in a Patient with Philadelphia Chromosome–Positive Acute Biphenotypic Leukemia: Case Report. Med J Clin Trials Case Stud 2019, 3(2): 000203.

The patient recovery was uneventful, she later received complementary chemotherapy and she recently underwent a bone marrow transplant and is well under close surveillance.
Discussion
k ‘ ’ mixture of both types of acute leukemias, acute myeloid leukemia (AML) and acute lymphoblastic leukemia. In biphenotypic leukemia, the leukemia cells have markers for two different types of cells on their surface, markers for lymphoid cells and also markers for myeloid cells, which are usually found in acute myeloid leukemia. Patients with biphenotypic leukemia usually have structural chromosome abnormalities including a high incidence of the Philadelphia chromosome as in this case, chromosome rearrangements and other abnormalities. BAL is a rare clinical entity. It is estimated that around 5% of people with acute leukemia have biphenotypic leukemia; its association with a sarcoma as in this case is even more rare, and mentioned only in few cases in literature [4].
GS was first described by Burns in 1811. In 1853 King named it chloroma, because of its typical yellow-green appearance secondary to its high MPO concentrations. In 2001, the World Health Organization (WHO), named it myeloid sarcoma, and classified it in 2 major categories: GS and Monoblastic Sarcoma [5].
It is a rare disease that can present as an isolated extra medullary leukemic tumor, concurrently with (as the case presented in this article), or at a relapse of leukemia. The majority of GSs are diagnosed at autopsy. Due to the rarity of the disease most of the case reported is small case series or case reports [6]. Oliva, et al. presented one of the few series of cases describing 11 patients diagnosed with GS of the female genital tract, 7 of which were ovarian [7, 8, 9, 10].
The gold standard for diagnosis is biopsy (that may be fine needle) completed by immunohistochemistry and immunophenotype. Touch preparations of the tissue obtained during the biopsy may be stained with enzyme cytochemical stains such as myeloperoxidase, Sudan black B, chloroacetate esterase, among others) [11]. Immunohistochemical stains are used widely including immature markers (such as CD34, CD117), as well as markers to help establish differentiation (MPO, CD56, CD68-R, lysozyme, CD33, CD14, CD163) [12, 13].
The overall survival and prognostic factors are unclear and to vary significantly depending on the patient's age, sex, race, and sites of presentation. The clinical presentation has a very wide variety of symptoms, depending of its localization. GS of the ovary usually presents as asymptomatic unilateral or bilateral solid mass, with possible cystic component, hemorrhage, and necrosis [14]. Presentation as an acute abdomen is very infrequent [2].
There is no consensus on optimal time and treatment for GS, as randomized prospective studies are lacking. The current treatment regimen must be targeted to the base hematologic pathology. Systemic treatment should be considered in all patients, as relapses and progression are part of the natural history of the disease in most cases [15]. Although frequently given concomitantly, the role of radiotherapy has not been established, as overall survival improvement has not been proven [5]. Surgery is an option for tumors causing organ dysfunction or obstruction. This patient received complementary chemotherapy and recently underwent a bone marrow transplant and is well under close surveillance [16].
Conclusion
Granulocytic sarcomas are rare hematological neoplasms due to extra medullary leukemic deposits. Ovarian presentations are further rare, but the association with biphenotipic leukemia is only reported in Weber A, et al. Ovarian Granulocytic Sarcoma in a Patient with Philadelphia Chromosome–Positive Acute Biphenotypic Leukemia: Case Report. Med J Clin Trials Case Stud 2019, 3(2): 000203.
other four cases in English literature as far as we know. This patient presented with an acute abdomen, and laparoscopic surgical treatment was successfully performed. Six months after surgery the patient undergone a bone marrow transplant and is currently under vigilance.
References
-
Campidelli C, Agostinelli C, Stitson R, Pileri SA (2009) Myeloid Sarcoma; Extramedullary Manifestation of Myeloid Disorders. Am J Clin Pathol 132(3): 426-437.
-
Guermazi A, Feger C, Rousselot P, Merad M, Benchiab N, et al. (2002) Granylocytic Sarcoma (Chloroma) Imaging Findings in Adults and Children. Am J Roentgenol 178(2): 319-325.
-
Yilmaz AF, Saydam G, Sahin F, Baran Y (2013) Granulocytic sarcoma: a systematic review. Am J blood Res 3(4): 265-270.
-
Khanna G, Nishikant DA, Agarwal S, Roy M, Jain D, et al. (2017) Mixed Phenotypic Acute Leukemia (mixed myeloid/B-cell) with Myeloid Sarcoma of the Thyroid Gland: A Rare Entity with Rarer Asssociation - Detected on FDG PET/CT. Indian J Nucl Med 32(1): 46-49.
-
Sabattini E, Bacci F, Sagramoso C, Pileri SA (2010) WHO classification of tumours of haematopoietic and lymphoid tissues in 2008: an overview. Pathologica 102(3): 83-87.
-
Park KU, Lee DS, Lee HS, Kim CJ, Cho HI (2001) Granulocytic sarcoma in MLL-positive infant acute myelogenous leukemia. Am J Pathol 159(6): 2011- 2016.
-
Avni B, Koren-Michowitz M (2011) Myeloid sarcoma: Current Approach and Therapeutic Options. Therapeutic advances in hematology 2(5): 309-316.
-
Ding J, Li H, Qi YK, Jian Wu, Ze-Bin Liu, et al. (2015) Ovarian granulocytic sarcoma as the primary manifestation of acute myelogenous leukemia. International Journal of Clinical & Experimental Pathology 8(10): 13552-6.
-
Samanta D, Sahoo TK, Roopesh K, Mohanty KR, Bose C, et al. (2016) Granulocytic Sarcoma of Ovary Associated with Chronic Myelogenous Leukemia Mimiking Carcinoma: A Rare Case Report. Journal of Cancer and Tumor International 3(2): 1-5.
-
Oliva E, Ferry JA, Young RH, Prat J, Srigley JR, et al. (1997) Granulocytic sarcoma of the female genital tract: a clinicopathologic study of 11 cases. Am J Surg Pathol 21(10): 1156-1165.
-
Suh YK, Shin HJ (2000) Fine-needle aspiration biopsy of granulocytic sarcoma: a clinicopathologic study of 27 cases. Cancer 25: 364-372.
-
Chang CC, Eshoa C, Kampalath B, Shidham VB, Perkins S (2000) Immunophenotypic Profile of Myeloid Cells in Granulocytic Sarcoma by Immunohistochemistry: Correlation With Blast Differentiation in Bone Marrow, Am J Clin Pathol 114(5): 807-811.
-
Alexiev BA, Wang W, Ning Y, Chumsri S, Gojo I, et al. (2007) Myeloid sarcomas: a hystologic, immunohistochemical, and cytogenetic study. Diagn Pathol 2: 42.
-
Goyal G, Bartley AC, Patnaik MM, Litzow MR, Al-Kali A, et al. (2017) Clinical features and outcomes of extramedullary myeloid sarcoma in the United States: analysis using a national data set. Blood Cancer J 7(8): e592.
-
Carrillo R, Estévez P, Muciño J (2012) Sarcoma granulocítico en una paciente con leucemia mieloide crónica. Revista de la Facultad de la UNAM 55(1): 22- 28.
-
Yilmaz AF, Saydam G, Sahin F, Baran Y (2013) Granulocytic sarcoma: a systematic review. American Journal of Blood Research 3(4): 265-270. Weber A, et al. Ovarian Granulocytic Sarcoma in a Patient with Philadelphia Chromosome–Positive Acute Biphenotypic Leukemia: Case Report. Med J Clin Trials Case Stud 2019, 3(2): 000203.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey