Motion Artifact Mimics Subdural Hemorrhage on CT Scans: A Case Series
The aim of this paper is to show a common phenomenon seen in brain computed tomography scans. This phenomenon is seen when the patient slightly moves during the brain scan which creates a motion artifact that appears like pathology and the radiologists might misdiagnose the case as a false positive case. A slight motion artifact appeared as a subdural hemorrhage in five cases. Some of these cases came to the hospital as road traffic accident cases, while others have only suffered a chronic headache. In this case series, five cases are presented, scanned again to rule out any pathology, and these cases are discussed in this paper to find any common pattern among these cases.
Introduction
Motion artifact can happen when the patient is not well instructed, suffer from phobia (claustrophobic), in uncomfortable situation, has a severe pain, or has low level of consciousness. New immobilization techniques have been proposed before as a head holder for CT scanners [1]. There are published papers about motion artifact mimicking subarachnoid and inter-ventricular hemorrhage on different MRI scan pulse sequences [2]. Motion artifact and streak artifact can mimic subdural hemorrhage according to many papers [3, 4, 5]. A key point that could help in identifying the motion artifact from subdural hemorrhage is that mass effect and shift of the ventricles which can be seen, when there is a hemorrhage. In brain CT scans, due to the lack of involuntary movement like in the chest (heart movements) and in the abdomen (bowel movements), the gantry rotation of CT scan will be slower compared to the chest because involuntary movement is not a concern in brain scans; therefore; motion artifact occurs [6]. This slow motion will reduce the image quality of the brain CT scan [7]. This slow gantry motion will reduce the temporal resolution when the patient moves or contrast media bolus is injected which will cause motion artifact [8]. In a study of 77 patients using CT scan, motion artifact occurs in 12% of patients and it causes interpretation impairment in 8% of the patients’ CT scans [8]. Motion artifact has been reported in most of CT applications [9]. Loss of reconstruction resolution has been reported to be associated with patients’ movements by many authors [10, 11, 12, 13, 14, 15, 16]. Many solutions have been proposed to eliminate motion artifact [1, 17, 18, 19, 20].
The 1st Case
A 27-year-old male patient came to the emergency department after he was involved in a Motor Vehicle Accident (MVA). A CT brain was requested for the patient which revealed a subdural hemorrhage on the right side see (Figure 1). The subdural hemorrhage appears disconnected into many segments, so an MRI scan was requested to rule out any hemorrhage. A brain MRI scan was done which revealed no subdural hemorrhage on the right side, but a small contusion was found on the left hemisphere see (Figure 1).
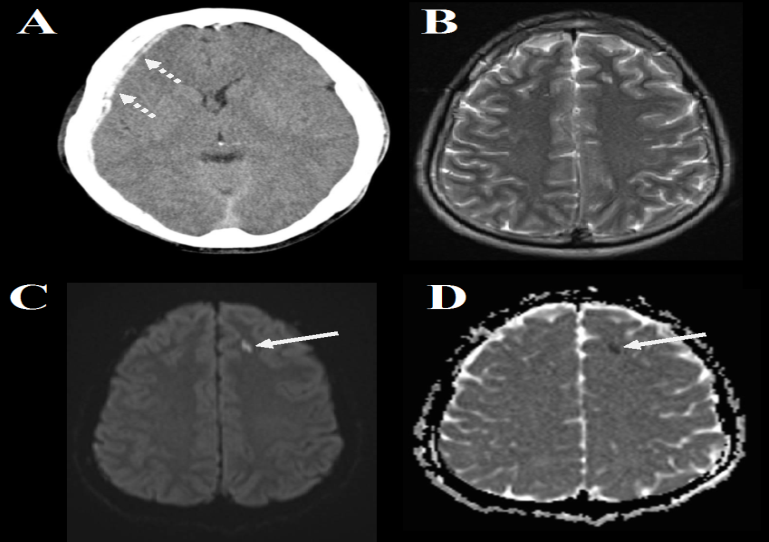
Figure 1: A 27-year-old male patient was involved in a MVA and underwent scans presented as the following; A- an axial brain CT shows a subdural hemorrhage (the intermittent arrow), B- a brain MRI T2 shows no subdural hemorrhage, C- a brain MRI diffusion shows an inter- parenchymal high intensity foci most likely is a contusion (the continuous arrow), and D- a brain MRI ADC map shows a foci with restricted diffusion on the left side which could be a contusion (the continuous arrow).
The 2nd Case
A 51-year-old male patient suffered from an episode of epilepsy and he fell down and on his head. A CT brain was requested from the emergency room to rule out any bleeding. The patient was not very responsive and even under a heavy dose of diazepam the patient kept moving which created this sign of subdural hemorrhage. Luckily, one of the sections showed the skull bone separated into two which indicated motion artifact rather than a subdural hemorrhage. An MRI was requested, but the patient kept moving, so the patient was admitted under observation for 48 hours. After 48 hours, the patient was fine and he was discharged upon his request (Figure 2).
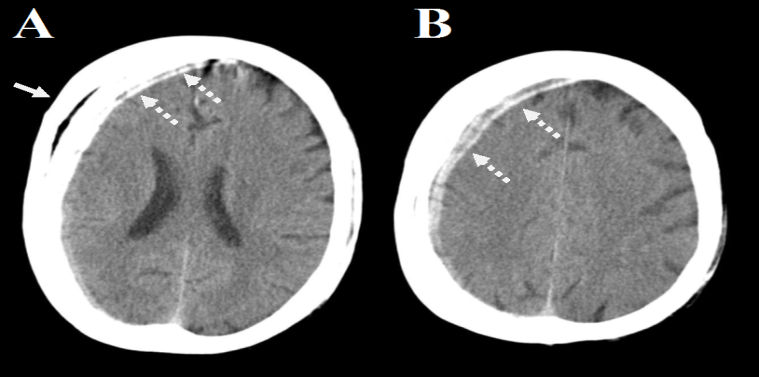
Figure 2: A 51-year-old male patient suffered an episode of epilepsy and he underwent a CT scan which shows the following; A- an axial brain CT scan shows what looks like as a subdural hemorrhage (the intermittent arrow) and the right part of the skull is seen split into two which is due to the slight movement (the continuous arrow), and B- a brain axial scan shows what appears to be a subdural hemorrhage (the intermittent arrow). The case appears normal and due to the fact that patient is irresponsive, no other imaging was done and he was admitted under observation for 48 hours then discharged after he improved.
The 3rd Case
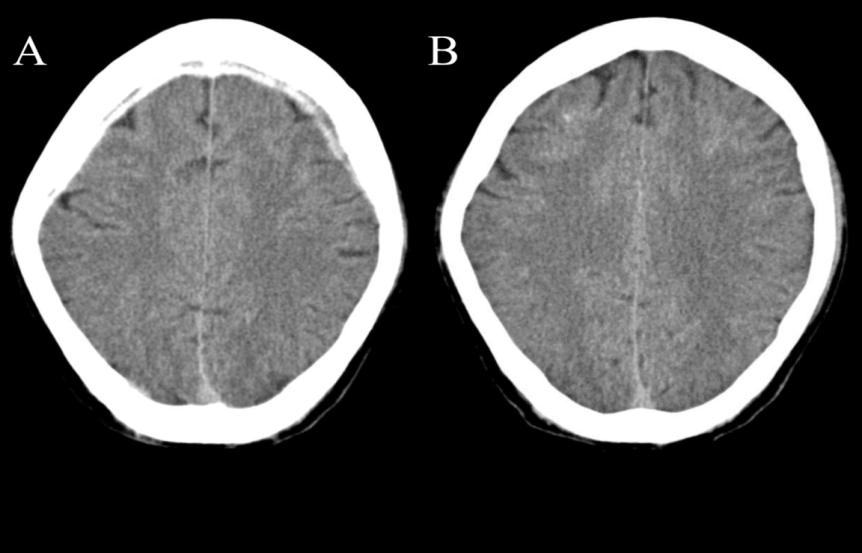
A 19-year-old female patient fell down from 2 meters height to the ground. She was brought to the hospital and a CT scan was requested for the head and the body. The whole body was normal, but the brain CT was abnormal. A subdural hemorrhage was seen in the right hemisphere of the brain see (Figure 3). The CT scan was repeated to check the subdural hemorrhage if it will be detected again? The second brain CT showed no abnormality see (Figure 3), so a brain MRI was requested to do a double check on the patient. The brain MRI did not reveal any abnormality see (Figure 3).
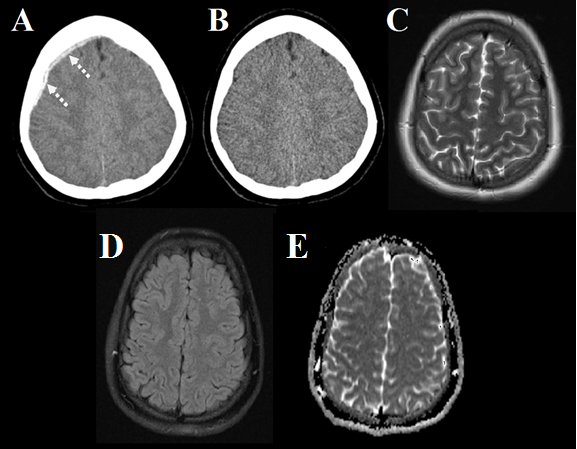
Figure 3: A 19-year-old female patient who fell down and underwent brain scans which shows the following; A- an axial brain scan shows a subdural hemorrhage on the right side (the intermittent arrow), B- a repeated axial brain CT scan shows a normal brain, C- a brain MRI T2 image shows no abnormality, D- a brain MRI FLAIR image shows no abnormality, and E- a brain MRI ADC map shows no abnormality.
The 4th Case
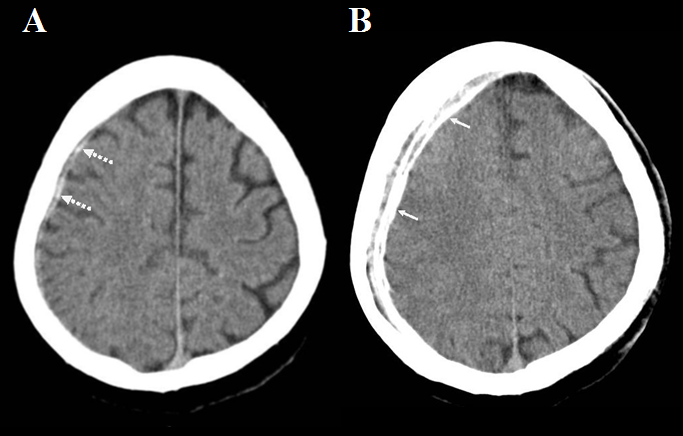
A 44-year-old male patient was involved in a Road Traffic Accident (RTA) and the emergency department requested a PAN CT. The images showed a white area looks like a subdural hemorrhage on the right side. The other section of the brain CT scan showed a blurry skull bones due to movement (Figure 4).
The 5th Case
A 55-year-old male patient came to the emergency room complaining of a severe headache and blurry vision. A CT scan was done and the patient moved slightly which appeared as a prefrontal lobe subdural hemorrhage. On another section, no prefrontal lobe’s abnormality which indicates it most likely to be a motion artifact rather than a haemorrhage (Figure 5).
Discussion
Notice all five cases have the same issue in the right frontotemporal side which could be a machinery problem (i.e. artifact). But the patients did shift their brain to the right side as seen in cases from 1 to 4 and in one case the patient moved anteriorly (i.e. case 5). In order to differentiate them from subdural hemorrhage cases, the following criteria must be followed:
- The motion artifact is dotted non continuous white strip, while the subdural hemorrhage is hyperdense (acute setting) continuous area which might have a swirl sign;
- The motion artifact does not push the brain away (i.e. no mass effect), while the subdural hemorrhage pushes the brain (i.e. mass effect);
- The motion artifact has no brain swelling, while subdural hemorrhage might have a brain swelling;
- The motion artifact has a HU of the skull bones, while subdural hemorrhage has the blood HU;
- The motion artifact might show a blurry image slice due to movement which in subdural hemorrhage cases might show some patients move too due to a severe headache and pain, but no blurry images should be accepted.
Motion artifact have many forms including; streaking, blurry, ghosting, internal structure deforming, and harsh image distortion [21]. New technologies used to eliminate the motion artifact are: Convolutional Neural Network (CNN) and Deep Residual Network (DRN) [22, 23]. Both methods induced new issues; the CNN increased the edge enhancement in MRI images, while DRN ignores some structures’ contrast [22, 23]. In angiography imaging, a Generative Adverbial Networks (GAN) module was used and it shows a little bit of progress in reducing motion artifact in coronary imaging [24]. A new proposed algorithm used in head CT scanning, claim to show normalizations of images, but the presented image in the paper still contain motion artifact over the right temporal lobe [25]. Sedation is used with pediatric patient who undergo CT scan [26], usually diazepam, but it might help with some young patients and be useless with hyperactive children.
Limitations
This is a case series which has a sample size of 5 cases and it did not examine many patients. Other severe motion artifact cases were not included in the paper due to the bad quality of the images. Some cases of missing brain structures due to the fast movement of the patients were not included as well. Some of the cases were not fully conscious.
Conclusion
Motion artifact can mimic the subdural hemorrhage appearance, but repeating the CT scan or do a brain MRI
can rule out the subdural hemorrhage. The motion artifact will necessitate a repeat and the repeat will increase the radiation dose. The skull blurriness is an indication that this is a motion artifact. Patient immobilization techniques must be improved to grantee a higher image quality and lower radiation dose. Sedition, immobilization techniques, explaining to the patients (i.e. well informed patient), ask one of the relatives to hold the patients still and make them covered by lead apron, all are methods used to help to prevent motion artifact, but still motion artifact is affecting many scans, for the length of the scans in general.
References
-
Alahmari A (2022) A Proposal of a Head Holder for CT Scan Tables: A New Fixation Design. Austin J Radiol 9(2): 1191.
-
Cianfoni A, Martin MG, Du J, Hesselink JR, Imbesi SG, et al. (2006) Artifact Simulating Subarachnoid and Intraventricular Hemorrhage on Single-Shot, Fast Spin- Echo Fluid-Attenuated Inversion Recovery Images Caused by Head Movement: A Trap for the Unwary. AJNR Am J Neuroradiol 27(4): 843-849.
-
Lim M, Kheok SW, Lim KC, Venkatanarasimha N, Small JE, et al. (2019) Subdural Haematoma Mimics. Clin Radiol 74(9): 663-675.
-
Bordia R, Le M, Behbahani S (2021) Pitfalls in the Diagnosis of Subdural Hemorrhage-Mimics and Uncommon Causes. J Clin Neurosci 89: 71-84.
-
Haar FL, Lott TM, Nichols P (1977) The Usefulness of CT Scanning for Subdural Hematomas. Neurosurgery 1(3): 272-275.
-
Ginat DT, Gupta R (2014) Advances in Computed Tomography Imaging Technology. Annu Rev Biomed Eng 16(1): 431-453.
-
(2008) Mobile Computed Tomography Evaluation of the NeuroLogica Cere Tom. Health Devices 37(11): 325-342.
-
John S, Stock S, Cerejo R, Uchino K, Winners S, et al. (2016) Brain Imaging Using Mobile CT: Current Status and Future Prospects. J Neuroimaging 26(1): 5-15.
-
Linney NC, Gregson PH (2001) Organ Motion Detection in CT Images Using Opposite Rays in Fan-Beam Projection Systems. IEEE Transactions on Medical Imaging 20(11): 1109-1122.
-
Green MV, Seidel J, Stein SD, Tedder TE, Kempner KM, et al. (1994) Head Movement in Normal Subjects during Simulated PET Brain Imaging with and without Head Restraint. J Nucl Med 35(9): 1538-1546.
-
Ritchie CJ (1995) Methods for Reducing Motion Artifacts in Computed Tomography Scans of the Chest. PhD Thesis 1995: 0506.
-
Boyd DP, Lipton MJ (1983) Cardiac Computed Tomography. Proceedings of the IEEE 71(3): 298-307.
-
Robb RA, Hoffman EA, Sinak LJ, Harris LD, Ritman EL (1983) High-Speed Three-Dimensional X-ray Computed Tomography: The Dynamic Spatial Reconstructor. Proceedings of the IEEE 71(3): 308-319.
-
Crawford CR, Godwin JD, Pelc NJ (1989) Reduction of Motion Artifacts in Computed Tomography. In Images of the Twenty-First Century. Proceedings of the Annual International Engineering in Medicine and Biology Society, pp: 485-486.
-
Crawford CR, Pelc NJ (1991) Method for Reducing Motion Induced Image Artifacts in Projection Imaging. United States patent US 4,994,965.
-
Menke M, Atkins MS, Buckley KR (1996) Compensation Methods for Head Motion Detected during PET Imaging. IEEE Transactions on Nuclear Science 43(1): 310-317.
-
Goldstein SR, Daube-Witherspoon ME, Green MV, Eidsath A (1997) A Head Motion Measurement System Suitable for Emission Computed Tomography. IEEE Transactions on Medical Imaging 16(1): 17-27.
-
Fulton RR, Eberl S, Meikle SR, Hutton BF, Braun M (1999) A Practical 3D Tomographic Method for Correcting Patient Head Motion in Clinical SPECT. IEEE Transactions on Nuclear Science 46(3): 667-672.
-
Beach RD, Gifford HC, Shazeeb S, Bruyant PP, Feng B, et al. (2005) Stereo-Infrared Tracking to Monitor and Characterize Rigid-Body Motion and Respiration during Cardiac SPECT Imaging: Progress towards Robust Clinical Utilization. IEEE Nuclear Science Symposium Conference Record, Fajardo, USA.
-
Bhowmik U, Iqbal MZ, Adhami R (2012) Mitigating Motion Artifacts in FDK based 3D Cone-Beam Brain Imaging System using Markers. Cent Eur J Eng 2(3): 369- 382.
-
Ko Y, Moon S, Baek J, Shim H (2021) Rigid and Non-rigid Motion Artifact Reduction in X-ray CT using Attention Module. Medical Image Analysis 67: 101883.
-
Duffy BA, Zhang W, Tang H, Zhao L, Law M, et al. (2022) Retrospective Correction of Motion Artifact Affected Structural MRI Images Using Deep Learning of Simulated Motion. Medical Imaging with Deep Learning, Amsterdam, Netherlands.
-
Zhao B, Liu Z, Ding S, Liu G, Cao C, et al. (2022) Motion Artifact Correction for MR Images based on Convolutional Neural Network. Optoelectronics Letters 18(1): 54-58.
-
Zhang L, Jiang B, Chen Q, Wang L, Zhao K, et al. (2023) Motion Artifact Removal in Coronary CT Angiography based on Generative Adversarial Networks. Eur Radiol 33(1): 43-53.
-
Su B, Wen Y, Liu Y, Liao S, Fu J, et al. (2022) A Deep Learning Method for Eliminating Head Motion Artifacts in Computed Tomography. Med Phys 49(1): 411-419.
-
Kyme AZ, Fulton RR (2021) Motion Estimation and Correction in SPECT, PET and CT. Phys Med Biol 66(18).
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey