Neutrophil CD177 Flow Cytometric Expression as a Potential Myeloid Marker
Introduction: A specific clonality marker, may enhance diagnosis of myeloid neoplasms, particularly in challenging cases. Neutrophil CD177, being exclusive to the granulocytic series, could represent a good potential marker. Our aim in this study was to explore this assumption. Methods: 213 subjects with benign and neoplastic’ myeloid disorders were included in this study. Peripheral blood neutrophils were analyzed by flow cytometry (FC) for CD177+% and mean fluorescent intensity (MFI). Results: CD177 showed 2 expression patterns; single& bimodal. Neutrophil CD177+ MFI was significantly higher in Phnegative c-MPNs (2.9-37.4; median 14.1), compared to controls (0.8-20.5; median 8.8). No significant difference in either CD177% or MFI was observed between Polycythemia Vera (PV) and Essential Thrombocythemia (ET) groups. The PV group showed a significantly higher, CD177 MFI compared to SE and control groups (4.8-37.4; median 16.5, 1.58-25.7; median 5.81, 0.85-20.5; median 8.8 respectively). Similarly, the ET group had a significantly higher CD177+ MFI compared to controls (2.9- 34.5; median 13.4 versus 0.85-20.5; median 8.8 respectively). No significant difference in CD177+ neutrophil % or MFI was observed in MDS patients compared to controls. No significant correlation was detected between CD177+% and MIF, nor with the JAK2 V617F allele burden in JAK-2+ cases. A high specificity of CD177 MFI was only observed in; Ph-negative c-MPNs (93%) & in differentiating PV from SE (85%); at a cutoff, of 20 p.d.u. Conclusion: The CD177 expression is suggested as a good potential marker in Ph-negative MPNs, particularly in differentiatingPV and secondary erythrocytosis.
Introduction
The CD177 is a member of the human Ly-6 gene superfamily which encodes glycosyl-phosphatidylinositol (GPI) anchored glycoproteins and has 70 to 100 amino acids conserved domains. It is encoded by a polymorphic gene with two alleles: PRV-1 and NB1, with the former as the most prevalent [1]. The NB1 gene is expressed by a subpopulation of neutrophils and carries Human Neutrophil Antigen (HNA)-2a [2]. Although its function is not fully understood, it has been demonstrated to facilitate neutrophil endothelial transmigration [3, 4, 5]. The CD177 shows a peculiar distribution pattern on neutrophils, with ∼95% of healthy individuals producing CD177+ neutrophils, and 5% are CD177 deficient [6]. Individuals show a stable CD177 pattern over time, with distinct membrane CD177- and CD177+ neutrophil subsets. The percentage and expression level of CD177 increase with granulocyte maturation from CD11b+CD16– to CD11b+CD16+ cells [7].
Increased expression of CD177 with reported in many disorders that increased neutrophil production or release. A significant increase was particularly realized in c-MPNs and its use as a potential clonal marker in these disorders has been suggested by many researchers, using different methods of expression analysis. These studies were particularly intriguing since there is no established myeloid marker that can be clinically applied in these disorders which constitutes a critical diagnostic gap. Our aim in this study, therefore, was to explore the potential of neutrophil CD177 expression as a diagnostic marker in myeloid disorders.
Materials and Methods
Subjects
A total of 213 cases, diagnosed at Kasr Al-Aini Hospitals, Cairo University during the period December 2014 through January2016, were included. They comprised 3 main myeloid disorders groups; benign neutrophilia, SE, and clonal myeloid neoplasms, as well as a hematologically-normal group as a control. Patients on G-CSF, Interferon or hypomethylating drugs, or in the first 3 months of Hydroxyurea treatment; and patients with MDS and a PNH clone; were excluded.
Methods
For each patient relevant clinic-pathological data were anonymously obtained from patients’ records, excluding all identifying data. Data included age, gender, final diagnosis, directly relevant diagnostic investigations e.g. BCR-ABL1 & JAK-2 etc.
During routine follow up patients visits, an extra 2 ml EDTA-anti-coagulated whole blood samples were obtained in coded -deidentified vacutainers, after obtaining the patient consent. Samples were used for FC analysis of CD177 neutrophil expression. A minimum of 10,000 events were counted for each specimen. Neutrophils were gated according to size (forward scatter, FSC) and complexity (side scatter, SSC). Negative control samples were used. FACS Data analysis was performed using CXP flow analysis software. CD177-positive and CD177-negative populations were obtained by placing the cutoff cursor at the value between the positive and negative peaks. For samples with 2 positive peaks, both peaks were included in the positive population.
Statistical analysis was carried out using SPSS (Statistical Package for the Social Science; SPSS Inc., Chicago, IL, USA).
Results
The distribution of pathological entities included in the study is shown in figure 1.
Among the clonal MPNs neoplasms of 93 patients; 30 had PV, 20 had ET, 2 had PMF, 20 had BCR-ABL 1positive CML, 15 had MDS, 5 had MDS/MPNs, and one had acute myeloid leukemia (AML) on top of refractory cytopenia with multilineage dysplasia (RCMD).
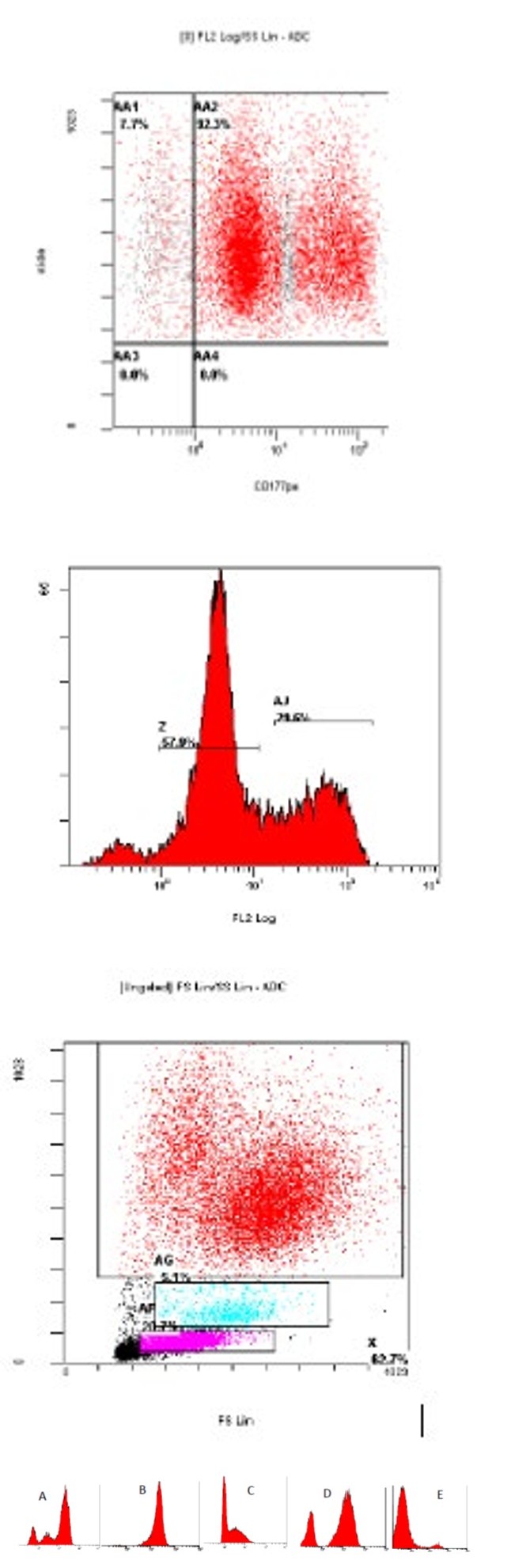
The interpretation and expression patterns of CD177on peripheral blood neutrophils, by flow cytometry are demonstrated in figure 2 a and b, respectively. Three patterns are recognized; dim, bright or both (bimodal pattern), but none was exclusive to a certain pathologic entity. A single positive peak is seen in 88.5 % of cases (207/213) and double positive peaks were seen in 11.5 % of cases (27/213).
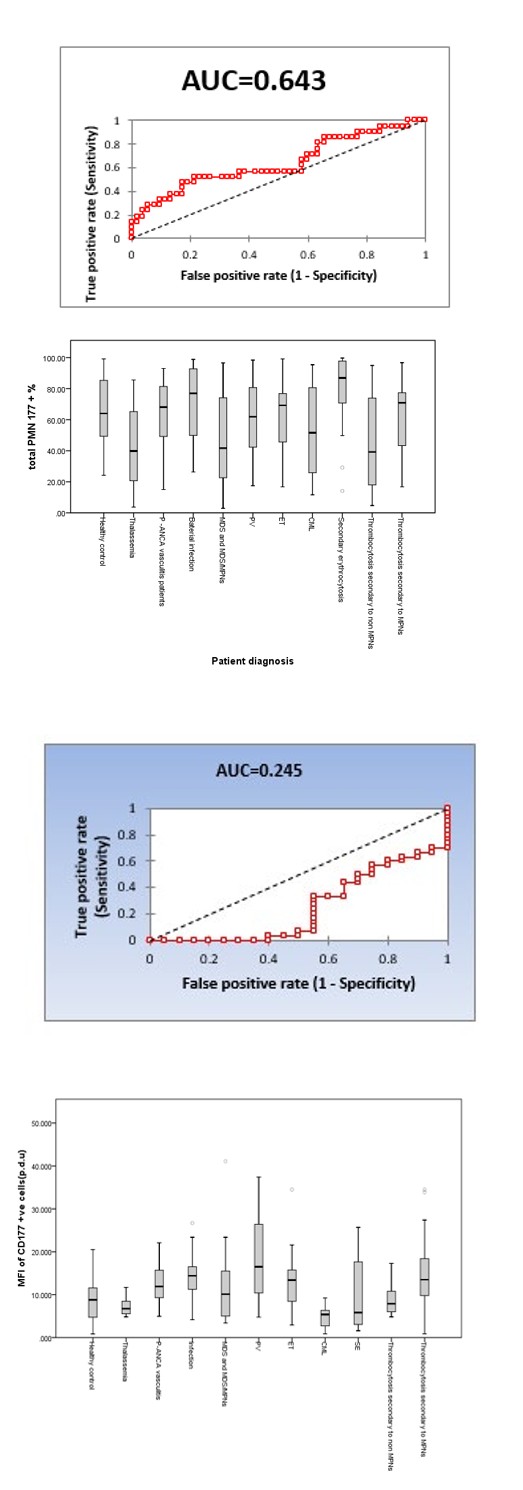
Figure 2A: Box blot of median, 25th and 75th quarter in regards to CD177 +ve cells % in different study groups, Abbreviation PMNs polymorphonuclear cells, P-ANCA perinuclear anti neutrophil cytoplasmic antibody , MDS myelodysplastic syndrome, MPNs myeloproliferative neoplasms, PV polycythemia vera, ET essential thrombocytosis ,CML chronic myelogenous leukemia.
Figure 2B: Box blot of median, 25th and 75th quarter in regards to CD177 +ve cells MFI in different study groups, Abbreviation MFI mean florescent intensity measured in procedure defined unit (p.d.u), P-ANCA perinuclear anti neutrophil cytoplasmic antibody , MDS myelodysplastic syndrome, MPNs myeloproliferative neoplasms, PV polycythemia vera, ET essential thrombocytosis ,CML chronic myelogenous leukemia.
The comparison of CD177 expression’ MFI and % of the studied groups is diagrammatically represented in figure 3’ box plots. The correlation of CD177 MFI, CD177+ve cells %, and the absolute neutrophilic count was not significant for any of the studied groups. For JAK-2 positive PV (30) and ET (20) cases, no correlation was detected between allele burden and CD177 + neutrophils % (r0.135, p=0.475, and r=0.126, p value =0.596, respectively).
Figure 3A: Receiver Operating Characteristic (ROC) curve showing that the area under the curve of CD177 +ve cells % as test in diagnosis of MDS and MDS/MPNs versus Philadelphia negative myeloproliferative neoplasm group was 0.643 with a p value of p=0.05. P value < 0.05 is considered statistically significant difference, P value < 0.01 is considered high statistically significant difference. AUC >0.6 is considered a fair test, AUC >0.7 is considered a good test, AUC >0.8 is considered a very good test, AUC >0.9 is considered an excellent test.
Figure 3B: Receiver Operating Characteristic (ROC) curve showing the area under the curve (AUC= 0.245 ) of using mean florescent intensity (MFI) of CD177 +ve cells as test in diagnosis of Polycythemia Vera (PV) versus Secondary Erythrocytosis(SE) (p value 0.0002) ,P value < 0.05 is considered statistical significant difference, AUC >0.6 is considered a fair test, AUC >0.7 is considered a good test, AUC >0.8 is considered a very good test, AUC >0.9 is considered an excellent test.
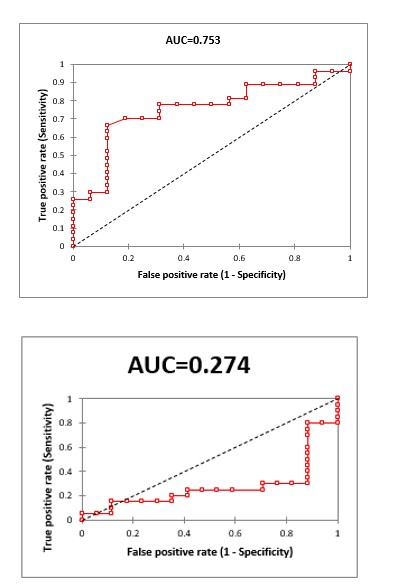
Figure 3C: Receiver Operating Characteristic (ROC ) curve showing the area under the curve of using CD177 mean florescent intensity (MFI) as test in diagnosis of thrombocytosis secondary to MPNs and non MPNs causes (AUC=0.753 ) with a p value of 0.0004, P value < 0.05 is considered statistical significant difference, AUC >0.6 is considered a fair test, AUC >0.7 is considered a good test, AUC >0.8 is considered a very good test, AUC >0.9 is considered an excellent test.
Figure 3D: Receiver Operating Characteristic (ROC ) curve showing the area under the curve of using CD177 MFI as test in diagnosis of Essential thrombocytosis and secondary thrombocytosis group (AUC=0.274 )with a p value of 0.007, P value < 0.05 is considered statistical significant difference, AUC >0.6 is considered a fair test, AUC >0.7 is considered a good test, AUC >0.8 is considered a very good test, AUC >0.9 is considered an excellent test.
The sensitivity and specificity of CD177 expression as a discriminating diagnostic test between the different studied groups is represented by the receiver operating characteristic (ROC) curves in figure 4. A summary of the sensitivity and specificity of CD177 expression at different cut-off values is given in table 1. The CD177 MIF showed an AUC=0.274 (p-value 0.007), between ET and secondary thrombocytosis groups, which is considered. The CD177+ neutrophil % showed an AUC=0.643 (p=0.05) in discriminating “MDS and MDS/MPNs” from “Ph-negative MPNs”, which is considered “fair”, and of 0.731(p< 0.002) in discriminating PV versus SE, which is considered a “good test”.
Discussion
The CD177 expression is an exclusive and stable neutrophil membrane glycoprotein which is elevated in many conditions associated with their increased production or release. Its significant elevation in c-MPNs triggered many investigators to assess its potential use as a clinical diagnostic marker in these disorders. These studies were particularly intriguing since there is no reliable clonal myeloid marker for these disorders, which constitutes a critical diagnostic gap.
To explore this potential, a total of 213 subjects diagnosed with benign and neoplastic myeloid disorders were studied for peripheral blood neutrophil expression of CD177 using flow cytometry. In this study, 3 patterns of CD177 MFI expression were recognized: dim, bright or both (bimodal pattern). None of these patterns was exclusive to a certain disease entity. As to CD177+ %, a single positive peak was seen in 88.5% of cases (207/213), while a 2-peaks pattern was observed in 11.5% of cases (27/213).
The heterogeneous pattern of neutrophil CD177 expression was similarly reported in most studies, both in healthy individuals and in myeloid disorders. A small proportion of healthy individuals lack this antigen (CD177 null), with increased susceptibility to the development of anti-neutrophil antibodies [2].
Although the mechanism of this heterogeneousness, isn’t fully understood, recent studies have explored a variety of prospects. Wu et al, identified 3 leucocyte populations among their study cohort: negative (neg), intermediate (int) and high (hi) with the bulk of people having a bi-modal pattern, whereas some people having >20% of neutrophils expressing CD177 at intermediate levels. In their sequencing study, they identified a stop sequence arising from one base substitution in base seven, as being responsible for the CD177 null phenotype. In this variant, base seven is provided entirely by CD177 Pseudogene (CD177P1); a sequence homolog of CD177 exons 4–9 on the minus strand; through allelomorphic conversion and is transmitted through the germline. It is thus a heritable attribute which determines the individual phenotype by the quantitative relation of CD177/CD177P1 alleles. This phenomenon explains the distinctive CD177 transcription into CD177neg and CD177hi neutrophils among individuals [6].
EulenbergGustavus, et al. studied the mechanisms of subset restricted CD177 expression in bimodal people and incontestible that solely CD177pos, neutrophils, might manufacture CD177 macromolecule and messenger RNA. Using haplotype analysis, they could identify a novel monoallelic CD177 expression pattern, that doesn’t follow classical random monoallelic expression or learning. During this pattern, either the maternal or paternal allelomorph are stably transcribed, whereas the opposite copy is silenced throughout leucocyte differentiation, by tightly regulated silencing mechanism. The incidence of two CD177positive peaks, is another development discovered, with nevertheless not fully understood molecular basis. The Ph-negative c-MPNs represent the bulk of myeloid disorders cases (52/93) in this study, with PV (30 cases) and ET (20 cases) comprising the most entities. The BCR-ABL1-positive CML cases were next in frequency (20 cases) [7].
The CD177 expression results for the full Ph-negative c-MPNs group disclosed considerably higher MFI, however no difference in CD177 leucocyte positivity%; compared to controls. Similar results for the MFI and CD177 leucocyte positivity%; were detected within the ET sub-group. While, the PV subgroup, didn’t show a major distinction in CD177 expression (% and MFI) from the ET cases. However, they showed considerably higher CD177 MFI values compared to SE and controls. While the CD177+ neutrophil % for the Ph- negative c-MPNs in this study were in agreement with those reported by Slezak, et al. and Meyerson, et al. our CD177 MFI results were contradictory [8, 9]. The case variety and blend in several studies might cut back the accuracy of comparisons. In Meyerson et al. study as an example, the management cluster enclosed some patients with reactive conditions such as autoimmune disorders; that could increase the CD177 expression compared to the hematologically-normal subjects.
In examining PV and ET groups, our results agreed with those of Cilloni, et al. and of Passamonti, et al. whereas they were contradictory to those obtained by others [9, 10, 11, 12, 13]. In the latter study, considerably higher expression levels of CD177 were reported in PV compared to ET groups. Variations in the study population, patient inclusion criteria, and type and length of therapy might partly justify the inconsistent results.
The significant elevation of CD177 expression in PV patients within the current study compared to cases with SE, was comparable to those in several previous studies [10, 11, 12, 14, 15, 16, 17]. Bock, et al. however, using relative quantitation of CD177 factor, reported contradictory results, but the two techniques may not be accurately comparable [18].
Fifty patients in this study were JAK2 positive: thirty with PV and twenty with ET diagnoses. In these patients, no significant correlation was detected between CD177 expression levels and the JAK2 V617F allelic burden. This would possibly imply that overexpression of CD177 may not be a consequence of JAK2V617F activation. The present results were in step with those according to Rapado, et al. [19]. However, they contradict alternative studies that detected a robust correlation between CD177 expression and JAK2 V617F allelic burden [20, 21, 22, 23, 24]. However, these studies didn’t ensure a causative relation, but rather the two markers are associated with the same disorder. Tefferi, et al. hypothesized that CD177 overexpression was caused by the STAT hyperactivation [21]. The authors suggested a correlation between the 2 markers i.e. an associate allelic dose-dependent result of JAK2V617F on white corpuscle PRV- 1 expression; both show a considerably higher prevalence in PV and post polycythemic myeloid metaplasia [16, 25, 26, 27, 28].
Accordingly, the JAK2V617F-associated increase in PRV- 1 would possibly represent a recapitulation of cytokine- associated leucocyte activation that is mediated through the JAK-signal transcription pathway [29]. Furthermore, a recent study by Shahrabi, et al. recommended a prognostic value for variations within the expression of CD177 in MPNs. The overexpression of this marker in JAK2V617F positive MPNs might be a poor prognostic issue related to the presence of microorganism infection. The authors hypothesized that flow cytometric immunophenotyping could also help assess the prognosis of inflammatory and immune complications in MPNs [30].
Fifteen MDS cases were enrolled in our study and showed no vital distinction in each CD177 expression parameter (MFI and % positivity) compared to other groups. Some studies have reported similar results [ 18,31]. Others reported significantly different results in their MDS group [9]. Meyerson, et al. reported a significant association of skewed low neutrophil CD177(%) with clonal myeloid disorders, particularly myelodysplasia, and suggested its use for diagnosis in these disorders. They explained this association on the same principle as the skewing of k and L light chain ratio for determining clonal B cells based on the expression of a single immunoglobulin type as a result of allelic exclusion and its maintenance on tumor cells. Though the reason for the association of low neutrophil CD177(%) with MDS and CMML is not fully understandable, the authors explained its possible relation to asynchronous or abnormal expression in dysgranulopoiesis maturation. The low neutrophil CD177(%) in their study however, had a limited sensitivity for detecting MDS with only half of their patients demonstrating a neutrophil CD17 7(%) below 40% [9].
In the current study, the sensitivity and specificity of CD177 MFI in Ph-negative c-MPNs diagnosis was 48
% and 77 %, respectively, which agreed with the results reported by Tefferi, et al. the CD177 MFI similarly revealed a high accuracy level in the differentiation between PV and secondary erythrocytosis in this study (sensitivity 40% and 85% specificity with a 20 p.d.u cut off) [21]. This was in agreement with the results reported by Klippel, et al. Passamonti, et al. Sirhan, et al. [11, 12, 14]. However, a low sensitivity (AUC of 0.58) of the CD177 % in the diagnosis of MDS patients was observed in our study. This contradicts the results reported by Meyerson, et al. [9]. However, their MDS patient’s diagnosis was not entirely based on WHO diagnostic criteria as in the present study; a factor which may reduce the comparability of their results.
In conclusion, our results suggest that CD177 expression has good potential as a marker in the diagnosis of c-MPNs. Flow cytometry analysis of CD177 expression is a simple stable method in clonal myeloid neoplasms, particularly in the diagnosis of challenging cases of Philadelphia-negative c-MPDs such as triple-negative and pediatric cases, and in differentiating ET from pre-fibrotic IMF. It would be also useful in confirming the differentiation of c-MPNs from reactive cases, especially PV and SE. Further larger studies and wide-scale clinical trials of this marker are recommended for clinical application.
Ethical Compliance
This study was performed according to the recognized standards of the “Declaration of Helsinki” for the Protection of Human Subjects including:
- Anonymous collection of patient’s data, excluding all identifying data. Obtained data included age, gender, final diagnosis, directly relevant diagnostic investigations e.g. BCR-ABL1 & JAK-2 etc.
- Patient’s informed consent was obtained for the extra- blood sample collection. A standard Informed consent form is used according to the standards required in the “Declaration of Helsinki” and in compliance with the Ethical Committee of Cairo University.
- Extra-sample was anonymously obtained during routine follow up patients visits.
Using coded de-identified vacutainers after obtaining patient’s consent.
References
-
Caruccio L, Bettinotti M, Director‐Myska AE, Arthur DC, Stroncek D (2006) The gene overexpressed in polycythemia rubra vera, PRV‐1, and the gene encoding a neutrophil alloantigen, NB1, are alleles of a single gene, CD177, in chromosome band 19q13. 31. Transfusion 46(3): 441-447.
-
Stroncek DF, Caruccio L, Bettinotti M (2004) CD177: A member of the Ly-6 gene superfamily involved with neutrophil proliferation and polycythemia vera**.** Journal of Translational Medicine 2: 8.
-
Sachs UJ, Andrei-Selmer CL, Maniar A, Weiss T, Paddock C, et al. (2007) The neutrophil-specific antigen CD177 is a counter-receptor for platelet endothelial cell adhesion molecule-1 (CD31). J Biol Chem 282(32): 23603-23612.
-
Bayat B, Werth S, Sachs UJH, Newman DK, Newman PJ, et al. (2010) Neutrophil transmigration mediated by the neutrophil-specific antigen CD177 is influenced by the endothelial S536N dimorphism of platelet endothelial cell adhesion molecule-1. J Immunol 184(7): 3889-3896.
-
Kuckleburg CJ, Tilkens SB, Santoso S, Newman PJ (2012) Proteinase 3 contributes to transendothelial migration of NB1-positive neutrophils. J Immunol 188(5): 2419- 2426.
-
Wu Z, Liang R, Ohnesorg T, Cho V, Lam W, et al. (2016) Heterogeneity of Human Neutrophil CD177 Expression Results from CD177P1 Pseudogene Conversion. PLoS Genet 12(5): e1006067.
-
Eulenberg‑Gustavus C, Bähring S, Maass PG, Luft FC, Kettritz R (2017) Gene silencing and a novel monoallelic expression pattern in distinct CD177 neutrophil subsets. J Exp Med 214(7): 2089-2101.
-
Slezak S, Jin P, Lorraine Caruccio L (2009) Gene and microRNA analysis of neutrophils from patients with polycythemia vera and essential thrombocytosis: down-regulation of micro RNA-1 and -133a. Journal of Translational Medicine 7: 39.
-
Meyerson HJ, Osei E, Schweitzer K, Blidaru G, Edinger A, et al. (2013) CD177 Expression on Neutrophils: In Search of a Clonal Assay for Myeloid Neoplasia by Flow Cytometry. American journal of clinical pathology 140(5): 658-669.
-
Cilloni D, Carturan S, Gottardi E, Messa F, Fava M, et al. (2004) Usefulness of the quantitative assessment of PRV-1 gene expression for the diagnosis of polycythemia vera and essential thrombocythemia patients. Blood 103(6): 2428-2429.
-
Passamonti F, Pietra D, Malabarba L, Rumi E, Porta MG, et al. (2004) Clinical significance of neutrophil CD177 mRNA expression in Ph‐negative chronic myeloproliferative disorders. British journal of haematology 126(5): 650- 656.
-
Sirhan S, Lasho TL, Elliott MA, Tefferi A (2005) Neutrophil polycythemia rubra vera-1 expression in classic and atypical myeloproliferative disorders and laboratory correlates. Haematologica 90(3): 406-408.
-
Chang H, Hung YS, Chang CH, Huang YH, Lin TL, et al. (2012) Clinical Utility of PRV-1 mRNA Expression Levels in Polycythemia Vera and Essential Thrombocythemia. Blood 120(21): 2846.
-
Klippel S, Strunck E, Temerinac S, Bench AJ, Meinhardt G, et al. (2003) Quantification of PRV-1 mRNA distinguishes polycythemia vera from secondary erythrocytosis. Blood 102(10): 3569-3574.
-
Liu E, Jelinek J, Pastore YD, Guan Y, Prchal JF, et al. (2003) Discrimination of polycythemias and thrombocytoses by novel, simple, accurate clonality assays and comparison with PRV-1 expression and BFU-E response to erythropoietin. Blood 101(8): 3294-301.
-
Tefferi A, Lasho TL, Wolanskyj AP, Mesa RA (2004) Neutrophil PRV-1 expression across the chronic myeloproliferative disorders and in secondary or spurious polycythemia. Blood 103(9): 3547-3548.
-
Tutaeva V, Misurin AV, Michiels JJ, Rozenberg JM, Sokolova MA, et al. (2007) Application of PRV-1 mRNA expression level and JAK2V617F mutation for the differentiating between polycytemia vera and secondary erythrocytosis and assessment of treatment by interferon or hydroxyurea. Hematology 12(6): 473-479.
-
Bock O, Serinsöz E, Neusch M, Schlué J, Kreipe H (2003) The polycythaemia rubra vera‐1 gene is constitutively expressed by bone marrow cells and does not discriminate polycythaemia vera from reactive and other chronic myeloproliferative disorders. British journal of haematology 123(3): 472-474.
-
Rapado I, Albizua E, Ayala R, Hernández JA, Garcia- Alonso L, et al. (2008) Validity test study of JAK2 V617F and allele burden quantification in the diagnosis of myeloproliferative diseases. Annals of hematology 87(9): 741-749.
-
Goerttler PS, Steimle C, März E, Johansson PL, Andreasson B, et al. (2005) The Jak2V617F mutation, PRV-1 overexpression, and EEC formation define a similar cohort of MPD patients. Blood 106(8): 2862- 2864.
-
Tefferi A, Sirhan S, Lasho TL, Schwager SM, Li CY, et al. (2005) Concomitant neutrophil JAK2V617F mutation screening and PRV‐1 expression analysis in myeloproliferative disorders and secondary polycythaemia. British journal of haematology 131(2): 166-171.
-
Mnjoyan Z, Yoon D, Li J, Delhommeau F, Afshar-Kharghan V (2006) The effect of the JAK2 V617F mutation on PRV- 1 expression. Haematologica 91(3): 411-412.
-
Bennett M, Stroncek DF (2006) Recent advances in the bcr-abl negative chronic myeloproliferative diseases. Journal of translational medicine 4(1): 1.
-
Vannucchi AM, Guglielmelli P, Antonioli E, Mappa S, Pancrazzi A, et al. (2006) Inconsistencies in the association between the JAK2V617F mutation and PRV‐1 over‐expression among the chronic myeloproliferative diseases. British journal of hematology 132(5): 652-654.
-
Baxter EJ, Scott LM, Campbell PJ, East C, Fourouclas N, et al. (2005) Acquired mutation of the tyrosine kinase JAK2 in human myeloproliferative disorders. Cancer Genome Project. Lancet 365(9464): 1054-61.
-
James C, Ugo V, Le Couédic JP, Staerk J, Delhommeau F, et al. (2005) A unique clonal _JAK2_ mutation leading to constitutive signalling causes polycythaemia vera. Nature 434(7037): 1144-1148.
-
Kralovics R, Passamonti F, Buser AS, Teo SS, Tiedt R, et al. (2005) A Gain-of-Function Mutation of _JAK2_ in Myeloproliferative Disorders. N Engl J Med 352(17): 1779-1790.
-
Levine M, Davidson EH (2005) Gene regulatory networks for development. PNAS 102(14): 4936-4942.
-
Al-Shami A, Mahanna W, Naccache PH (1998) Granulocyte-Macrophage Colony-stimulating Factor- activated Signaling Pathways in Human Neutrophils. Selective Activation of Jak2, Stat3, AND Stat5B**.** Journal of Biological Chemistry 273(2): 1058-1063.
-
Shahrabi S, Ehsanpour A, Heidary S, Shahjahani M, Behzad MM (2018) Expression of CD markers in JAK2V617F positive myeloproliferative neoplasms: Prognostic significance. Oncology Reviews 12(2): 373.
-
Teofili L, Martini M, Luongo M, Di Mario A, Leone G, et al. (2002) Overexpression of the polycythemia rubra vera- 1 gene in essential thrombocythemia. Journal of clinical oncology 20(20): 4249-4254.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey