Efficacy of Errector Spinae Plane Block in Postoperative Pain Controle after Laparoscopic Cholecystectomy
Objective: To assess the efficacy of bilateral Erector Spinae plane (ESP) block in pain outcome after laparoscopic cholecystectomy. Material & Methods: This descriptive study was conducted at Surgical Department Hayatabad Medical Complex Peshawar. A total of 52 patients were included, Female 39 (78%), Male 13 (22%). In the first post op day the NRS score were recorded as 1/10 during first hour while they stayed at <3 up to 18 hours in all patients and none of them received standard analgesia. Conclusion: Bilateral ESP block is a useful technique to provide post op analgesia in the first 24 hours reducing the need for opoid analgesia.
Introduction
Cholelithiasis is one of the major causes of morbidity worldwide with gross geographical variations. Asian countries have an estimated prevalence of 3-5%, as compared to European countries where the prevalence maybe as high as 10-15%. In Pakistan the number of patients affected by gall stones are increasing day by day [1]. Laproscopic cholecystectomy is considered the gold standard treatment modality for the management of gallstones [2, 3]. Despite being minimally invasive procedure, post-operative pain is a significant complication amongst many causing discomfort to the patient which is mostly controlled by the use of multimodal analgesic regimens [4]. However, due to its significant side effects newer modalities of treatment are being devised in order to enhance recovery [5, 6].
Described for the first time by Forero et al., in 2016, Erector spine plane block (ESPB) is an ultrasound guided interfascial block to attain regional anesthesia/analgesia.
Although initially it was utilized to manage acute thoracic neuropathic pain, it has since been indicated for effective pain control in various conditions such as post operative abdominal surgery patients, post op breast surgery patients, rib fractures, pelvic surgeries, burns patients as well as an anesthetic technique in minor surgical procedures [7].
ESPB has been used as a mean of postoperative analgesia in laproscopic cholecytectomy in patients across the globe, and is still being researched upon and documented in multiple case series. However, this innovative technique has yet to be utilized in Pakistan [8, 9, 10, 11, 12, 13, 14, 15]. Our team will be the first to document the outcome of ESPB in the underdeveloped world and contribute to the pool of research work that is still being analyzed in order to determine its efficacy.
Material and Methods
This study was conducted in collaboration with Department of Surgery & Anesthesia, Hayatabad Medical Complex Peshawar during the period from 1st June 2019 to 30th May 2020. A total of 52 patients scheduled for elective cholecystectomy were included in the study after taking informed consent. Age limit was set at 20-75 yrs with no preference to male or female patients. The patients included had an ASA status I/II and a normal coagulation profile. Obese and patients who were allergic to any of the used drugs or had infections at the puncture site were excluded from the study. After approval from the ethical committee of the hospital all patients were counseled for the risk benefit ratio of the block prior to surgery.
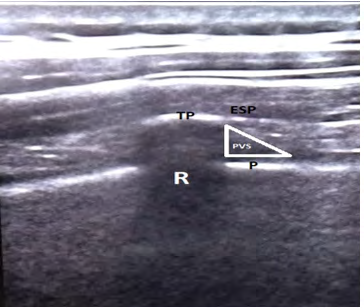
On the day of surgery 18 G I/V line was passed to all the patients and infusion started. Preoperatively, patients were given anxiolytics and 10 mg Nalbuphine along with prophylactic antibiotics. Basic monitoring of the patients was started. The patient was then asked to sit and a preliminary scan was done using an ultrasound linear probe to define and mark the required level T6-T8. Both midline and bilateral points were marked. After identification of the desired level, the skin was anesthetized by 2ml of Lignocaine and a 22g spinal needle was introduced. The needle was viewed in an in-plane technique and when firm contact was made with the transverse process at the desired level, hydro dissection was done with normal saline. Spread of the fluid was visually confirmed both cranially and caudally. Single shot technique with no catheter insertion was applied. After negative aspiration, 20 ml of 0.25 % Bupivacaine was injected in increments of 5 ml.
After the block was effective, the patient was induced with Propofol 150 mg and Atracurium 40mg; and maintained with oxygen, nitrous oxide and Isoflurane. At the end of the procedure reversal was done with Neopyrolate. Following extubatation good ventilation and pressure support was ensured with normal blood pressure and respiratory pattern. Patient was put on diclofenac as standard analgesia and Tramdol as rescue analgesia. Patient’s pain was assessed with the NRS at 0-30 min and 1, 3, 6, 12, 18 and 24 hours. Pent scale (none, mild, moderate and severe) was used for the assessment of postoperative nausea and vomiting (PONV).
Results
Post operatively only 2 (3.8%) patients had an NRS of 2/10 in 0-30 minutes after surgery, while all stayed at 3/10 for up to 12 hrs. At 18 hours 6 (11.5%) patients had an NRS of 5/10 and received rescue analgesia in the form of opiod analgesic. At 24 hours 10(19.2%) patients had an NRS of 5/10 requiring opiod analgesic. None of the patients having an NRS of 3/10 received additional analgesia.
| Time | Nrs Score | No.of Pts |
|---|---|---|
| 0-30 mints | 2/10 | 2 (3.8%) |
| 1 hr | 1/10 | 52(100%) |
| 3 hrs | 3/10 | 52(100%) |
| 6 hrs | 3/10 | 52(100%) |
| 12 hrs | 3/10 | 52(100%) |
| 18 hrs | 5/10 | 6(11.5%) |
| 24 hrs | 5/10 | 10(19.2%) |
Table 1: Nrs Score in First 24 Hours. Post-operative nausea vomiting (PONV) were noted in 2(3.8%) patients which were treated wit
Discussion
Post-operative pain and nausea vomiting (PONV) are some of the most common complications of Lap chole. Though significantly less as compared to open cholecystectomy still it continues to be a source of discomfort for the patient [16, 17]. Visceral pain due to irritative effects of the insufflating gases and diaphragmatic stretching is the most common cause of post op pain in such patients, followed by port site pain and shoulder pain [16, 18].
In order to lower the pain scores several regimens and blocks have been introduced with variable results. Multimodal analgesia, port site infiltration, low pressure pneumoperitoneum and pulmonary recruitment maneuvers are some that contribute significantly in reducing post op pain. Epidural catheter, paravertebral block, TAP block, Rectus sheath block, quadrates lamborum blocks etc have all been attempted and stay quite successful in lowering the pain scores although with a significant risk [6, 19].
ESPB is a novel technique in which local anesthesia is injected into the fascial plane deep to the erector spinae muscle anesthetizing not only the dorsal and ventral rami of the spinal nerves but also blocking the sympathetic nerves [7]. Its tendency to spread both cranially and caudally as demonstrated in cadavers and MR scans further enhances its utility and makes it a preferable mode of analgesia [7, 8, 9, 10, 12, 20]. This technique is not only minimally invasive, but also simpler, safer and quicker to perform [8]. ESPB provides indirect access to the paravertebral space minimizing the potential risk of pneumothorax [21]. Unlike epidural block this technique can be useful in anti coagulated patients and can be performed prior to induction, under GA and even post operatively, as a single shot or via a continuous infusion using indwelling catheter [22]. The technique has been successfully performed in obese and high risk patients in whom other blocks are difficult to perform due to sonological non visualization [7, 23]. Tulgar, et al in his study elaborated its utility in a patient undergoing laparoscopic cholecystectomy as well as hernia repair in a single session [7]. He was able to achieve appreciable analgesia with ESP Block only where otherwise the patient would have required two different blocks at two different location [24].
In our study 2(3.8%) patients reported an NRS of 2 in the immediate post op period which is comparable to a study performed by Aksu et al, where they reported an NRS of 2 in the first post op hour and 0 NRS at 24 hour postoperatively. A study by Tulgar et al estimating the efficacy of ESPB in comparison to OSTAP block and a control group who received no block, reported an NRS of 3 upto 18 hours postoperatively [5]. However at 24 hrs none of the patients in Tulgar’s study had an NRS of >3 as compared to our study where 10 (19.2%) patients reported an NRS of 5 requiring opiods [25]. In a case series by Alessandro, et al. an NRS of 3 was documented in the first 8 hours [26].
Opiod requirements were significantly reduced in patients who received ESP block postoperatively. None of the patients required analgesia in the first 12 hours. At 18 hours 6(11.5%) patients needed opiods and at 24hrs 10(19.2%) patients needed opiods in our study. Tulgar, et al. reported an NRS of <3 in the ESPB group up to 24 hours postoperatively; 3 (16%) patients were administered opiod analgesic in the first 12hours while another 2(11.11%) patients in the next 12hours. In the same study where he compared ESPB to control group significantly higher rescue analgesics were required [25].
PONV which was observed in only 2 (3.8%) patient’s postoperatively. Tulgar et al., reported PONV in 1(5.55%) patients in the ESPB group and 2(11.11%) patients in the control group. Kjartan et al., reported PONV in none of the patients who received ESPB [25]. We used 20ml of 2.5% Bupivicaine which was successful in providing analgesia upto 18 hrs [27]. Tulgar, et al. also used the same amount and was able to achieve analgesia in upto 24hrs in almost all patients. Luftig, et al. in their review article recommended a weight based dose i.e. 2 mg/kg for bupivicaine to be used in order to achieve adequate anesthesia [25, 28].
As this technique is being evaluated for its beneficial aspects, there are still some unanswered questions e.g. dose of local anaesthesia required, its systemic toxicity etc which needs further studies. Comparative studies are required comparing it with other blocks.
Conclusion
We conclude that a bilateral ESP block using 20ml of bupivucaine is sufficient to provide analgesia in the first 24hrs reducing the need for opiods.
References
-
Kratzer W, Mason RA, Kachele V (1999) Prevalence of gallstones in sonographic surveys worldwide. Journal of Clinical Ultrasound 27(1): 1-7.
-
Channa NA, Khand FD, Bhanger MI, Leghari MH (2004) Surgical incidence of Cholelithiasis in Hyderabad and adjoining areas (Pakistan). Pakistan Journal of Medical Science 20(1): 13-17.
-
Khand FD (1997) Cholelithiasis in Southern Sindh (Pakistan): Incidence and composition of gallstones. Pakistan Journal of Medical Sciences 13(3): 263-270.
-
Pazouki A, Cheraghali R, Saeedimotahhar H, Jesmi F, Jangjoo A, et al. (2015) Pre-operative Rectal Indomethacin for Reduction of Postoperative Nausea and Vomiting after Laparoscopic Cholecystectomy: A Double-Blind Randomized Clinical Trial. J Coll Physicians Surg Pak 25(1): 56-59.
-
Can A, Alparslan K, Hadi Y, , Cennet KT, Yavuz G (2019) The Effect of Erector Spinae Plane Block on Postoperative Pain Following Laparoscopic Cholecystectomy: A Randomized Controlled Study. Journal of Anesthesiology and Reanimation Specialists’ Society 27(1): 9-14.
-
Bisgaard T (2006) Analgesic treatment after laparoscopic cholecystectomy: a critical assessment of the evidence. Anesthesiology 104(4): 835-846.
-
Forero M, Adhikary SD, Lopez H, Tsui C, Chin KJ (2016) The erector spinae plane block: a novel analgesic technique in thoracic neuropathic pain. Reg Anesth Pain Med 41(5): 621-627.
-
Chin KJ, Adhikary S, Sarwani N, Forero M (2017) The analgesic efficacy of pre-operative bilateral erector spinae plane (ESP) blocks in patients having ventral hernia repair. Anaesthesia 72(4): 452-60.
-
Bonvicini D, Giacomazzi A, Pizzirani E (2017) Use of the ultrasound-guided erector spinae plane block in breast surgery. Minerva Anestesiol 83(10): 1111-1112.
-
Veiga M, Costa D, Brazão I (2018) Erector spinae plane block for radical mastectomy: A new indication?. Rev Esp Anestesiol Reanim 65(2): 112-115.
-
Luftig J, Mantuani D, Herring AA, Dixon B, Clattenburg E, et al. Successful emergency pain control for posterior rib fractures with ultrasound-guided erector spinae plane block. Am J Emerg Med 36(8): 1391-1396.
-
Tulgar S, Selvi O, Senturk O, Ermis MN, Cubuk R, et al. (2018) Clinical experiences of ultrasound-guided lumbar erector spinae plane block for hip joint and proximal femur surgeries. J Clin Anesth 47: 5-6.
-
Ueshima H, Otake H (2018) Continuous erector spinae plane block for pain management of an extensive burn. Am J Emerg Med 36(11): 2130.e1-2130.e2.
-
Balaban O, Aydin T, Yaman M (2018) Is ultrasound guided erector spinae plane block sufficient for surgical anesthesia in minor surgery at thoracal region?. J Clin Anesth 47: 7-8.
-
Tulgar S, Thomas DT, Deveci U (2018) Erector spinae plane block provides sufficient surgical anesthesia for ileostomy closure in a high-risk patient. J Clin Anesth 48: 2-3.
-
Bisgaard T, Kehlet H, Rosenberg J (2001) Pain and convalescence after laparoscopic cholecystectomy. European Journal of Surgery 167(2): 84-96.
-
Jensen K, Kehlet H, Lund CM (2007) Post-operative recovery profile after laparoscopic cholecystectomy: A prospective, observational study of a multimodal anaesthetic regime. Acta Anaesthesiologica Scandinavica 51(4): 464-471.
-
Donatsky AM, Bjerrum F, G¨ogenur I (2013) Surgical technique to minimize shoulder pain after laparoscopic cholecystectomy. A systematic review. Surgical Endoscopy 27(7): 2275-2282.
-
Chin KJ, McDonnell JG, Carvalho B, Sharkey A, Pawa A, et al. (2017) Essentials of our current understanding: Abdominal wall blocks. Regional Anesthesia and Pain Medicine 42(2): 133-183.
-
Chin KJ, Malhas L, Perlas A (2017) The Erector Spinae Plane Block Provides Visceral Abdominal Analgesia in Bariatric Surgery: A Report of 3 Cases. Reg Anesth Pain Med 42(3): 372-376.
-
El-Boghdadly K, Pawa A (2017) The erector spinae plane block: Plane and simple. Anaesthesia 72(4): 434-438.
-
López M, Cadórniga Á, González J, Suárez E, Carballo C, et al. (2018) Erector Spinae Block. A Narrative Review. Central European Journal of Clinical Research 1(1): 28- 39.
-
Darling CE, Pun SY, Caruso TJ, Tsui BCH (2018) Successful directional thoracic erector spinae plane block after failed lumbar plexus block in hip joint and proximal femur surgery. J Clin Anesth 49: 1-2.
-
Tulgar S, Selvi O, Kapakli MS (2018) Erector Spinae Plane Block for Different Laparoscopic Abdominal Surgeries: Case Series. Case reports in anesthesiology.
-
Tulgar S, Kapakli MS, Kose HC, Senturk O, Selvi O, et al. (2019) Evaluation of Ultrasound-Guided Erector Spinae Plane Block and Oblique Subcostal Transversus Abdominis Plane Block in Laparoscopic Cholecystectomy: Randomized, Controlled, Prospective Study. Anesthesia, essays and researches 13(1): 50-56.
-
De Cassai A, Cin SD, Zarantonello F, Ban I (2019) Erector spinae plane block as a rescue therapy for uncontrolled pain after laparotomic surgery: A report of two cases. Saudi journal of anaesthesia 13(1): 66-68.
-
Hannig KE, Jessen C, Soni UK, Børglum J, Bendtsen JF (2018) Erector Spinae Plane Block for Elective Laparoscopic Cholecystectomy in the Ambulatory Surgical Setting. Case Reports in Anesthesiology.
-
Luftig PJ, Mantuani D, Herring AA, Dixon B, Clattenburg E, et al. (2018) The authors reply to the optimal dose and volume of local anesthetic for erector spinae plane blockade for posterior rib fractures. Am J Emerg Med 36(6): 1103-1104.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey