Gastric Cancer During Pregnancy; Torsion of Krukenberg Tumor (KT)
Ovarian tumor is very rare in pregnant women and only 5% of them are malignant and most of them appear as Krukenberg tumors (KT). The most common complication of ovarian tumors encountered in pregnancy is torsion. In this case, a 36-year-old, gestational age of 16 week pregnant woman who presented with ovarian mass torsion could not be evaluated clearly due to the result of her pathological evaluation being necrosis. After treatment, patient was readmited with a diagnosis of ovarian cyst in intact ovary and after surgery, was diagnosed as Advanced Gastric Cancer (AGC). Possibility of Krukenberg tumor should be kept in mind in patients diagnosed with torsion of ovarian mass and, with multidisciplinary evaluation of the patient, in the optimal period pregnancy must be terminated and primary tumor should be treated immediately.
Introduction
Pregnancy is not a predisposition condition to cancer and the incidence of malignant tumors during pregnancy usually appear in reproductive age. Although the most common cancers in pregnancy varry depending on the literature; breast cancer, cervical cancer, hematological malignancies and melanoma are the most common cancers. Lung and stomach cancers are rare, but have poor prognosis [1]. The incidence of ovarian tumors in pregnant women is 2.8 - 11 / 100.000 [2]. Of these tumors, 5% are malignant and most of them appear as Krukenberg tumors [3]. Today, due to the increase in pregnancies at advanced maternal age; cancer has began taking frequency in pregnant women. Most adnexal masses in pregnancies are represented by functional or corpus luteum cysts; It is detected in 11-41% of the pregnancies [4] and rarely exceeds 3-5 cm. 30% to 40% of metastatic ovarian cancer and Krukenberg tumors constitute 1% to 2% of all ovarian cancers [5] and are deadly tumors.
Since the resistant gastrointestinal symptoms caused by the Krukenberg tumor are similar to the physiological and hormonal changes in pregnancy, early diagnosis is often difficult. Krukenberg tumor contains a significant component of mucin-filled signet-ring cells lying within a cellular stroma of ovarian origin. The literature review demonstrate that about 76% of Krukenberg Tumour (KT) originate from stomach, 11% in colorectum, 4% from the breast, 3% from the biliary system and 3% from the appendix [6]. Krukenberg tumors are usually bilateral. Ovarian tumor may cause complications such as torsion, rupture during pregnancy and also spontaneous miscarriage and preterm labor. The most common complication of ovarian tumors during pregnancy is uterine torsion, and most of the torsions occur either during 8-16 weeks of gestation or during the involution of the uterus in the puerperal period. In this case report, we looked into the case of a patient with gastric carcinoma who was Krukenberg tumor diagnosed with ovarian torsion mass at 16th gestational week.
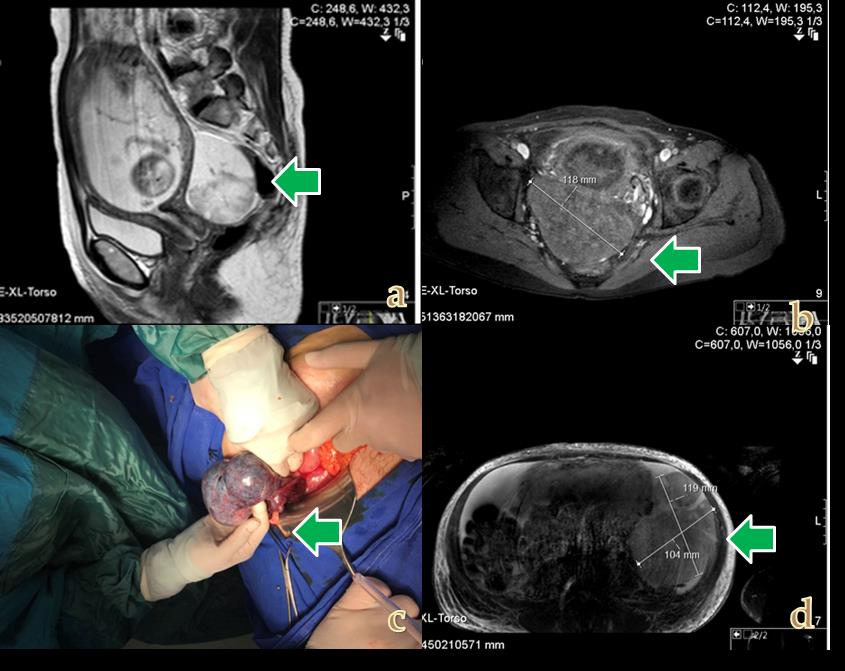
A 36-year-old patient, gravida 4, parity 3, and 16th gestational week was referred to our clinic with sudden onset of abdominal pain. In her past medical history, she reported that for the last two months she was suffering from occasional abdominal pain with nausea and intermittent vomiting. She did not have neither a family history of a chronic disease nor a history of substance use, smoking or alcohol use. The patient has not had any previous surgical operation and the patient's vital signs were stable. The ultrasonographic examination revealed that fetal heart rate was positive and inuterine pregnancy was observed. In the right adnexal region approximately 11x10 cm heterogeneous ovarian mass was detected, while the left ovary was in normal size. In the doppler ultrasound, no blood build up was observed on the right ovary. The patient was hospitalized. In the advanced MRI examination, adnexal mass of approximately 11x8 cm, sourced from the right adnexal region, was detected and there was minimal free fluid in the abdomen (Figure 1). On physical examination, there were defenses and rebounds in the abdomen and other system examinations were normal. Lab test showed the following results; In the complete blood count (CBC), hemoglobin: 10.9 g / dl, platelet count: 247.000 mm3, wbc 17.000 and complete urinalysis were normal.
Surgical intervention was planned due to ovarian torsion mass. In the evaluation of the patient during operation, the uterus size was of 16 weeks gestation and on the right ovarian, 11-centimeter size torsion mass was observed (Figure 1). The left ovary and tube were normal in appearance. Right salpingectomy was performed. In the postoperative follow-up of the patient, since there wasnt any problem, the patient was discharged. Pathological result could not be assessed clearly due to necrotic tissues but poorly differentiated Sertoli-Leydig Cell Tumour (SLCT) was considered. On the 40th post-operative (post-op) day, the patient was readmitted to the hospital with acute abdominal pain, in poor general condition and nausea-vomiting. The patient was hospitalized and had epigastric pain and dyspeptic complaints.
Ultrasonographic examination revealed a heterogeneous mass of 10 X 9 cm on the left ovary compatible with 23 weeks of gestation and widespread acidity in the stomach. Magnetic resonance imaging (MRI) showed widespread acid in abodmen, 12 x 10 cm solid cystic mass lesion on the left ovarian and mesenteric edema. (Figure 1). In laboratory tests, CA125: 394, CA19- 9: 9354, AFP: 90. After of gynecologic oncology and perinatology evaluation, to the patient who was in poor general condition and had nutritional problems, cesarean was planned at 28 weeks of gestation due to the development of advanced Intrauterine growth restriction (IUGR). In the abdominal observation of the patient, widespread implants were observed. Uterus was of normal appearance, left ovary size increased; approximately 20 cm in size and there were masses with multiple heterogeneous solid cystic areas. After caesarean section (c-section), 763 gr 7-8 APGAR baby girl was delivered. The patient underwent left salphingoopherectomy and was sent for frozen-section pathologic evaluation. Pathology report of frozen indicated signet ring cell adenocarcinoma metastasis in the left ovaries. An omentectomy was performed to the patient with prominent omental cake appearance.
Excisional biopsy was obtained from a 3 cm mass in the stomach. Biopsies were obtained from right ovary and implants on the sigmoid colon. Then the operation was terminated. On postoperative day 3, postoperative pain and dyspnea were present; computed tomography (CT) revealed gallbladder in hydropic appearance, bilateral pleural effusion and bilateral diffuse parenchymal lung septation. The T1 vertebrae was consistent with heterogeneous metastasis. ERCP was performed on sixth postoperative day. In the evaluation, amorphous mass was observed in the neighborhood of the pancreas bud. The patient was then transferred to the oncology department. Histopathology revealed tumor metastatic involving high-grade and poorly differentiated signet ring cell areas in the left ovary, excisional biopsies obtained from the sigmoid colon showed infiltration of adenocarcinoma, omental adenocarcinoma infiltration; adenocarcinoma infiltration was observed as a result of excisional biopsies taken from right ovarian region and sigmoid colon. The patient died in the oncology service, postoperative day (POD) 90.
Discussion
Krukenberg tumor (KT) during pregnancy is extremely rare and its incidence is 0.4-0.5%. Due to the physiological changes in pregnancy, the diagnosis of cancer may be delayed. Patients complaining of persistent epigastric complaints in the second Trimester of pregnancy, especially accompanied with weight loss and hemoptysis, Endoscopy and gastric biopsy should be recommended [7].
Elevated sex hormones in pregnancy may lead to the development of gastric cancer by triggering underlying precancerous lesions. The placental growth factor (PlGF), which is found more in the gastric cancer (GC) tissue than the vascular growth factor, is thought to be correlated with serosal invasion, lymph node metastases, tumor stage and patient survival rates [7] .
A systemic review was conducted [8] in 100 patients with Krukenberg tumor, live birth rate was (81.8%); 75.8% of them were delivered by cesarean section and in half of these patients (54.3%), cytoreductive surgery was performed at the third trimester. In %45.7 of these patients, ascites (45.7%), carcinomatosis (25.7%) and non-ovarian distant metastases (14.3%) were found at the time of surgery. In 12 cases; optimal tumor surgery was performed for primary cancer and ovarian cancer. 57.1% of the patients received chemotherapy during the postpartum period. In 20% of cases, primary cancer was diagnosed and treated before pregnancy; during the pregnancy, ovarian metastasis was diagnosed approximately 11 months after the diagnosis of primary cancer. Early diagnosis and close follow-up affect the results positively; but reported median overall survival is six months.
There is no standard opinion regarding maternal and fetal risks related to the optimal treatment of ovarian tumor [8]. Tumor treatment may vary depending on gestational age, patient's request, primary tumor and cancer's stage. Debulking surgery; Partial or total gastrectomy, lymph node dissection and bilateral oophorectomy with platinum based chemotherapy can be performed safely in early weeks of pregnancy. However if the diagnosis is made during the third trimester of pregnancy, the caesarean section must be done to deliver the fetus followed by chemotherapy and surgical resection [9, 10].
Conclusion
In conclusion, in this case presenting with ovarian torsion mass, since the dyspeptic complaints were not clear and necrosis, the patient could not be diagnosed. In the following period; the patient presented with general poor health, stomach pain and common abdominal pain from ovarian cyst. However, in this period, the patient presented as advanced gastric cancer. Krukenberg tumour should always be kept in mind in patients diagnosed with ovarian torsion mass and a multidisciplinary approach should be taken in the evaluation of patient. With the maternal and fetal optimal timing, termination of pregnancy and treatment of primary tumor are important.
References
-
Peccatori FA, Azim HA, Orecchia R, Hoekstra HJ, Pavlidis N, et al. (2013) ESMO Guidelines Working Group, Cancer, pregnancy and fertility: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol 24(6): 160-170.
-
Gezginç K, Karataylı R, Yazıcı F, Acar A, Celik C, et al. (2011) Ovarian cancer during pregnancy, J Gynaecol Obstet 115(2): 140-143.
-
Kwon YS, Mok JE, Lim KT, Lee IH, Kim TJ, et al. (2010) Ovarian cancer during pregnancy: clinical and pregnancy outcome. J Kor Med Sci 25(2): 230-234.
-
Katz L, Levy A, Wiznitzer A, Sheiner E (2010) Pregnancy outcome of patients with dermoid and other benign ovarian cysts. Arch Gynecol Obstet 281(5): 811-815.
-
Dueñas-García OF, Diaz-Sotomayor M, Chanana C (2011) Bilateral ovarian krukenberg tumor in a full- term pregnancy. ISRN Obstet Gynecol 620380.
-
Tan KL, Tan WS, Lim JF, Eu KW (2010) Krukenberg tumors of colorectal origin: a dismal outcome– experience of a tertiary center. Int J Colorectal Dis 25(2): 233-238.
-
Burgazli KM, Mericliler M, Kavukcu E, Erdogan A, Ertan AK (2013) Discovery of asymptomatic Krukenberg tumors diagnosed during caesarean section: therapy with hyperthermic intraperitoneal chemotherapy. Postgrad Med 125(4): 87-90.
-
Kodama M, Moeini A, Machida H, Blake EA, Grubbs BH, et al. (2016) Feto-maternal outcomes of pregnancy complicated by Krukenberg tumor: a systematic review of literature. Arch Gynecol Obstet 294 (3): 589-598.
-
Mahfoud T, Elhassani ME, Hafidi MR, Babahabib MA, Tanz R, et al. (2012) Krukenberg tumor secondary to gastric carcinoma in a pregnant woman: A case report and literature review. Biol Biomed Rep 2: 32-36
-
Glisic A, Atanackovic J (2006) Krukenberg tumor in pregnancy. The lethal outcome. Pathol Oncol Res 12(2): 108-110.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey