Unusual Penetrating, Retained Cardiac Intramural Foreign Body: Case Report
Penetrating cardiac injuries are devastating lesions that represent a major challenge with a high mortality (40-90%). Such injuries are considered a real challenge because of their unpredictable clinical course. Our case is unique to describe a nail penetrated the heart through the right atrium, sparing the tricuspid valve, the inter-ventricular septum, and the conduction system to be retained intramurally at the right ventricular inferior wall without an exit point. Timely diagnosis and proper operative management; enabled us to rescue a victim with penetrating cardiac injury. The use of CPB and the epicardial ultrasonography was beneficial in detecting and extracting the FB.
Introduction
Penetrating cardiac injuries are exceedingly devastating lesions with a high mortality rate (40-90%) [1]. Such injuries are considered a real surgical challenge. Our present case, to our knowledge, is one-of-a-kind to describe a metallic carpenter’s nail penetrated the heart through the right atrium, found its way within the myocardium sparing the tricuspid valve, the interventricular septum, and the conduction system to be retained intramurally at the inferior diaphragmatic right ventricular (RV) wall without an exit point.
Case History and Perioperative Data
Fifty-nine years old gentleman, his body mass index (BMI) was 38Kg/m2. There was a penetrating chest injury from the right side (3rd intercostal space 5cm away from the midline) caused by a “metallic nail” injured him from a carpenter’s nail gun (Figure 1A). Initial clinical examination revealed his unstable hemodynamics. Upon arrival CXR (Figure 1B) and CT chest without contrast were done (Figure 2); which showed the FB clearly, mild pericardial collection (hemopericardium), right hemothorax. Bedside TTE done also showed the pericardial collection but no vision for the FB. Consensus decision was taken to perform an emergency thoracic exploration. The patient and his relatives consented for this emergency intervention and for their approval to use the patient’s data for academic purposes. Our ethical research committee has approved this manuscript for publication.
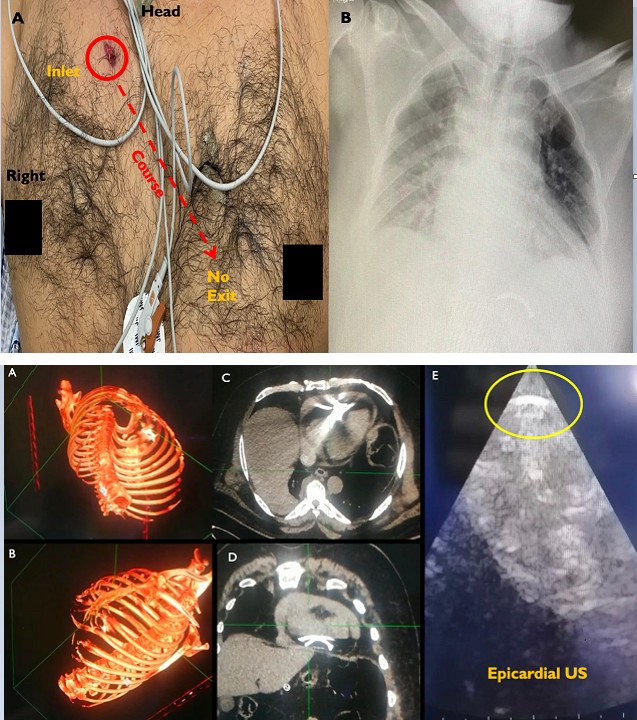
Figure 1A: Showing the anterior aspect of the patient’s chest. The foreign body inlet was 5 cm away from the midline on the 3rd right intercostal space; the dashed line indicates the provisional course of the FB (Nail) without an exit point. Figure 1B: Plain Chest X-ray AP view, showing the (nail) at the level of the left diaphragmatic copula, right lung field haziness.
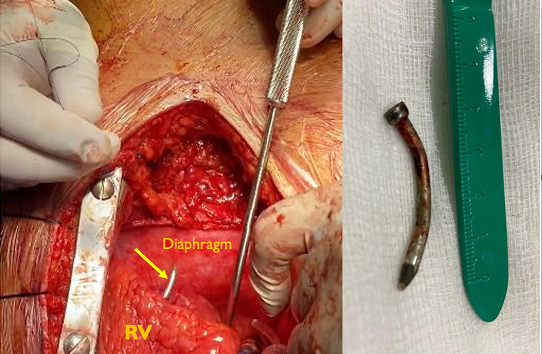
Thoracic Exploration through full median Sternotomy for FB extraction on pump (CPB) was done for better exposure. TEE could not show the FB. Only by intraoperative epicardial US we could detect the intramural FB in inferior diaphragmatic surface of RV (Figure 2E). We noticed the inlet in the free border of the RA sealed by a fresh blood clot then was secured by 4/0 Prolene® suture with pericardial pledgets. Extraction of the FB performed through the diaphragmatic RV wall (Figure 3) and the exit controlled by two stiches 4/0 Prolene® with Teflon pledgets.
Discussion
Penetrating cardiac injuries can easily jeopardize patients’ lives, unless promptly diagnosed and treated. The first intra cardiac FB case was reported by Wood W, in 1814, who described the history and the dissection findings [2]. Yet still rare cases, there were wide range of FBs described by authors like; sewing needles, acupunctures, bullets, missiles, Kirschner wires, venous catheters, and pencils. To our knowledge, this is the first reported case of a retained metallic nail inside the heart muscle.
In such cases, serious outcomes could ensue (e.g., hemothorax, tamponading hemopericardium, pneumothorax, mural thrombi with embolization, infective endocarditis, valve leaflet perforation, and ventricular septal rupture) [3]. Although there was controversy, owing to the limited number of cases, whether to intervene surgically, especially if asymptomatic, some authors reported reference of the conservative management.
Endovascular interventionists attempted to retrieve FBs percutaneously as performed by Carroll and colleagues [4]. Dagdelen S, et al. stated that less invasive procedures by using snare-loop catheter, could prevent grave consequences of open surgical retrieval [5]. Our rational to use the CPB is to establish a bloodless surgical field for better exposure, and to avoid migration of the FB through the peripheral circulation.
Regarding the diagnosis of the intracardiac FBs, Leitman M. and Vered Z. confirmed in their review that the use of transthoracic echocardiography (TTE) had nearly 100% diagnostic sensitivity, followed by Transesophageal Echocardiography (TEE) and this was not in our case where the TTE and TEE could not detect the FB in the heart which could be detected only with epicardial US [6].
Worth, Symbas and coworkers concluded that right ventricle (37.5%) was the most frequently involved part, compared to left ventricle (28.4%), pericardium (12.5%), right atrium (9%), and left atrium (3.4%) after reviewing 222 cases of retained missiles in heart [7]. We agree as our victim experienced the FB was settled in his RV wall, but it wasn’t the scenario for diagnosing its presence preoperatively by TTE and intraoperative TEE, our patient was overweight (130 Kg) which hindered ultrasound tissue penetrance. Here we emphasize the utmost importance of Epicardial echocardiography intraoperatively to visualize myocardium, heart chambers clearly and flawlessly.
We cannot deny the role of computed tomography (CT) scanning for correct localization of intrathoracic FB. Many authors supported the Hounsfield Units (HU) function in CT to detect the nature of thoracic and cardiac FB, this agreement was equal between surgeons and less invasive interventionists [8]. Ultimately, the patient’s life could greatly rely on the experience of the treating heart team, namely the skilled heart surgeon, the echocardiographer, and the “eagle- eyed” radiologist.
Conclusion
Our case is unique to describe a nail penetrated the heart through the right atrium, sparing the tricuspid valve, the inter-ventricular septum, and the conduction system to be retained intramurally at the right ventricular inferior wall without an exit point. The use of CPB and the use of epicardial ultrasonography were indeed beneficial in detecting and extracting the FB from the heart muscle.
The timely diagnosis by using of multiple radiological modalities and proper operative management; is mandatory to enable the heart team to rescue such patients.
References
-
Castriconi M, Festa P, Bartone G, Maglio MD, Vicenzo L, et al. (2013) Penetrating cardiac injuries. Two case reports. Ann Ital Chir 84(ePub): S2239253X13020987.
-
Wood W (1814) History and Dissection of a Case, in Which a Foreign Body Was Found within the Heart. Edinb Med Surg J 10(37): 50-54.
-
Actis Dato GM, Arslanian A, Di Marzio P, Filosso PL, Ruffini E (2003) Posttraumatic and iatrogenic foreign bodies in the heart: report of fourteen cases and review of the literature. J Thorac Cardiovasc Surg 126(2): 408- 414.
-
Carroll MI, Ahanchi SS, Kim JH, Panneton JM (2013) Endovascular foreign body retrieval. J Vasc Surg 57(2): 459-463.
-
Dagdelen S, Yuce M, Caglar N (2007) Percutaneous removal of two intracardiac and pulmonary truncal catheter fragment by using a snare-loop catheter. Int J Cardiol 116(3): 413-415.
-
Leitman M, Vered Z (2015) Foreign bodies in the heart. Echocardiography 32(2): 365-371.
-
Symbas PN, Picone AL, Hatcher CR, Vlasis-Hale SE (1990) Cardiac missiles. A review of the literature and personal experience. Ann Surg 211(5): 639-647.
-
Wang X, Zhao X, Du D, Xiang X (2012) Management of metallic foreign bodies in the heart. J Card Surg 27(6): 704-706.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey