Role of Plastic Periodontal Therapy in Clinical Management of Orthodontically Treated Vertical Maxillary Excess
Introduction: The most challenging task for an orthodontist is to achieve harmonious smile, especially in ‘‘gummy smile' or (vertical maxillary excess) cases. These kinds of cases are treated with either intrusion or orthognathic surgery. The most acceptable method is an intrusion, which is associated with buccal cortical bone thickening and decrease clinical crown length. The main aim of this case report is to explore the difference between with and without plastic periodontal therapy after the intrusion. Conclusion: Merely orthodontic intrusion and retraction do not solve the problem of a gummy smile, which further requires cortical shaving and crown lengthening can be achieved through plastic periodontal surgery
Case Report
A 35 years old female came with the chief complaint of forwardly placed teeth and excessive gummy display. On intraoral, cephalometric and model analysis examination describes the interdisciplinary with a bimaxillary dentoalveolar protrusion and excessive gingival display (“gummy smile”) or (vertical maxillary excess). The classic treatment approach with these cases includes extraction of first premolars and intrusion of a maxillary anterior segment to correct excessive gingival display caused duet vertical maxillary. The intrusion of anteriors associated with increase buccal cortical bone thickness, and reduced clinical crown length of anteriors.
Introduction
Gingival display during smile can enhance esthetic of the face with in its normal limit of less than 3mm, from its margin up to the upper lip line; if the gingival exposure is more than 3mm from its margin up to the upper lip line referred as gummy smile Allen Garber, et al. [1].
Various researchers have been reported that most common causes are the labial hyperactivity, gingival overgrowth, delayed passive eruption (DPE), vertical maxillary excess (VME), or a combination of them Robbins, Monaco.
Based on the etiological factors Schendel has been classified into dentogingival, dental and skeletal type. Furthermore, in dentogingival type excessive gummy exposure and short clinical crowns are caused by Hyperactivity of the elevator muscle of the upper lip; in dentoalveolar type excessive gummy exposure is caused by Protrusion of upper anterior dentoalveolar complex, and in skeletal type gummy exposure is caused by vertical maxillary excess or maxillary protrusion.
As per the Peck, et al. [2] epidemiological survey, the prevalence rate of gummy smile 7% in young adult male and 14% of an adult female were seen.
Garber and Salam 1996 have been suggested that orthognathic surgery was a classic approach in to enhance esthetic smile in vertical maxillary excess cases. However, Redlich, et al. reported that the maxillary intrusion was the best approach than orthognathic surgeries. Fowler suggested that merely orthodontic intrusion worsen the condition of excessive gingival by shortening clinical crown length [3].
Through this paper, we would like to suggest basic methods of treating excessive gingival display with a management of the soft-tissue to establish clinical crown length and smile line.
History and Etiology
A 35 year old female came with the chief complaint of forwardly placed teeth and excessive gummy display.
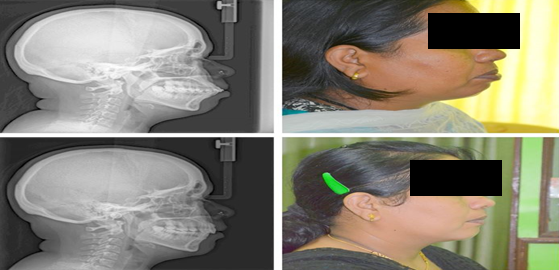
On extra oral examination, lips were incompetence with a hyperactive mental is (Figure 1). Intra-oral examination revealed a severe bimaxillary protrusion, gummy smile, lip incompetence and short clinical crowns. Mild crowding was noted in the lower dentition.

Diagnosis
Skeletally: maxillary protrusion, retrusive mandible (Table 1) Dental: component Class I molar relationship, midlines were coincident. Facial: Convex profile with protrusive lips and Excessive maxillary gingival display when smiling.
| Measurement | Normal value | Pre-treatment |
|---|---|---|
| SKELTAL | ||
| SNA | 82 | 83 |
| SNB | 79 | 76 |
| ANB | 2 | 6 |
| FMA | 23 | 32.3 |
| Z-Angle | 60 | 56.5 |
| DENTAL | ||
| OVERBITE (mm) | 1.8 | 3.5 |
| OVERJET (mm) | 3.5 | 3 |
| FMIA | 59.8 | 59.7 |
| 1-FH | 116 | 114.5 |
| INTER-INCISOL | 123.8 | 125.1 |
| SOFT-TISSUE | ||
| Upper lip -E line | -0.9 | -0.5 |
| Lower lip-Eline | 0.6 | 0.5 |
Table 1: Cephalometric pre-treatment values.
Treatment Objectives
Skeletal components: With maintaining transverse plane, retraction and intrusion of an antero-posterior and vertical component of the maxilla, and mandible respectively has to be done. Dental components: retraction and intrusion of maxillary anterior teeth with maintaining class I molars relationship.
Treatment Plan
As per obtained cephalometric values (Table 2) case has to be set for orthognathic surgery. However, due to patients’ unwillingness case has been planned for camouflage with all first premolars extraction and with the .022 X.028 Roath (dentos bracket) bracket systems. Anchorage preparation with transpalatel arch with a palatal button for intrusion (three-piece intrusion mechanics). To obtain esthetic smile, osteoplasty and periodontal plastic surgery were planned.
| Measurement | Normal value | Pre-treatment | Posttreatment |
|---|---|---|---|
| SKELTAL | |||
| SNA | 82 | 83 | 82.3 |
| SNB | 79 | 76 | 76.5 |
| ANB | 2 | 6 | 5.8 |
| FMA | 23 | 32.3 | 32.5 |
| Z-ANGLE | 60 | 56.5 | 70 |
| DENTAL | |||
| OVERBITE (mm) | 1.8 | 3.5 | 2 |
| OVERJET (mm) | 3.5 | 3 | 2.5 |
| FMIA | 59.8 | 59.7 | 51 |
| 1-FH | 116 | 114.5 | 111.8 |
| INTER-INCISAL | 123.8 | 125.1 | 119.4 |
| SOFT-TISSUE | |||
| Upper lip -E line | -0.9 | 0 | -o.5 |
| Lower lip-Eline | 0.6 | 0.5 | 0.5 |
Table 2: Cephalometric pre-treatment and post-treatment values.
Treatment Progress
After extracting all the first premolars, the .022 X.028 Roath (dentos bracket) bracket system was bonded on maxillary and mandibular teeth with a molar tube from first molars to opposite side first molar, and 014” NiTi, a wire was used in both arch along with lace back and cinch back distal to first molars. The sequence of wire changing was followed every month in a sequence of 014” NiTi, 016” NiTi, and 018” NiTi in the upper and lower arches. The individual arch form was fabricated with bown will’s triangle.
In the fifth month from the start of treatment .019x.025’’ NITI wire was used to check leveling and alignment, after achieving leveling with .019x.025’‘ NITI, .019x.025’’ SS was used to express torque then;//]yujplwalking off canine and segmental retraction.
Once the class I canine relation was obtained with distalization, space was created distal to laterals, was utilized for the intrusion of anterior with three-piece intrusion mechanics (TMA .019X25 wire).
In 18th month intrusion and retraction were achieved with short clinical crowns and gummy exposure, however, clinically increased gummy thickness and more gums exposure were seen as the cortical thickness was increased (Figure 2).

To reduce gum thickness and increase crown length case was set for both osteotomy and crown lengthening (periodontal plastic surgery). Both the procedure was performed by oral surgeon and periodontist (Figure 3,Figure 4).
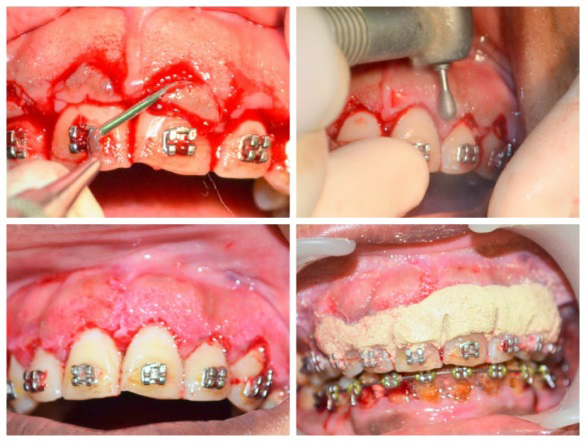

In the 21st month, lateral cephalograms were taken and tracings were done with software and manual superimpositions were done. The permanent retainer was bonded and debonding, a residual composite was removed with ultrasonic tips (Figure 5) compare pre and post treatment.
Discussion
There are two methods in the management of gummy smile (Vertical maxillary excess), orthognathic surgery (Lefort I) and intrusion of anteriors; the intrusion of anteriors causes buccal cortical bone deposition and clinical crown shortening can worsen gummy exposure. Orthognathic surgeries are the complex procedure where patient reluctant to accept such treatment options .
In adults, extrusions of molars are the best method suggested in the management of gummy smile [4], however, extrusion of molars were most difficult and least stable [5]. Hence, in our case, we opted for the intrusion of anteriors for stable then extrusion of molars.
[6] have been suggested that extrusion of molars were the best on- surgical management of a gummy smile with a least stable result and most difficult to achieve. Hence, [7] suggested that intrusion of anteriors can be achieved more easily and gingival countering facilitates to establish its esthetic smile enhancement .
Conventional intrusion mechanics (three piece arch technique) has the major disadvantage of extrusion of molars or the anchorage teeth [8]. Extrusion of maxillary molars results in clockwise rotation of mandible and retrusion chin [9, 10]
In our case we have consolidated the lateral segment till canine and palatal button was incorporated and standard protocol for intrusion such as the optimum force of [8] 80 gm of intrusion force was used on 4 upper incisors and 3 mm of true intrusion [9, 11] was obtained without notable root resorption or vitality problems during the active treatment period to overcome the associated disadvantage.
The concepts of buttress bone formation illustrate that reinforcing bone formation to a buccal alveolar bone in response to heavy occlusal forces [12]. Most of the studies have suggested that such bone formation occurs with the purpose of reinforcing bone trabeculae Matthews, et al. Furthermore, mechanical stimulus significant effect on bone remodeling; when higher mechanical loads occur (0.25– 0.40%), bone hypertrophy occurs with increased lamellar bone Garg, et al.
In our case buttress bone formation occurred due to intrusion mechanism, resulting into a short clinical crown and increased gingival display may be due to gingival hyperplasia. Thus, to establish pleasing smile and occlusion; both periodontal plastic surgery (genioplasty) and anterior osteoplasty were performed Figures 6 & 7.


Conclusion
In conclusion, the buttress bone formation and short clinical crown were the associated infrequent side effect to the orthodontic intrusion of anterior teeth. In order to establish pleasing smile, a proposed surgical protocol has to be achieved to increase clinical crown and to reduce excessive gingival exposure. Furthermore, an intrusion of anterior results in dropping of the upper lip without tension suggesting that the technique presented is a useful resource for esthetic improvements in gummy smile patients.
References
-
Garber DA, Salama MA (1996) The aesthetic smile: Diagnosis and treatment. Periodontology (11): 18-28.
-
Peck S, Peck L, Kataja M (1992) The gingival smile line. Angle Orthod (62): 91-100.
-
Fowler P (1999) Orthodontics and orthognathic surgery in the combined treatment of an excessively gummy smile. N. Z. Dent. J 95(420): 53-54.
-
Engel G, Cornforth G, Damerell J, Gordon J, Levyet P, et al. (1980) Treatment of deep-bite cases. Am J Orthod 77(1): 1-13.
-
McDowell EH, Baker IM (1991) The skeletodental adaptations in deep bite correction. Am J Orthod 100(4): 370-375.
-
Ricketts RM, Bench RW, Gugino CF, Hilgers JJ (1979) Bioprogressive Therapy. Denver, Co: Rocky Mountain Orthodontics 11(10): 661-671.
-
Proffit WR, Fields HW (2000) Contemporary Orthodontics. 3rd (Edn.), St. Louis, Mo: Mosby Year Book pp: 240-293.
-
Burstone CR (1977) Deep overbite correction by intrusion. Am J Orthod 72(1): 1-22.
-
Melsen B, Agerbaek N, Markenstam G (1989) Intrusion of incisors in adult patients with marginal bone loss. Am J Orthod Dentofacial Orthop 96(3): 232-24.
-
Burstone CJ, Pryputniewicz RJ (1980) Holographic determination of centers of rotation produced by orthodontic forces. Am J Orthod (77): 396-409.
-
Gianelly A, Goldman HM (1971) Biologic basis of orthodontics. Philadelphia: Lea andFebiger.
-
Glickman I, Smulow JB (1965) Buttressing bone formation in the periodontium. J Periodontol 36(5): 365- 370.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey