An Updated Role of Anastrozole in Male Factor Infertility for Avoidance of Need for Assisted Reproductive Technology ART A Short Communication
Male factor infertility causes infertility in about 50% couples. Aromatase hampering agents, like anastrozole restricts the transformation of testosterone (T) to estradiol (E2), minimize negative hampering on pituitary accessibility, and escalate endogenous Gn generation. Aromatase hampering agents have been offered historically to patients with a T: E2 ratio <10. Anastrozole, a more selective hampering agent in contrast to prior agents, has been illustrated to decrease serum E2 quantities and improvement of semen parameters in men with a low T: E2 ratio . Despite, escalated utilization of anastrozole for the treatment of infertile men with escalated peripheral estrogen, it is uncertain if a broader cohort may benefit also from therapy. For corroborating that Naelitz BD, et al. revealed in a multi institutional retrospective cohort study with regards to infertile men with the objective to evaluate the anticipative factors for World Health Organization -sperm concentration category (WHO-SCC)upgrade in case of male patients receiving anastrozole treatment. Their observations were that anastrozole Initiation was correlated with decreased serum estradiol (E2), escalated serum gonadotropin (Gn) quantities, and clinical improvement of semen paradigms in approximately 50% of infertile men. Baseline generation of sperms and greater T: LH ratios anticipated an upgrade of WHO-SCC. E2 quantities, E2: T ratio, and BMI revealed poor anticipative power in this cohort. Men with pretreatment azoospermia displayed poor response to anastrozole needing other treatment modalities. Non-azoospermic infertile men with a T-LH ratio ≥100 (in addition to a lesser degree those with a ratio <100) might gain advantage from treatment with anastrozole and get counseled regarding the anticipated probability of a clinically significant enhancement in semen paradigm. This might expand the availability of different therapies to couples who present with male factor infertility also aid in a trial of lesser invasive / costly fertility treatments.
Introduction
Male factor infertility aids in the infertility of any couple in about 50% instances. Although the etiology remains uncertain, this escalated prevalence continues to be unexplained in 40-70% of couples [1, 2]. Utilization of empiric medical treatment for idiopathic male infertility has the objective of augmentation of spermatogenesis through modulating of the hypothalamic-pituitary-gonadal hormone axis canonically, via the utilization of selective estrogen receptor modulators, aromatase hampering agent (AIs), as well as /or exogenous gonadotropins(Gns) [3, 4, 5]. Aromatase hampering agents for instance in view of anastrozole restricts the transformation of testosterone (T) to estradiol (E2), minimize negative hampering on pituitary accessibility, in addition to escalate endogenous Gn generation [1, 6]. Aromatase hampering agents have been offered historically to patients with a T-E2 ratio <10 [7, 8]. Anastrozole, a more selective hampering agent in contrast to prior agents, has been illustrated to decrease serum E2 quantities along with improvement of semen parameters in men witha low T-E2 ratio [9, 10]. A recent meta-analysis observed that the use of AIs was associated with improved sperm quantities in addition to endocrine profiles [11]. Anastrozole might be further advantageous for those also with morbid obesity who express aromatase at greater quantities [12]. Despite, escalated utilization of anastrozole for the treatment of infertile men with escalated peripheral estrogen, it is uncertain if a broader cohort may benefit also from therapy.
Naelitz BD, et al. [13], revealed in a multi institutional retrospective cohort study with regards to infertile men with the objective to evaluate the anticipative factors for World Health Organization-sperm concentration category (WHO-SCC)upgrade in case of male patients receiving anastrozole treatment. Anastrazole portrays a selective aromatase hampering agent, that canonically has been given to males having testosterone: estrogen (T:E)ratios less than 10 [14, 15]. Despite, utilization of aromatase hampering agents have been advocated by the Guidelines of American Urological Association, just follicle stimulating hormone (FSH) analogues are at present corroborated for use in males having so called idiopathic infertility [6]. Nevertheless, accessibility towards these strategies continue to pose a challenge in addition to entail remarkable expenditure. In a recent study by Naelitz BD, et al. [13], who retrospectively performed assessment of 90 men having infertility who got anastrozole treatment in addition to had a RSA(routine semen analysis) prior to as well as subsequent to anastrozole treatment. They had their classification in the form of responders along with non responders dependent on the existence of upgrade of WHO-SCC [13].
Around 50% of the patients had the experience of an upgrade of WHO-SCC in addition to12% had the experience of a WHO-SCC down grade. A significant percentage of patients (29%) upgraded to normospermia which contributed to the utilization of intrauterine insemination (IUI) in 31% of the patients. Moreover 25% of the patients having robust oligozoospermia upgraded to sperm quantities of greater than 15M/ml, probably contributing to the probability of conceiving by natural manner. Despite, baseline E in addition to body mass index (BMI) did not anticipate upgrade of WHO-SCC, a T: LH ratio greater than 100 along with baseline no azoospermia points to them being anticipative factors for upgrade of WHO-SCC (Figure1).
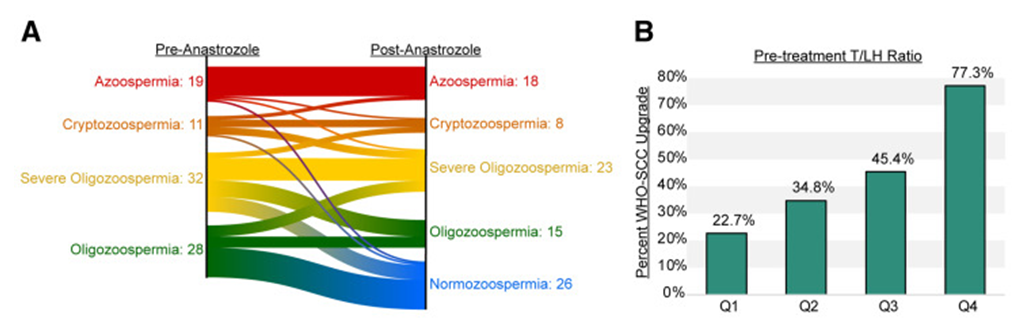
Figure 1: Courtesy ref no-13-The testosterone-to-luteinizing (T-LH) hormone ratio predicts response to anastrozole treatment, according to an upgrade in the World Health Organization sperm classification category (WHO-SCC). (A) 46% (n = 41/90) of the multi-institutional cohort experienced a WHO-SCC upgrade after initiating anastrozole therapy. Non responders included the 42% (n = 38/90) of the cohort that remained in the same WHO-SCC group and the 12% (n = 11/90) of the cohort who experienced a downgrade after the treatment. (B) Higher levels of the T-LH ratio identify those with a clinically significant response to anastrozole, with the highest quartile (Q4) being associated with a 77.3% incidence of WHO-SCC upgrade.
Naelitz T, et al. [13] had conclusions drawn regarding how anastrozole might possess greater utilization in case of male patients having infertility apart from those having obesity or a reduced T: E ratio. Akin to that, their outcomes illustrated that those possessing lesser gonadotropins prior to treatment along with certain baseline sperm generation might possess greater probability of being responsive to anastrozole treatment. Lastly, the importance of T: E ratio was deduced to make a decision with regards to patients having a T:LH ratio greater than 100 possess functional Leydig along with sertoli cells which need extra stimulation (Figure2).
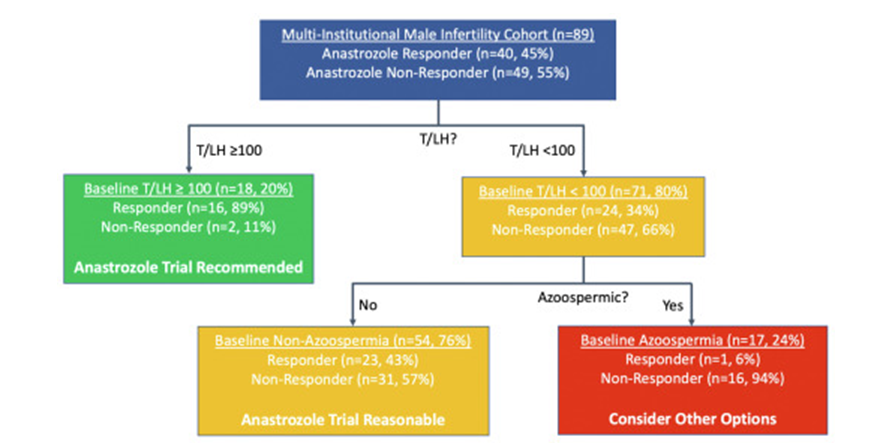
Figure 2: Courtesy ref no-13-The testosterone-to-luteinizing hormone (T-LH) ratio and baseline nonazoospermia identify appropriate candidates for the initiation of anastrozole. Recursive partitioning analysis identified the baseline T-LH ratio with a cutoff ≥100 as the best initial differentiator for selecting patients most likely to experience a World Health Organization sperm classification category (WHO-SCC) upgrade. The cohort was further partitioned by identifying those unlikely to respond to treatment, which included those with baseline azoospermia. Nonazoospermic patients with a baseline T-LH ratio <100 constituted the final fraction of the cohort. Under the assumption that all patients with nonazoospermia received a trial of anastrozole and all patients with azoospermia avoided treatment, this partitioning model was 98% sensitive and 33% specific for WHO-SCC upgrades. Notably, one patient in the cohort did not possess a baseline LH measurement and was excluded from partitioning analysis.
Despite, this ratio was observed to possess 98% sensitivity for anticipating WHO-SCC upgrade, however its specificity was just 33%.Hence it makes it imperative to perform future prospective studies for estimating the clinical usefulness with regards to assessment of infertile males. Despite, these outcomes are interesting in addition to possess the probability of altering clinical scenario with regards to men having infertility,one has to take into account the fashioning of the study .This was a multi institutional retrospective cohort study.Just a single RSA performed prior to treatment restricted the evaluation of the correct semen analysis prior to treatment.Similarly,12% patients had an experience of a WHO-SCC down grade with anastrazole treatment. Naelitz T, et al. [13] advocated requirement of an RSA repeated regarding clarification if the finding takes place secondary to a natural difference in investigating RSA. Furthermore there was illustrated heterogeneity amongst the institutions which participated in correlation with age, BMI in addition to dosage of anastrozole. Though clarificationwas given by these authors that once addition of institution was done in the form of an anticipative variable it did not significantly influence how the model performed. Lastly the primary end point with regards to the study was for WHO-SCC, that works in the form of an indirect infertility marker. Nevertheless, it getting acknowledged that this was a retrospective study along with no pregnancy rates in addition to live birth rates (LBR) outcomes availability, this end point mirror a substitute which had a clinical meaning.
The outcomes of this study are significant in numerous manners. Canonically, utilization of anastrazole has been done only for men having obesity with diminished T:E ratios. Nevertheless, the illustrated importance of the T:LH ratio greater than 100 aids in probable expanding this agent’s utilization which is off label regarding male factor infertility as well as might aid assisted reproductive technology(ART) patients in addition to their partners in prevention of expensive ART. Greater work in the future as a prospective clinical trial needs to be performed with regards to corroborating the outcomes of this study along with enhancement of American Society Guidelines which are advocated by team headed bythe experienced Schlegel PN’s team [16]. Furthermore utilization of anastrozole in patients having non obstructive azoospermia was not validated by the outcomes of this study. These outcomes give addition to the restricted knowledge with regards to pharmacologically manipulating aromatase hampering in males having presentation as oligozoospermia [17].
Conclusion
Anastrozole Initiation was correlated with decreased serum estradiol (E2) quantities, escalated serum gonadotropin (Gn) quantities, and resulted in clinical improvement of semen paradigms in approximately 50% of infertile men. Baseline generation of sperms in addition to greater T: LH ratios anticipated an upgrade of WHO- SCC. E2 quantities, E2: T ratio, as well as BMI revealed poor anticipative power in this cohort. Men with pretreatment azoospermia displayedpoor response to anastrozole along with need other treatment modalities. Non-azoospermic infertile men with a T-LH ratio ≥100 (in addition to a lesser degree those with a ratio <100) might gain advantagefrom treatment with anastrozole as well as get counseled regarding the anticipated probability of a clinically significant enhancement in semen paradigm. This might expand the availability of different therapies to couples who present with male factor infertility as well as aid in a trial of lesser invasive or lesser costly fertility treatments.
References
-
Chehab M, Madala A, Trussell JC (2015) Onlabel and off label drugs used in the treatment of male infertility. Fertil Steril 103(3): 595-604.
-
Tuttelmann F, Ruckert C, Ropke A (2018) Disorders of spermatogenesis: perspectives for novel genetic diagnosis after 20years of unchanged routine.Med Genet 30: 12-20.
-
Minhas S, Bettocchi C, Boeri L, Capogrosso P, Carvalho J, et al. (2021) European Association of Urology guidelines on male sexual and reproductivehealth: 2021 update on male infertility. Eur Urol 80(5): 603-20.
-
Ko EY, Siddiqi K, Brannigan RE, Sabanegh ES (2012) Empirical medical therapyfor idiopathic male infertility: a survey of the American Urological Association. J Urol 187(3): 973-978.
-
Rittenberg V, El-Toukhy T (2010) Medical treatment of male infertility. Hum Fertil(Camb) 13(4): 208216.
-
Thaker H, Ko EY, Sabanegh ES, Brannigan RE, Alukal JP, et al. (2020) Empiricalmedical therapy for idiopathic male infertility. F S Rep 1(1): 15-20.
-
Gregoriou O, Bakas P, Grigoriadis C, Creatsa M, Hassiakos D, et al. (2012)Changes in hormonal profile and seminal parameters with use of aromataseinhibitors in management of infertile men with low testosterone to estradiolratios. Fertil Steril 98(1): 48-51.
-
Helo S, Ellen J, Mechlin C, Feustel P, Grossman M, et al. (2015) A randomizedprospective double-blind comparison trial of clomiphene citrate and anastrozole in raising testosterone in hypogonadal infertile men. J Sex Med 12(8): 1761-1769.
-
Shoshany O, Abhyankar N, Mufarreh N, Daniel G, Niederberger C (2017) Outcomesof anastrozole in oligozoospermic hypoandrogenic subfertile men. Fertil Steril 107(3): 589-594.
-
Guo B, Li JJ, Ma YL, Zhao YT, Liu JG (2022) Efficacy and safety of letrozole oranastrozole in the treatment of male infertility with low testosterone-estradiol ratio: a meta-analysis and systematic review. Andrology 10(5): 894-909.
-
Shah T, Nyirenda T, Shin D (2021) Efficacy of anastrozole in the treatment of hypogonadal,subfertile men with body mass index R25 kg/m2. Transl Androl Urol 10(3): 1222-1228.
-
Yang C, Li P, Li Z (2021) Clinical application of aromatase inhibitors to treat maleinfertility. Hum Reprod Update 28(1): 30-50.
-
Naelitz BD, Jiang T, Munoz-Lopez C, Sigalos JT, Modiri N, et al. (2023) Testosterone and Luteinizing hormone predict semen parameters improvement in infertile men with anastrazole. Fertil Steril 120(4): 746-754.
-
Raman JD, Schlegel PN (2002) Aromatase inhibitors for male infertility. J Urol 167(2): 624-629.
-
Shishany O, Abhyankar N, Mufarreh N, Daniel G, Niederberger C (2017) Outcomes of anastrazole in oligozoospermic hypoandrogenic sub fertile men. Fertil Steril 107(3): 589-594.
-
Schlegel PN, Sigman N, Collura B, Di Jonge CJ, Eisenberg ML, et al. (2021) Diagnosis and treatment of infertility in men:AUA/ASRM Guidelines PartII. J Urol 205(1): 44-51.
-
Deebel NA, Ramaswamy R (2023) Utilization of anastrazolein male infertility: potential for expanded use. Fertil Steril 120(4): 810.
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey