Primary High Grade Muscle Invasive Bladder Urothelial Carcinoma with Metastasis to the Penis Sparing the Urethra- A Case Presentation and Review of Literature
Background: Metastatic transitional cell carcinoma in the penis is extremely rare. Symptoms like penile pain, swelling, or priapism should raise the suspicion, when they happen in a known case of invasive bladder cancer. Case presentation: We report an unusual case of penile pain and swelling in a 69-year-old man, known to have invasive bladder cancer that was initially treated with radiotherapy. Although both penile ultrasound and MRI suspected hematoma or scarring rather than malignancy, the penile biopsy confirmed metastatic transitional cell carcinoma. Conclusion: Metastatic urothelial carcinoma in the penis is a rare presentation with poor prognosis, where treatment options are very limited and mainly palliative
Background
Penile metastasis of urothelial bladder cancer are extremely rare as per literature. It indicates a disseminated disease and hence a poor prognosis. Regarding how it present, this is usually in the form of penile nodule or priapisim. Most cases present after a mean time of 18 months from the diagnosis of primary bladder cancer.
A 69-year-old male diagnosed with G3T2 TCC of the bladder (T2NoMo) 10 months ago. Due to multiple co-morbidities he was not a candidate for neoadjuvant chemotherapy or radical surgery. MDT recommended EBRT. Six months ago patient has completed 46.75 Gy in 17 fractions. Due to severe diarrhoea he couldn’t complete 20 fractions as planned. His first surveillance cystoscopy after radiotherapy (3 months later) was clear. However on the second surveillance cystoscopy after another 3 months, patient couldn’t tolerate the test as his penis was very sore, and for the first instance looked like having a priapism. There was partial erection in the shaft of the penis, but there was no rigidity at the base.
Hence we suspected either metastasis from the bladder cancer or primary penile cancer. The later was less likely as there was no exophytic lesion on the skin surface. On clinical examination there was no palpable lymph nodes. Prostate cancer wasn’t a concern as digital rectal examination revealed a smooth large prostate, and PSA 1.1.
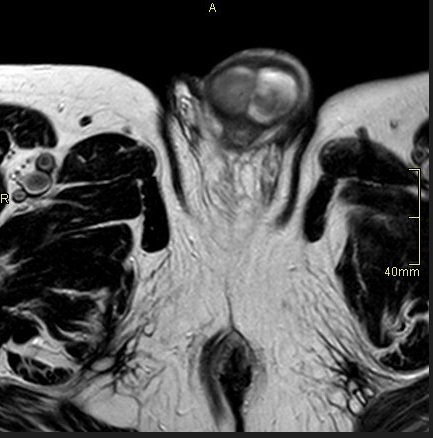
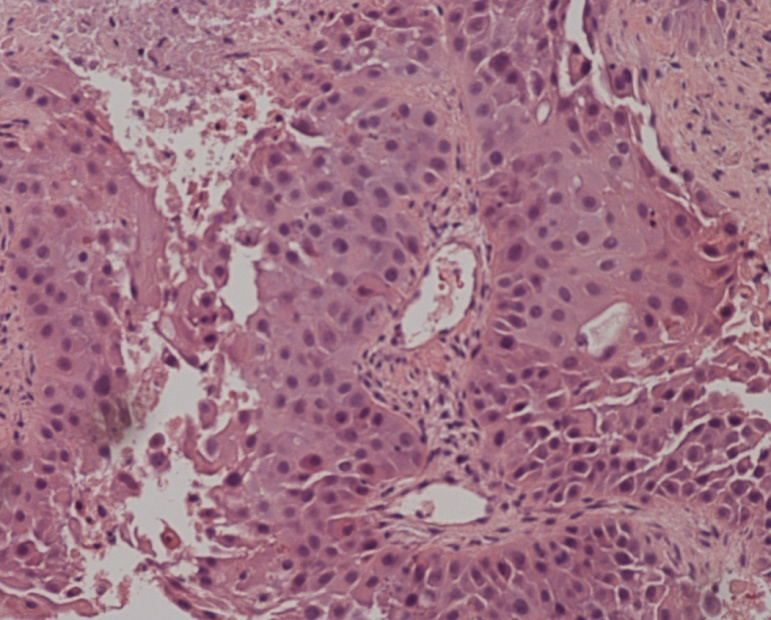
MRI pelvis showed a 27 mm T2 hyperintense plaque on the left corpus cavernosum, a thinner lesion on the other side, both with features suggestive of a hematoma or scarring, however MRI recommended a penile ultrasound for confirmation. Ultrasound again confirmed a hematoma. GA cystoscopy revealed a clear urethra and bladder. Final test was true cut biopsy from each side of corpora, and the histology came back as metastatic high grade urothelial carcinoma (Figures 1 & 2).
Case was discussed at our local MDT meeting. The recommendation was to get a new CT-TAP for restaging, and to consider palliative treatment.
The new CT-TAP showed cancer has spread to liver and lung. Patient was offered palliative chemotherapy and radiotherapy, however he declined.
One month later patient had acute urinary retention. Due to severe penile pain urethral catheter was inserted under GA. Later on bilateral nephrostomies were inserted.
Conclusion
High grade muscle invasive urothelial carcinoma is notoriously known of micrometastasis at time of presentation. Hence the extreme importance of regular checks by clinical evaluation and imaging. In addition to surveillance cystoscopies to role out recurrence in case bladder preserving approach was adopted [1].
Penile metastasis from bladder urothelial carcinoma is a rare presentation and usually associated with poor prognosis. The average survival is 3.9 months from diagnosis. It may reach 9.2 months with extensive surgery and chemotherapy [2].
According to literature, the common way of spread of bladder urothelial carcinoma to the penis is by retrograde venous route [3].
The other possible mechanisms for penile metastasis include retrograde lymphatic spread, direct invasion, direct arterial spread, and instrumental seeding [4].
Treatment always requires an MDT approach. And the options include local tumour excision, external beam radiation therapy, brachytherapy, chemotherapy, or partial or total penectomy [5].
Declaration
Conflicting Interests: I declare that there is no conflict of interest. Funding: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Informed Consent: Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article. Ethical Approval: Ethical approval to report this case was obtained from ETHICS COMMITTEE at Calderdale and Huddersfield NHS Foundation Trust. Guarantor: TQ Contributorship: Consenting the patient, writing the case report, liaising with radiology and histology for getting the necessary pics. Acknowledgements: I would like to thank my colleagues for their assistance.
References
-
Paquin AJ, Roland SI (1956) Secondary carcinoma of the penis. A review of the literature and a report of nine new cases. Cancer 9(3): 626-632.
-
Berger AP, Rogatsch H, Hoeltl L, Steiner H, Bartsch G, et al. (2003) Late penile metastasis from primary bladder carcinoma. Urology 62(1): 145.
-
Yang XJ, Lecksell K, Epstein JI (1999) Can Immunohistochemistry Enhance the Detection of Micrometastases in Pelvic Lymph Nodes From Patients With High-Grade Urothelial Carcinoma of the Bladder. Am J Clin Pathol 112(5): 649-653.
-
Zhu YP, Yao XD, Zhang HL, Shen YJ, Huang D, et al. (2012) Penile Metastasis from Primary Bladder Cancer: A Study of 8 Cases and Review of the Literature. Onkologie 35(4): 196-199.
-
Pomara G, Pastina I, Simone M, Casale P, Marchetti G, et al. (2004) Penile metastasis from primary transitional cell carcinoma of the renal pelvis: first manifestation of systemic spread. BMC Cancer pp: 4.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey