Mucoepidermoid Carcinoma of the Thyroid Gland with Lymphovascular Invasion A Case Report
Mucoepidermoid carcinomas (MECs) are generally found in salivary glands, but they have also been mentioned in other organs such as the larynx, esophagus, and breast. Mucoepidermoid carcinoma (MEC) of the thyroid is a very rare and lowgrade indolent neoplasm. In past reports of the thyroid MEC, only nine cases were described as poor prognosis. We here present a case of a female patient, 29 years old, euthyroid, no chronic medical illness, no drug history, non-smoker; she is married and has 3 children. She presented to the hospital with painless neck swelling. Fine needle aspiration cytology (FNAC) showed mixture of squamoid cells and pale enlarged cells with cytoplasmic vacuoles and devoid of colloid with possible pseudo inclusions. (Consistent with Hűrthle cell neoplasm). Lt hemithyroidectomy was done and sent to histopathology for diagnosis. Histopathology analysis revealed a microscopic focus of intrathyroidal intermediate-grade MEC within the Lt lobe nodule. The patient was scheduled for completion thyroidectomy with midline cervical lymphadenectomy after metastatic work-up was done. The present case is a rare presentation of intermediate-grade thyroidal MEC
Introduction
Mucoepidermoid carcinoma (MEC) commonly arises in the salivary glands [1] but also in the esophagus, respiratory tract, pancreas and breast [2]. In rare cases, MEC arises in the thyroid gland. Theoretically, MEC in thyroid gland originates from remnants of the ultimobranchial body, remnants of salivary gland intrathyroidal, follicular epithelium, parafollicular C cells, thyroglossal duct and parathyroid [3]. According to histologic features, MEC is classified as low, intermediate or high grade [4] with most cases being low grade. MEC of the thyroid were first described by Rhatigan RM, et al. [5] in 1977 and since then only 46 cases have been reported in the thyroid gland with poor prognosis in nine cases [6]. Herein, we present a case of MEC in the thyroid gland with lympho-vascular invasion.
Case
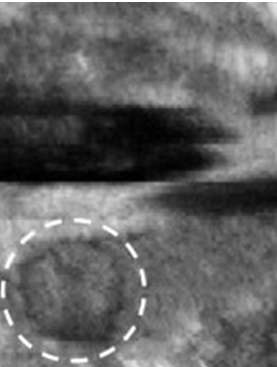
Approval of Minia College of Medicine institutional Ethics Committee was obtained. A 29 years old Yemeni female patient, euthyroid, with no chronic medical illness, no drug history, non-smoking; she is married and has 3 children. She visited our hospital because of painless neck swelling that persisted for 6 months. The patient had no previous history of neck irradiation, and her family history was negative for any form of thyroid disease. Clinical examination of the neck revealed a solitary left lobe thyroid nodule with no palpable cervical LNs. On neck ultrasound, a 2 cm hypoechoic mass was identified in the left lobe of the thyroid gland (Figure 1).
Routine blood tests and thyroid function tests were also within normal limits. Sonar guided fine needle aspiration was done and demonstrated mixture of squamoid cells and pale enlarged cells with cytoplasmic vacuoles and devoid of colloid with possible pseudo inclusions. An impression of possible Hűrthle cell neoplasm was made. Left hemi- thyroidectomy was conducted under general anesthesia (Figure 2).

Histopathological examination revealed a microscopic focus of intrathyroidal intermediate grade MEC within the 2 cm nodule, however, no papillary features were identified. Lympho-vascular invasion was seen, as well as masses of tumor cells invading blood vessels (Figure 3).
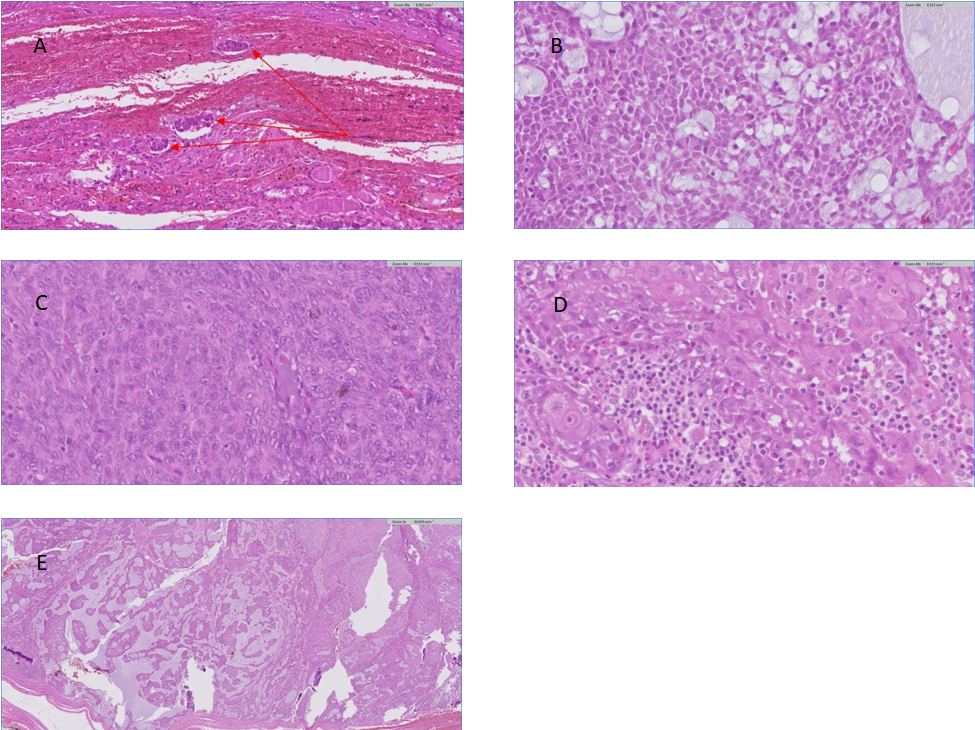
Figure 3: Histological findings. A: Lympho-vascular invasion, B: Vacuolated cells are located within epidermoid cells, C: Mitoses are frequently identified, D: Large irregular nests or solid sheets of tumor cells with prominent nucleoli and intracellular keratinization, E: large irregular nests of epidermoid cell containing glandular spaces with mucin.
Metastatic work up revealed no extra-thyroid extension. A completion thyroidectomy was done with midline cervical lymphadenectomy. Postoperative specimen revealed no residual malignant foci inside the thyroid with no lymph nodes metastases.
Discussion
MEC is a rare malignant neoplasm in the thyroid gland, with approximately 46 cases reported in the literature [6]. According to those 46 reported cases, occurrence of MEC is more commonly in females with patients age at time of diagnosis ranging from 10 to 91 years [1]. Patient with thyroid MEC show symptoms of painless, unilateral mass in the thyroid with reduced uptake in thyroid scans. The incidence rate of extrathyroidal extension is 14.8%, and approximately 42.2% of patients have nodal metastases. Because MEC could arise from de-differentiation of pre-existing well-differentiated papillary and follicular thyroid cancer [3]. Definite origin of MEC in the thyroid gland is uncertain. Some authors have suggested that MEC can originate from metaplastic dedifferentiation of papillary, follicular, or oncocytic thyroid carcinoma [3]. The microscopic picture of MEC in the thyroid gland is the same as in the salivary gland. Cords, solid sheets, or nests of interweaved mucous and epidermoid cells are arranged in the fibrotic stroma. The epidermoid cells connected together by bridges and undergo keratinization. The mucous cells are foamy cell with vacuolated cytoplasm and eccentric nucleus [7]. The grading system for thyroid MEC has not yet been settled. Thyroid MEC is considered a low-grade malignancy with rare mitosis and necrosis. The prognosis is favorable in most cases but cases with poor prognosis have also been recorded [6]. For purposes of prognosis, there has been an attempt, begun by the originators of the diagnostic term, to divide mucoepidermoid tumors into classes based on their histologic appearance [8]. Healy W, et al. [9, 10] developed this concept further and separated mucoepidermoid tumors into three grades of malignancy: low-grade, high-grade, and intermediate. The overall survival for high grade MEC is approximately 50%, compared to about 90% of intermediate and low-grade MECs [11]. Generally, the well-differentiated or low-grade carcinomas tend to have many cystic spaces lined by a single layer of mucous secreting epithelium. Epidermoid and intermediate cells are sparse and pleomorphism and mitoses are nearly absent. The present case is of intermediate type of MEC forming solid nests of cells and more cellular than low grade tumors and have a greater preponderance of epidermoid and intermediate cell types with fewer cystic spaces. The cells have slight to moderate pleomorphism and occasional mitoses. Most of the malignant cells have a squamous appearance with prominent nucleoli, intercellular bridges and keratin pearls. However, the intermediate cells with moderately increased nuclear/cytoplasmic ratio and centrally located nuclei are the least diagnostic cells of MEC. The differential diagnosis of the current case includes differentiated thyroid carcinoma, fibrosing Hashimoto thyroiditis, papillary thyroid with squamous metaplasia, primary or metastatic squamous cell carcinoma and MEC. It is important to have a high index of suspicion and a specific diagnosis when dealing with thyroid lumps.
Conclusion
Mucoepidermoid carcinoma is a rare malignancy of the thyroid gland with only 46 cases reported to date. Although MEC of the thyroid is usually considered a low-grade malignant tumor, several cases with adverse outcomes have been reported. According to the past reports, only nine cases of thyroid MEC with poor prognosis were described. Herein, we have described a very rare case of thyroid MEC with lympho-vascular invasion with a suspected poor prognosis.
References
-
Le QV, Ngo DQ, Ngo QX (2019) Primary mucoepidermoid carcinoma of the thyroid: a report of a rare case with bone metastasis and review of the literature. Case Rep Oncol 12(1): 248-259.
-
Bhandarkar ND, Chan J, Strome M (2005) A rare case of mucoepidermoid carcinoma of the thyroid. Am J Otolaryngol 26(2): 138-141.
-
Prichard RS, Lee JC, Gill AJ, Sywak MS, Fingleton L, et al. (2012) Mucoepidermoid carcinoma of the thyroid: a report of three cases and postulated histogenesis. Thyroid 22(2): 205-209.
-
Goode RK, Auclair PL, Ellis GL (1998) Mucoepidermoid carcinoma of the major salivary glands: clinical and histopathologic analysis of 234 cases with evaluation of grading criteria. Cancer 82(7): 1217-1224.
-
Rhatigan RM, Roque JL, Bucher RL (1977) Mucoepidermoid carcinoma of the thyroid gland. Cancer 39(1): 210-214.
-
Lee K, Mirza O, Dobbs S, Jayaram S (2020) Poorly differentiated mucoepidermoid carcinoma of the thyroid. BMJ Case Rep 13: e236539.
-
Vazquez RF, Otal SC, Argueta MO, Galera RH, Gonzalez CR (2000) Fine needle aspiration cytology of high grade mucoepidermoid carcinoma of the thyroid: a case report. Acta Cytol 44: 259-264.
-
Stewart RW, Foote FW, Becker WF (1945) Mucoepidermoid tumors of the salivary glands. Ann Surg 122(5): 823-844.
-
Healey WY, Perzin KH, Smith L (1970) Mucoepidermoid carcinoma of salivary gland origin: Classification, clinicopathologic correlation, and results of treatment. Cancer 26: 368.
-
Foote FW, Frazeil EL (1953) Tumors of the major salivary glands. Cancer 6: 1065.
-
McHugh CH, Roberts DB, El-Naggar AK, Hanna EY, Garden AS, et al. (2012) Prognostic factors in mucoepidermoid carcinoma of the salivary glands. Cancer 118(16): 3928- 3936.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey