Intestinal Malrotation in Adulthood with Non-Ischemic Midgut Volvulus: A Case Report
Background: Congenital intestinal malrotation diagnosed in adulthood is rare, hence is more often an incidental diagnosis. We report in our paper a case of young adult with chronic small gut malposition complicated with midgut volvulus without arterial compromise. Methods: We report the case of a 22-years old female with no past history admitted for chronic sub-occlusive syndrome and portal hypertension. Physical examination assessed a mild abdominal distension with ascites and a BMI of 16 kg /m2. Endoscopic exploration was non-specific. Abdominal entero-CT scan confirmed jejunal malposition with mesenteric hyperemia and parietal venous stasis. Further exploration confirmed malabsorptive disorders and malnutrition. Decision was made favoring coelioscopic evaluation first. We converted to laparotomy for extended exploration and appropriate management. We carried on adhesiolysis of the jejunum, retrograde bowel emptying, small bowel unfolding and finally fixation of the last jejunal loop with its mesenteric root. Post-operative evolution was uneventful. Discussion: Congenital intestinal malrotation is considered a spectrum of rotational anomalies; as such it holds a high clinical multigenicity. Moreover considering difficulty of diagnosis, high number of subtypes, and consequent possible complications, there is no standard of care regarding treatment of intestinal malrotation. We carried laparoscopic exploration followed by laparotomy un-conventional Ladd’s surgery. Finally, our case report manifests the possible repercussions of delayed treatment such as severe malnutrition. Conclusion: Small bowel malrotation carry a significant risk of complication, including midgut rotation. Our paper shows downfalls of chronic midgut volvulus that are essentially malabsorptive complications, associated with serious decline of quality of life. Therefore surgical treatment is both inevitable and effective.
Introduction
Congenital Intestinal malrotation is a complex gastrointestinal disorder resulting from the lack of fetal intestinal physiological rotation [1]. Congenital malrotation can be considered either typical or atypical based on the position of the ligament of Treitz compared to midline [2]. Dott first described congenital intestinal malrotation in 1923
among other developmental and anatomical variations [1]. Since then, intestinal malrotation has been reported to be commonly an incidental diagnosis in adults as a result to the nonspecificity of its clinical presentation. Unfortunately, the incidence of congenital intestinal malrotation has still not been defined with specificity neither updated, and is estimated to 0.0001% and 0.19 % in adulthood [3, 4]. Furthermore intestinal malrotation diagnosed in adulthood is rare [1, 5]. Consequent to the non-specificity of the symptoms, complications can subside. Among the most severe complications of intestinal malrotation is midgut volvulus. Midgut volvulus is the twisting of small intestine around its own mesenteric root, with or without compromising of the small bowel blood flow [6]. Though the risk of vascular compromise is significant. Intestinal ischemia is associated with high morbidity and mortality, and is therefore considered an emergency necessitating prompt operative intervention [7]. Moreover adult’s midgut volvulus is a rare surgical disease [6]. Hereby we report in our paper a rare case of young adult with chronic small gut malposition complicated with midgut volvulus with vascular compromise, and significant quality of life decline.
Clinical Case
A 22-year-old female patient, presented to our medical unit for evolving Koenig’s like syndrome over 6 months, associated with episodes of hematochezia, diarrhea, and non-specific abdominal pain. Past medical history included amenorrhea evolving over a year. The patient reported taking no alcohol, smoke or ellicit drugs. No past surgical history was noted. No weight loss was assessed. Abdominal examination confirmed a mild abdominal distension with ascites. BMI was 16 kg /m2. The patient underwent both ileo-colonoscopy and upper gastrointestinal endoscopy that were non-conclusive with negative intestinal biopsy for celiac disease. Abdominal entero-CT scan showed jejunal malposition with presence of a swirl like images at the right flank with a dilated portal vein associated with collateral mesenteric venous circulation and tortuous dilated superior mesenteric vein of 18 mm (Figure 1).
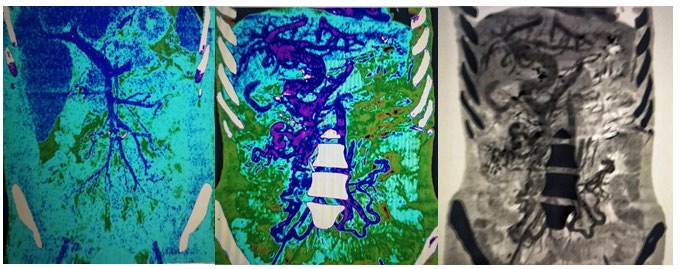
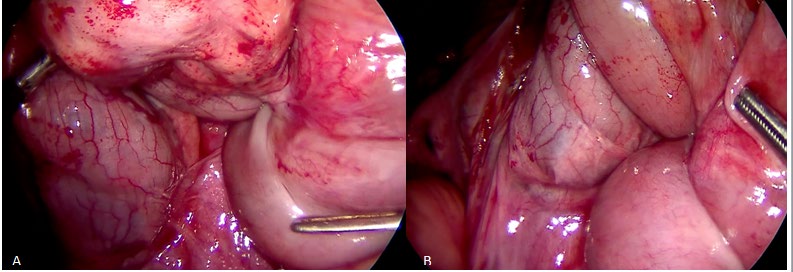
Portal vein had a diameter of 15 mm with anatomical variant giving three branches; two remained permeable. Abdominal CT-scan demonstrated as well mesenteric hyperemia with edematous infiltration of pelvic intestinal wall, intraperitoneal effusion and signs of portal hypertension with parietal venous stasis. Laboratory findings revealed a marked malabsorption syndrome with hypoalbuminemia and severe hypovitaminosis. Decision was made favoring laparoscopic evaluation first. Abdominal cavity exploration showed intestinal dilation upon unidentified obstacle of the ileum that seemed to be buried under a fixed intestinal bridle at first. We converted to laparotomy for extended exploration. On laparotomy exploration found adhesions between the first and the last loop of small bowel (Figure 2). Significant dilation of jejunum compared to ileum was observed. As well as absence of fixation of the root of the ileal mesentery was noticed. We carried on adhesiolysis of the jejunum, retrograde bowel emptying, small bowel unfolding and finally fixation of the last jejunal loop with its mesenteric root. No appendectomy was done. Post-operative evolution was uneventful. The patient was discharged of day 5. Short- term evaluation one month later the patient reported absence of symptoms with weight gain.
Discussion
Intestinal malrotation is characterized by faulty fixation of the midgut and its mesentery to the posterior abdominal wall. It is usually encountered in infants and children. The most serious complication of malrotation is volvulus. Around 80% of midgut volvulus cases present during the first month of life [2]. To our best of knowledge only few cases have been reported during adulthood similarly to our patient [8, 9, 10]. A simple and reasonable way of classifying intestinal anomalies of rotation and fixation would be as non-rotation, malrotation (incomplete rotation), and reversed rotation [11, 12]. The physiopathologic mechanisms underlying this spectrum basically encompass the timing of return of the midgut into the peritoneal cavity after certain degrees of rotation during intrauterine developmental stages; less than the normally expected 270° counterclockwise. Other congenital anomalies causing incomplete bowel occlusion usually have delayed clinical onset later in life [11]. And often need radiological exploration for diagnosis like barium enema studies, ultrasonography, computed tomography, and magnetic resonance imaging (MRI) [11]. The “whirl sign”, as seen on abdomino-pelvic CT examinations, refers to a whirling or spiral shape of the mesenteric vessels, which may or may not accompany the intestinal loops and their supplying vessels. Sensitivity of abdomino-pelvic CT scan to detecting intestinal malrotation is high, and its specificity with regard to symptomatic volvulus increases when accompanied with whirling of both bowel and vessels [13].
Ladd’s procedure was first described in 1941 to treat symptomatic bowel movements. This procedure remains the standard treatment regardless of the type of symptomatic malrotation involved. The general principle is a repositioning of the intestine in “complete common mesentery” at 90°, corresponding to the initial stage of the rotation of the primitive intestinal loop during embryonic life [14]. Indeed, it is unreasonable to aim at repositioning the intestine in normal anatomical position in case of total malrotation, since it can be the source of its own morbidity due to bridles or internal hernias. It is recommended, though not mandatory, to complete Ladd procedure with appendectomy. In fact it is a described practice essentially in a preventive scope in case of acute appendicitis with delayed diagnosis due to atypical positioning [14]. We decided to undergo laparoscopic exploration and quickly converted to laparotomy due to the high risk of perforation with excessive laparoscopic forceps manipulation of dilated bowel.
Considering difficulty of diagnosis, high number of subtypes, and consequent possible complications, there is no standard of care regarding treatment of intestinal malrotation. Such high multigenicity exists because the congenital intestinal malrotation is not a single congenital entity, but rather is a spectrum of rotational anomalies [15]. Classily, treatment protocol for intestinal malrotation is still unclear. In one hand it is highly controversial to operate on an asymptomatic intestinal malrotation [16]. Some authors state the benefice of early surgical intervention in order to prevent more serious latter complications, and reduce morbidity and mortality [17]. In fact, our case report manifests the possible repercussions of delayed treatment including serious quality of life decline, and severe malnutrition that can occur during a key period of developmental milestone. While elective Ladd’s procedure is reserved for clinically non-urgent symptomatic cases, laparoscopic approach is preached in this matter. Indeed, laparoscopy is an excellent mean of evaluation and treatment of chronic symptomatic intestinal malrotation without midgut volvulus [18]. In the other hand emergent laparotomy is still the standard approach for emergency cases.
Conclusion
The jejunal malposition is a congenital malformation, which clinically manifested in our patient only at the age of 22 years. Small bowel malrotation carry a significant risk of complication, including midgut rotation. Chronic non- ischemic midgut volvulus lead to malabsorptive downfalls, associated with serious decline of quality of life. Therefore surgical treatment is both inevitable and effective.
Bullet Points
- Congenital intestinal malposition is a congenital malformation with non-specific symptoms, with therefore possible delayed clinical diagnosis and consequent complications.
- Small bowel malrotation carry a significant risk of complication, including midgut volvulus.
- Surgical treatment is both inevitable and effective; early surgical intervention may prevent more serious latter complications, and reduce morbidity and mortality
- Both open and laparoscopic approaches are suitable for treating congenital intestinal malrotation that can require a dynamic choice and adaptation to the situation.
References
-
Sipahi M, Caglayan K, Arslan E, Erkoc MF, Aytekin FO (2014) Intestinal Malrotation: a rare cause of small intestinal obstruction. Case Rep Surg 2014: 1-4.
-
Ayane GN, Kadimo K (2018) Diagnosis and surgical management of congenital intestinal malrotation presenting with midgut volvulus in an adult: high index of suspicion (case report). Pan Afr Med J 29: 154.
-
Von Flue M, Herzog U, Ackermann C (1994) Acute and chronic presentation of intestinal nonrotation in adult. Dis Colon Rectum 37: 192-198.
-
Wang C, Welch C (1963) Anomalies of intestinal rotation in adolescents and adults. Surgery 54: 839-855.
-
Haak BW, Bodewitz ST, Kuijper CF, de Widt-Levert LM (2014) Intestinal malrotation and volvulus in adult life. Int J Surg Case Rep 5(5): 259-261.
-
Nicholson O, El Khairi SM, Schreiber H (1992) Primary midgut volvulus in the adult: two case reports. Am J Gastroenterol 87(3): 395-398.
-
Oldenburg WA, Lau LL, Rodenberg TJ, Edmonds HJ, Burger CD (2004) Acute Mesenteric Ischemia: A Clinical Review. Arch Intern Med 164(10): 1054-1062.
-
Papadimitriou G, Marinis A, Papakonstantino A (2011) Primary midgut volvulus in adults: report of two cases and review of the literature. J Gastrointest Surg 15: 1889-1892.
-
Bozlar U, Ugurel MS, Ustunsoz B, Unsal C (2008) CT angiographic demonstration of a mesenteric vessel “Whirlpool” in intestinal malrotation and midgut volvulus: A Case Report. Korean J Radiol 9(5): 466-469.
-
Söker G, Yılmaz C, Karateke F, Gülek B (2014) An unexpected cause of small bowel obstruction in an adult patient: midgut volvulus. BMJ Case Rep.
-
Berrocal T, Lamas M, Gutieerrez J, Torres I, Prieto C, et al. (1999) Congenital anomalies of the small intestine, colon, and rectum. Radiographics 19(5): 1219-1236.
-
Long FR, Kramer SS, Markowitz RI, Taylor GE (1996) Radiographic patterns of intestinal malrotation in children. Radiographics 16(3): 547-556.
-
Gollub MJ, Yoon S, Smith LM, Moskowitz CS (2006) Does the CT whirl sign really predict small bowel volvulus?: Experience in an oncologic population?. J Comput Assist Tomogr 30(1): 25-23.
-
Tan V, Kotobi H, Parc Y (2017) Technique chirurgicale: la procédure de Ladd pour volvulus total du grêle sur malrotationLadd procedure for malrotation with total intestinal volvulus. Journal de chirurgie viscérale 154(3).
-
Kapfer S, Rappold J (2004) Intestinal malrotation not just the pediatric surgeon’s problem. J Am Coll Surg 199(4): 628-635.
-
Hmadeh H, Saliba C, Raka M, et al. (2018) An Unusual Case of Intestinal Malrotation Causing Duodenal Obstruction by a Looped Appendix. Am J Case Rep 19: 1362-1365.
-
Prasil P, Flageole H, Shaw K, Nguyen LT, Youssef S, et al. (2000) Should malrotation in children be treated differently according to age?. J Pediatr Surg 35(5): 756- 758.
-
Mazziotti MV, Strasberg SM, Langer JC (1997) Intestinal rotation abnormalities without volvulus: the role of laparoscopy. J Am Coll Surg 185(2): 172-176.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey