Prevalence and Factors Associated with Anaemia among Pregnant Women Attending Antenatal Clinic in Mbaitoli L.G.A Imo State
Anemia during pregnancy continues to be a major health concern in Imo State and Nigeria. Globally, 41.8% - 60.0% of pregnant women experience anemia, and Nigeria has a prevalence rate of 55.1%. This cross-sectional study was conducted from September 2022 to May 2023 and involved 250 pregnant women who attended antenatal care at Nwaorieubi Comprehensive Health Center in Mbaitoli LGA, Imo State. The objective of this study was to gain insights into factors related to anemia, as well as prevention and control measures within the context of antenatal care. Data was collected through a structured questionnaire and by examining hemoglobin measurements from health records. Descriptive analysis was performed to determine means, frequencies, and proportions, while regression analysis (p<0.05) with odds ratios and a 95% confidence interval was used to explore associations. The prevalence of anemia during pregnancy was found to be 61%. The analysis revealed various factors contributing to anemia, including inadequate intake of vitamins, financial constraints, limited availability of antenatal care, lack of utilization of prenatal care services, gaps in awareness, cultural and social barriers, genetic conditions, and the occurrence of multiple pregnancies. Regression analysis highlighted significant correlations (p < 0.05) between inadequate intake of vitamins, underutilization of prenatal care, cultural and social barriers, genetic conditions, and multiple pregnancies. In terms of participant demographics, the descriptive analysis categorized participants into the following age groups: 15-22 (39 participants), 23-30 (90 participants), 31-39 (103 participants, 41%), and 40-49 (18 participants, 7%). It is worth noting that all participants in this study were married and identified as Christian. In order to raise awareness about the risk of developing anemia in late pregnancy, it is recommended that reproductive advice and education be provided to all women of reproductive age. Interventions such as mass media campaigns, outreach education, and life skills programs should be implemented to educate women on the importance of actively participating in antenatal care, adhering to prescribed medications, consuming a diverse range of nutritious meals, and incorporating iron-rich foods into their diets during pregnancy.
Introduction
The term Anemia finds its origin in the Ancient Greek language, specifically the term ἀναιμία anaimia, which conveys the concept of ‘deficiency of blood’. Consequently, this condition signifies a decrease in the population of red blood cells within the human body [1]. Anemia is a medical condition characterized by a decline in red blood cells (Erythrocytes) or the oxygen-carrying protein, hemoglobin (Hb). Consequently, the blood lacks the necessary capacities to transport oxygen, resulting in symptoms such as fatigue, debility, breathlessness, cephalalgia, and diminished exercise capacity. Moreover, this condition hampers the body’s aptitude for proper metabolism, making it frequently apparent in individuals experiencing severe anemia [2]. Additional indications of anemia encompass atypical cardiac arrhythmias, an absence of natural coloration in the skin, lowered blood pressure, and potentially even anguish in the thoracic region or impaired cardiac function. It is crucial to note that the manifestation and intensity of these symptoms are contingent upon the level of severity at which anemia is determined [3]. Anemia can arise from diminished red blood cell production, accelerated red blood cell degradation, significant hemorrhage leading to blood loss, inflammation of the stomach or intestine, surgical interventions, severe injuries, and blood donation [3]. Some common factors that contribute to the development of anemia include deficiencies in iron and vitamin B12, specific genetic conditions such as sickle cell anemia, infections experienced during pregnancy, acute malaria, thalassemia, as well as certain autoimmune diseases.
Anemia can manifest in individuals of any background, regardless of personal attributes, racial affiliation, ethnic heritage, or geographic location. It frequently presents itself in the pediatric and female populations [4]. For women of reproductive age, the onset of anemia during pregnancy poses a significant hazard to both the maternal and fetal health. This condition stands as a substantial and pervasive complication throughout the global landscape of pregnancy. Nigeria faces a significant challenge in terms of a noteworthy prevalence of anemia. Based on the estimations provided by the World Health Organization (WHO) in 2019, the prevalence of anemia in Nigeria stands at a notable 55.9%, with a range spanning from 51.6% to 58.7%. Moreover, data obtained from the Nigerian Demographic Health Survey conducted in 2023 reveals that approximately 61.1% of pregnant women within the country suffer from anemia. It is crucial to address this issue promptly as anemia greatly contributes to both mortality and morbidity among pregnant women, consequently heightening the risks associated with fetal development, neonatal health, and overall infant mortality rates [5]. Anemia is believed to have a significant impact on the health of a substantial number of women and children globally. Approximately, there are around 500 million women aged 15-49 and 269 million children aged 6-59 months who are affected by this condition. As of the year 2019, it was observed that 539 million non-pregnant women, accounting for 30% of that population, and 32 million pregnant women, accounting for 37% of that population, between the ages of 15 and 49 years were affected by anemia, according to the World Health Organization [6].
According to the World Health Organization’s (WHO) estimates in 2023, there were nearly 800 daily fatalities of women worldwide in the year 2020. A vast majority, approximately 95% (equivalent to 287,000 deaths), occurred in developing countries. Among these, the sub-Saharan Africa region was responsible for 70% (equivalent to 202,000 deaths). These fatalities, comprising 75% of the total, were primarily due to pregnancy-related complications. The latest report on maternal mortality trends, jointly conducted by WHO, UNICEF, UNFPA, World Bank Group, and UNDESA/ Population Division, reveals significant fluctuations from 2000 to 2020 [7]. In the year 2020, Nigeria recorded a significantly elevated maternal mortality ratio (MMR) of 1047 (with a confidence interval of 793 to 1586). On a global scale, it remains a prevailing issue that women continue to endure the occurrence of anemia during the period of pregnancy, resulting in a distressing 20% of maternal mortality cases [8]. According to the World Health Organization’s (WHO) classification, anemia is characterized as a medical condition wherein the hemoglobin concentration dips below 12.0 g/dl among non-pregnant individuals, and 11.0 g/dl for breastfeeding mothers. In the context of breastfeeding mothers, hemoglobin levels ranging from 10.0 to 10.9 g/dl are regarded as an indication of a moderately anemic state. In accordance with the extensive research conducted by Oyerinde et al. (2023), individuals exhibiting mild anemia are observed to possess hemoglobin concentrations within the range of 7.0 to 9.9 g/dl. Furthermore, those with severe anemia are identified as having hemoglobin levels below 7.0 g/dl. It is of significant importance to note that if the prevalence of anemia lies within the interval of 5.0% to 19.9%, it transforms into a matter of mild global health concern. Nonetheless, should the incidence escalate within the range of 20% to 39.9%, it escalates into a notable moderate global health issue. Based on the report provided by the World Health Organization (WHO) in 2021, the global prevalence of anemia among pregnant women is recorded at a substantial rate of 36.5%. This statistic serves as evidence that anemia poses a significant health challenge for expectant mothers worldwide. Due to the high incidence of anemia in Nigeria, it is crucial to devise enhanced strategies to counteract its adverse impact on maternal and child well- being. Consequently, this study was undertaken with the aim of examining the underlying frequency and contributing factors of anemia during pregnancy among expectant mothers, in order to propose guidelines for timely detection, treatment, and prevention of anemia.
Materials and Methods
Research Design
A comprehensive cross-sectional examination was conducted on a cohort comprising of 250 expectant mothers visiting the antenatal clinic at Nwaorieubi Comprehensive Health Center within the timeframe of September 2022 to May 2023. The main objective of this investigation was to identify the various factors that are closely linked to the prevalence of anaemia among pregnant women. Data was gathered through the diligent administration of questionnaires by the esteemed researchers, as well as the meticulous utilization of anthropometric measurements and laboratory tests extracted from the patient’s clinic cards/ register, with the aim of evaluating the hemoglobin levels.
Area of the Study
The area of the study’ is Nwaorieubi Comprehensive Health Center Mbaitoli L.G.A.
Population of the Study
The study population consisted of 250 pregnant mothers who sought antenatal care (ANC) at Nwaorieubi comprehensive health center in Mbailtoli and were registered between September 2022- May 2023.
Sampling and Sample Size
Purposive sampling technique refers to a method of selecting participants based on specific criteria or characteristics relevant to the research objectives. Unlike random sampling, where participants are chosen purely by chance, purposive sampling involves deliberately selecting individuals who possess certain attributes or experiences that are of interest to the study. This approach allows researchers to target a specific subgroup of the population that can provide valuable insights or information related to the research topic. We employed a purposive sampling technique to select a targeted group of 250 women, who attended antenatal care (ANC) at the Nwaorieubi Comprehensive Health Center in Mbaitoli, for inclusion in the study. Purposive sampling was chosen due to its effectiveness in selecting participants who possess specific characteristics or experiences relevant to the research objectives. This method allowed us to deliberately select participants who met predetermined criteria, such as pregnant women within a certain gestational age range and residing in the study area. By using purposive sampling, we aimed to ensure the inclusion of participants who could provide valuable insights into the factors influencing anemia in pregnancy, thus enhancing the relevance and depth of our findings. To prevent duplicate participant recruitment, the research assistants ensured that the individuals had not visited the ANC at the health center previously or participated in the study during the data collection period. Participants were enlisted in the waiting room of the antenatal care clinic.
Instrument of Data Collection
To obtain pertinent information concerning the participants, a personal interview was utilized. During this interview, a pre-tested structured questionnaire was employed. This questionnaire skillfully addressed various areas such as demographic and socio-economic attributes, comprehension of anaemia in pregnancy, comprehension of factors linked with anemia in pregnancy, understanding of the diagnosis of anemia, awareness of the repercussions of anemia in pregnancy, familiarity with preventive measures for anemia in pregnancy, and potential obstacles encountered when attending ante natal clinic.
Validity of the Instrument
The researcher submitted the questionnaire to the project supervisor for the purpose of assessing its content validity. Upon review, the project supervisor provided valuable input regarding necessary structural corrections and suggestions. These recommendations were carefully considered and subsequently implemented to enhance the quality of the questionnaire prior to its final approval. The modifications made were directly influenced by the insightful comments provided by the validators.
Reliability of the Instrument
In order to guarantee the dependability, lucidity, and straightforwardness of the questionnaire, a preliminary assessment was carried out at the Nkalu health ANC clinic. The Nkalu health centre possesses analogous attributes to the Nwaorieubi health center, as both establishments are situated in a semi-urban setting. A grand total of 25 expectant females (equivalent to 10% of the designated sample) were personally interviewed by the researcher, and the insights they provided were meticulously examined to effect suitable enhancements to the research instrument.
Method of Data Collection
The data collection process was conducted by the researcher and a trained assistant who were both well- versed in the effective utilization of tools and the acquisition of essential information. The assistant also received training on the significance of maintaining excellent communication skills while engaging with the participants, in order to guarantee comprehensive data collection. Before distributing the questionnaire, the researcher cordially welcomed the participants and respectfully inquired about their overall well-being, fostering a warm and inviting environment that facilitated open sharing of the requested information. All questionnaires were securely stored in locked cabinets throughout the duration of the study, with exclusive access granted solely to the researcher, thereby ensuring confidentiality and preventing any potential data loss.
Method of Data Analysis
In the process of analyzing numerical data, the quantitative data was carefully examined using Statistical Package for Social Sciences Version 23.0 (SPSS 23.0). Descriptive statistics were calculated for all pertinent variables. The data was then effectively presented through the use of tables and graphs, demonstrating the frequency distribution for both the independent and dependent variables. In order to determine the association between the independent variable and anemia, pertinent statistical tests such as Pearson’s chi-square test and odds ratio (or) were conducted. These tests were accompanied by corresponding 95% confidence intervals (CI). It is important to note that a significance level of 0.05 will be used to ascertain statistical significance.
Ethical Considerations
The study received official approval from Imo State University. Prior to conducting the study at Nwaorieubi Comprehensive Health Center, formal permission was acquired from the administrator of said health center. Each participant involved in the study was duly provided with thorough explanations regarding the specifics of the study. Furthermore, prior to their inclusion, the informed consent of each subject was diligently acquired.
Results
Socio-Demographic Characteristics of Participants
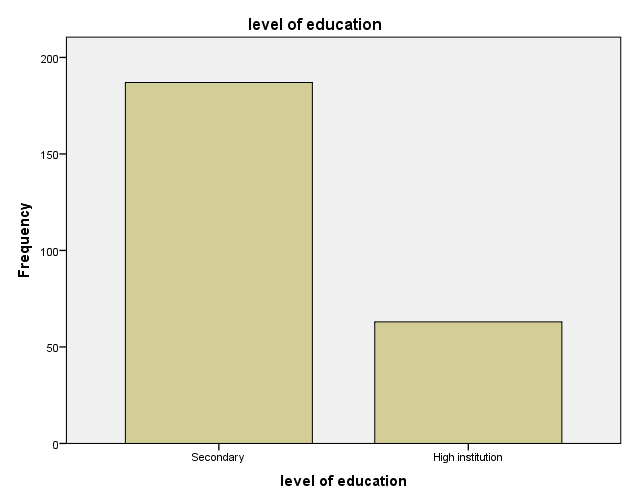
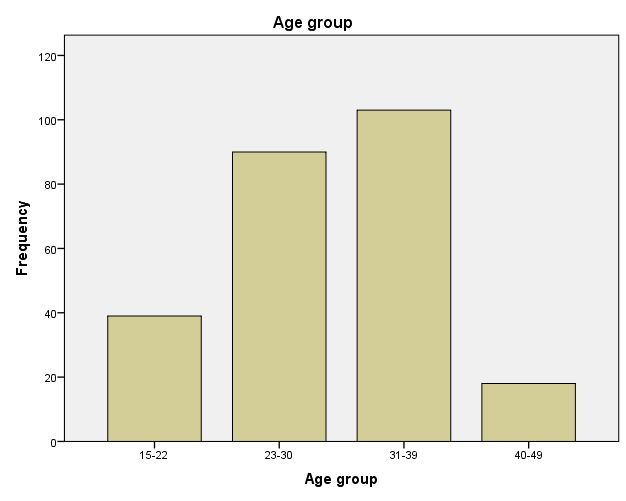
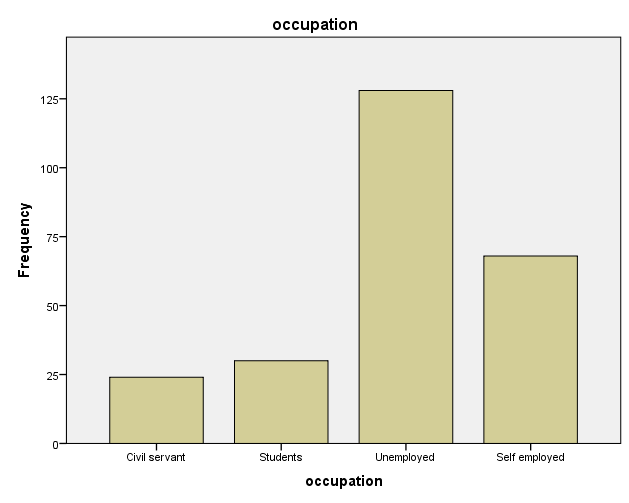
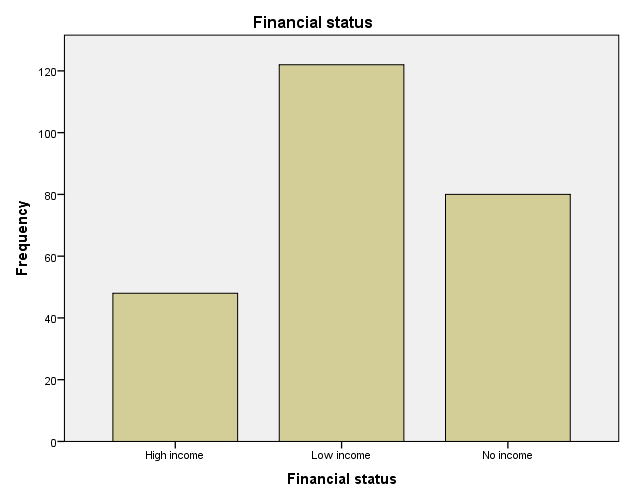
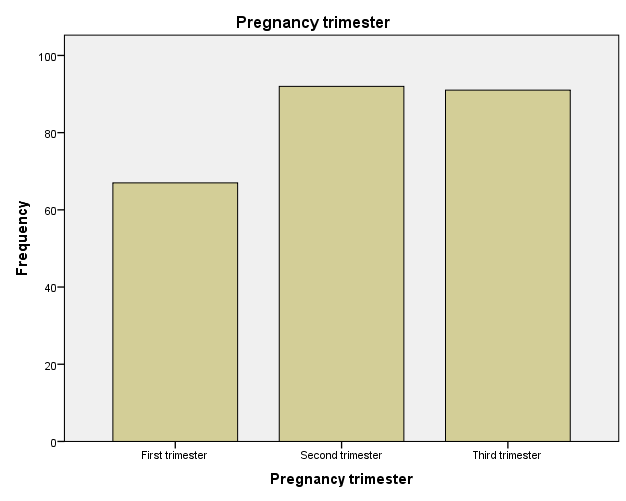
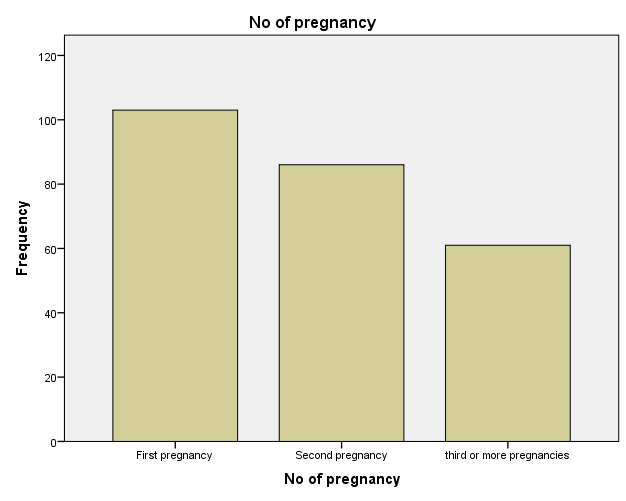
The socio-demographic characteristics of the respondents are shown below in Table 1. The mean age of women was 23.4 years with a SD of +_ 8 years. Out of the 250 participants 39(16%) and 103(41%) were in the age group of 15-22 and 31-39 respectively. 90(36%) and 18(7%) were 23-30 and 40-49 respectively. 31-39 as the highest age range. All the participants are Christians, Married and resides in Nigeria. Educational level of participants, 187(75%) and 63(25%) attended secondary and high institutions respectively, with no one at the primary level. Majority of the participants are unemployed, 128(51%). The rest are civil servant, student, self-employed with 24(10%), 30(12%), 68(27%) respectively. In the second trimester, 92(37%) participants were recorded as the highest majority of the participants; this is there first pregnancy, recording 103(41%). Their financial status is low since 122(49%) participants earn very little income, with 48(19%) women with High income and 80(32%) with no income at all.
| Variables | N | % |
|---|---|---|
| Age | ||
| 15-22 | 39 | 16% |
| 23-30 | 90 | 36% |
| 31-39 | 103 | 41% |
| 40-49 | 18 | 7% |
| Religion | ||
| Christian | 250 | 100% |
| Marital Status | ||
| Married | 250 | 100% |
| Level of Education | ||
| Primary | 0 | 0% |
| Secondary | 187 | 75% |
| High institution | 63 | 25% |
| Occupation | ||
| Civil servant | 24 | 10% |
| Student | 30 | 12% |
| Unemployed | 128 | 51% |
| Self employed | 68 | 27% |
| Financial Status | ||
| High Income | 48 | 19% |
| Low income | 122 | 49% |
| No income | 80 | 32% |
| Pregnancy Trimester | ||
| First trimester | 67 | 27% |
| Second trimester | 92 | 37% |
| Third trimester | 91 | 36% |
| No of Pregnancy | ||
| First Pregnancy | 103 | 41% |
| Second Pregnancy | 86 | 34% |
| Third Pregnancy and Above Pregnancy | 61 | 24% |
Table 1: Socio-demographic characteristics of pregnant women.
Knowledge of Pregnant Women on Anemia in Pregnancy
Table 2 below summarizes the level of understanding these women have concerning anemia in pregnancy. Majority, 227(91%), of women know about anemia. 119(48%) women knows that anemia is a condition of little blood level. These women were known to have very low level of understanding compared to 6(2%) that knows what anemia means, its consequences and factors that contributes to anemia, these participants have Very high level of understanding about anemia. 227(91%) out of 250 participants have heard of anemia occurring in pregnancy. Only 50(20%) have been diagnosed of anemia before. An average of 150 women experienced all the symptoms of anemia including: pale skin, fatigue, severe headaches, shortness of breath, dizziness, rapid heartbeat and so on.
| N | % | |
|---|---|---|
| The women knowledge about anemia in general | ||
| Yes | 227 | 91% |
| No | 23 | 9% |
| Their level of understanding about anemia | ||
| Very Low | 119 | 48% |
| Low | 72 | 29% |
| Moderate | 35 | 14% |
| High | 18 | 7% |
| Very High | 6 | 2% |
| Have you heard about anemia occurring in anemia | ||
| Yes | 227 | 91% |
| No | 23 | 9% |
| Have you been diagnosed with anemia before | ||
| Yes | 50 | 20% |
| No | 200 | 80% |
| Have you been experiencing fatigue in this pregnancy | ||
| Yes | 203 | 81% |
| No | 47 | 19% |
| Have you been experiencing pale skin | ||
| Yes | 190 | 76% |
| No | 60 | 24% |
| Have you been experiencing rapid heartbeat in this pregnancy | ||
| Yes | 130 | 52% |
| No | 120 | 48% |
| Have you been experiencing shortness of breath in this pregnancy | ||
| Yes | 140 | 56% |
| No | 110 | 44% |
| Have you been experiencing dizziness in this pregnancy | ||
| Yes | 178 | 71% |
| No | 72 | 29% |
| Have you been experiencing headache | ||
| Yes | 155 | 62% |
| No | 95 | 38% |
| Have you been experiencing swelling of the hands and feet | ||
| Yes | 129 | 52% |
| No | 121 | 48% |
| Do u have Malaria/Infection | ||
| Yes | 213 | 85% |
| No | 37 | 15% |
| Do u experience excessive blood loss | ||
| Yes | 10 | 4% |
| No | 240 | 96% |
Table 2: Knowledge of pregnant women on anemia in pregnancy.
Knowledge on Factors that Contribute to Anemia in Pregnancy
This section tests participants on their knowledge on factors that contributes to anemia in pregnancy. 109(44%), 73(29%), 78(31%), 115(46%), 166(66%), 142(57%), 64(26%), 149(60%), 159(64%), 86(34%) indicated that insufficient intake of vitamins and minerals, heavy menstrual bleeding, multiple pregnancy, certain genetic conditions, lack of financial resources, Limited availability of healthcare/facilities, low level education, underutilization of prenatal care, lack of awareness, cultural or social barrier as factors that contributes to anemia in pregnancy respectively. 138(55%) participants believed avoiding certain foods due to traditional practices may contribute to anemia in pregnancy. 91(36%) said herbal medicine without medical advice can contribute to anemia in pregnancy. While 21(8%) said smoking of cigarette and alcohol consumption.
| N | % | |
|---|---|---|
| Insufficient intake of vitamins and minerals | ||
| Yes | 109 | 44% |
| No | 141 | 56% |
| Lack of financial resources | ||
| Yes | 166 | 66% |
| No | 84 | 34% |
| Limited availability of healthcare/ facilities | ||
| Yes | 142 | 57% |
| No | 108 | 43% |
| Lack/ underutilization of prenatal care | ||
| Yes | 149 | 60% |
| No | 101 | 40% |
| Lack of awareness about anemia in pregnancy | ||
| Yes | 159 | 64% |
| No | 91 | 36% |
| Cultural or social barriers | ||
| Yes | 86 | 34% |
| No | 164 | 66% |
| Certain genetic conditions | ||
| Yes | 115 | 46% |
| No | 135 | 54% |
| Multiple pregnancies (having twins or more) | ||
| Yes | 78 | 31% |
| No | 172 | 69% |
Table 3: Knowledge on factors that contribute to anemia in pregnancy.
Knowledge of How Anemia Can Be Diagnosed
Table 4 Below summarizes participants knowledge on how anemia can be diagnosed. More than an average (54%) knows how anemia can be diagnosed, this was confirmed by a follow-up question. 55(41%), 70(52%) and 10(7%) participants chose blood test, urine test and physical examination respectively as a method of anemia diagnosis.
| 0.06 | N | % |
|---|---|---|
| Are you aware of how anemia in pregnancy can be diagnosed? | ||
| Yes | 135 | 54% |
| No | 115 | 46% |
| If yes. Which of the following is used to diagnose anemia during pregnancy? | ||
| Blood test | 55 | 41% |
| Urine test | 70 | 52% |
| Physical examination | 10 | 7% |
Table 4: Knowledge of how anemia can be diagnosed.
Knowledge of Consequences of Anaemia
This Table 5 show a summary of participants who knows about effects of anemia on pregnant women and on their fetus. 201(92%), 180(72%), 157(72%), 169(68%) participants knew it will lead to high risk of maternal mortality, infant mortality, preterm birth, low birth weight, and still birth respectively. Majority 183(84%) of them found it hard to believe that anemia in pregnancy can cause increased fatigue because fatigue is a symptom of pregnancy.
| N | % | |
|---|---|---|
| Do you think there are complications that may occur because of anemia during pregnancy for the pregnant woman and the developing fetus? | ||
| Yes | 219 | 88% |
| No | 31 | 12% |
| If yes, is fatigue and weakness one of the complications | ||
| Yes | 36 | 16% |
| No | 183 | 84% |
| Increased risk of infections | ||
| Yes | 131 | 60% |
| No | 88 | 40% |
| Increased risk of preterm birth | ||
| Yes | 157 | 72% |
| No | 62 | 28% |
| Increased risk of maternal mortality | ||
| Yes | 201 | 92% |
| No | 18 | 8% |
| What do you believe are the potential consequences of anemia during pregnancy for the developing fetus? Low birth weight | ||
| Yes | 169 | 68% |
| No | 81 | 32% |
| Premature birth | ||
| Yes | 132 | 53% |
| No | 118 | 47% |
| Developmental delays | ||
| Yes | 133 | 53% |
| No | 117 | 47% |
| Increased risk of stillbirth | ||
| Yes | 155 | 62% |
| No | 95 | 38% |
| Increased risk of infant mortality | ||
| Yes | 180 | 72% |
| No | 69 | 28% |
Table 5: Knowledge of Consequences of Anemia in Pregnancy.
Knowledge on the Prevention of Anemia in Pregnancy
132(53%) participants complained that they did not receive adequate prenatal care, while 118(47.2%) were satisfied with the ANC. The reason for most discomfort was that 138(55%) women felt that information was not properly shared about anemia in the ANC. 103(41%) women consumed iron rich food during ANC but a total of 147 pregnant women didn’t take it seriously. 97(39%) participants took the iron supplements as their healthcare provider prescribed seriously while the rest where not devoted. 140(56%) women wasn’t financially stable to get the nutritious food which was required.103 (41%) pregnant women thought that Iron supplement should be taken in the third trimester. Out of 250 participants, 152(60.8) have no knowledge of resources or programs available to support women managing anemia in pregnancy.
| N | % | |
|---|---|---|
| Did you receive adequate prenatal care during your pregnancy | ||
| Yes | 102 | 47% |
| No | 148 | 53% |
| Did you receive information about anemia during your antenatal care visits? | ||
| Yes | 107 | 45% |
| No | 143 | 55% |
| Did you consume iron-rich foods during pregnancy, such as red meat, leafy greens, or beans? | ||
| Yes, regularly | 64 | 41% |
| Occasionally | 54 | 20% |
| Rarely | 65 | 12% |
| Not at all | 67 | 27% |
| Did you take iron and folic acid supplements as recommended by your healthcare provider? | ||
| Yes, regularly | 57 | 39% |
| Occasionally | 49 | 16% |
| Rarely | 61 | 12% |
| Not at all | 83 | 33% |
| Can you name at least one recommended time for pregnant women to start taking iron supplements? | ||
| Early in pregnancy (first trimester) | 95 | 38% |
| Later in pregnancy (third trimester) | 103 | 41% |
| Anytime during pregnancy is fine | 52 | 21% |
| Did you have adequate financial resources to purchase nutritious food during pregnancy? | ||
| Yes | 98 | 44% |
| No | 152 | 56% |
| Are you familiar with any local programs or resources available to support pregnant women in managing anemia? | ||
| Prenatal care clinics | 47 | 19% |
| Community health centers | 37 | 15% |
| Government health programs | 14 | 6% |
| I don’t know of any | 152 | 61% |
Table 6: Knowledge on the prevention of anaemia in pregnancy.
Challenges Faced by Participants
Table 7 summarizes challenges faced by participants. Main challenges faced are Lack of transportation; 198(79%) women reported that they had difficulties in getting to the health center because of its distance. 177(71%) complained that they had to wait till they got attended to. 242(97%) had financial issues. Few participants, 30(12%) found it difficult to communicate in our lingua franca. 183(73%) participants had issues with cultural and social issues.
| N | % | |
|---|---|---|
| Is there any challenge that has hindered your attendance to ANC? | ||
| Yes | 232 | 93% |
| No | 18 | 7% |
| What were the main challenges you faced in accessing Antenatal Care services during your pregnancy? Lack of transportation options | ||
| Yes | 198 | 79% |
| No | 52 | 21% |
| Long waiting times at healthcare facilities | ||
| Yes | 177 | 71% |
| No | 73 | 29% |
| Limited availability of Antenatal Care centers in your area | ||
| Yes | 113 | 45% |
| No | 137 | 55% |
| Financial constraints and affordability issues | ||
| Yes | 242 | 97% |
| No | 8 | 3% |
| Cultural or social barriers | ||
| Yes | 183 | 73% |
| No | 67 | 27% |
| Language barriers | ||
| Yes | 30 | 12% |
| No | 220 | 88% |
| Fear of judgment or discrimination | ||
| Yes | 14 | 6% |
| No | 236 | 94% |
| Attitude of health workers | ||
| Yes | 191 | 76% |
| No | 59 | 24% |
| How would you rate the availability and proximity of Antenatal Care facilities in your area? | ||
| Very Accessible | 67 | 27% |
| Moderately Accessible | 45 | 18% |
| Not Accessible | 148 | 59% |
| How satisfied were you with the overall quality of the Antenatal Care services you received? | ||
| Very Satisfied | 24 | 10% |
| Satisfied | 53 | 21% |
| Neutral | 103 | 41% |
| Dissatisfied | 57 | 23% |
| Very Dissatisfied | 13 | 5% |
Table 7: Challenges faced by participants.
Research Questions 1: to determine the prevalence of anemia among pregnant women attending ANC in Nwaorieubi Health Center
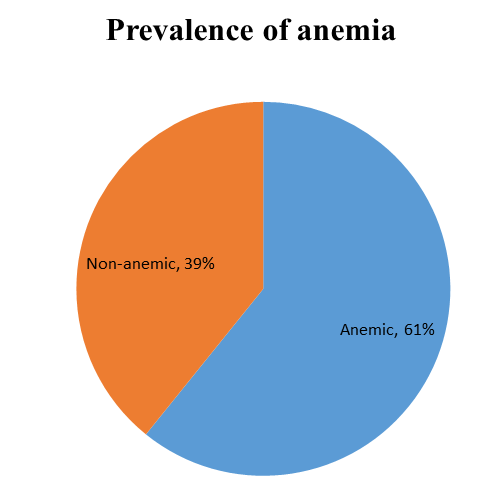
Prevalence of Anemia in Pregnancy: According to the established algorithm of anemia cut-off point of 11g/dl for the diagnosis of anaemia during pregnancy, the general prevalence rate of anaemia was found to be 61.0% as depicted in Figure 2. This indicates that more than half of the pregnant women in the study had an Hb concentration below the threshold for anaemia.
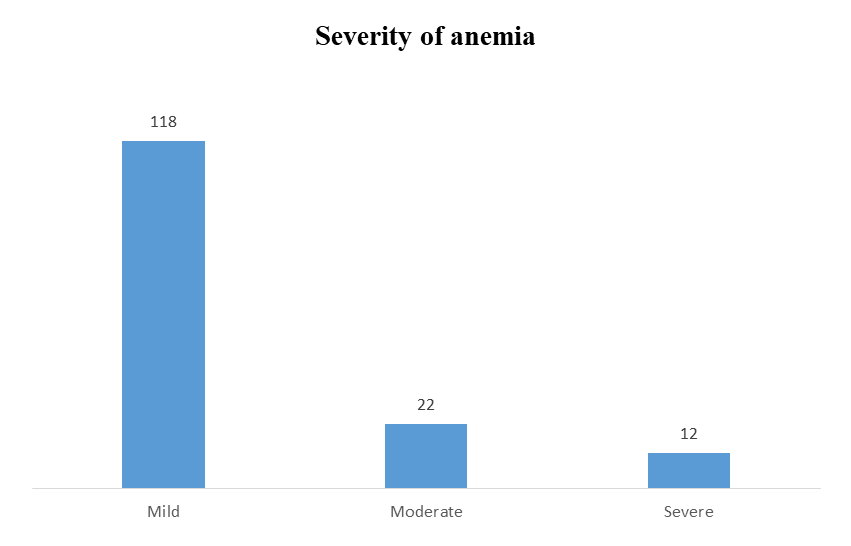
In terms of severity level, the prevalence of mild anaemia (Hb = 10-10.9 g/dl) was 118(47.2%), while the prevalence of moderate anaemia (Hb = 7-9.9 g/dl) was 22(8.8%). Severe anaemia (Hb < 7 g/dl) was found to have a prevalence of 12(4.8%). These percentages identify the epidemiology of anaemia severity among the pregnant women in the study.
Research Question 2: factors associated with anemia among pregnant women attending antenatal clinic.
A multivariate regression analysis was performed to determine the significance of factors associated with anemia and anemia in pregnancy. The null hypothesis states “There
- is no significant relationship between anemia and the factors”. We shall reject the null hypothesis if the p-value is less than alpha (0.05) otherwise, we will not. The result proved to be significant for factors such as insufficient intake
- Factors
- OR
- 95% CI
- X2
- Insufficient intake of vitamins and minerals
- -0.459
- -0.611
- -0.457
- 0
- Lack of financial resources
- -0.024
- -0.197
- 0.066
- 0.027
- Limited availability of ANC
- 0.056
- -0.002
- 0.111
- 0.058
- Lack/underutilization of prenatal care
- -0.429
- -0.501
- -0.352
- 0
- Lack of awareness
- 0.001
- -0.069
- 0.071
- 0.975
- Cultural or social barrier
- 0.278
- 0.231
- 0.383
- 0
- Certain genetic condition
- -0.373
- -0.685
- -0.508
- 0
- Multiple pregnancy
- 0.303
- 0.611
- 0.832
- 0
Table 8: Association between factors associated with anemia.
Research Question 3: knowledge about preventive and control measures of anemia in pregnancy
| N | % | |
|---|---|---|
| Did you receive adequate prenatal care during your pregnancy | ||
| Yes | 102 | 47% |
| No | 148 | 53% |
| Did you receive information about anemia during your antenatal care visits? | ||
| Yes | 107 | 45% |
| No | 143 | 55% |
| Did you consume iron-rich foods during pregnancy, such as red meat, leafy greens, or beans? | ||
| Yes, regularly | 64 | 41% |
| Occasionally | 54 | 20% |
| Rarely | 65 | 12% |
| Not at all | 67 | 27% |
| Did you take iron and folic acid supplements as recommended by your healthcare provider? | ||
| Yes, regularly | 57 | 39% |
| Occasionally | 49 | 16% |
| Rarely | 61 | 12% |
| Not at all | 83 | 33% |
| Can you name at least one recommended time for pregnant women to start taking iron supplements? | ||
| Early in pregnancy (first trimester) | 95 | 38% |
| Later in pregnancy (third trimester) | 103 | 41% |
| Anytime during pregnancy is fine | 52 | 21% |
| Did you have adequate financial resources to purchase nutritious food during pregnancy? | ||
| Yes | 98 | 44% |
Table 9: Knowledge about preventive and control measures of anemia in pregnancy.
| 152 | 56% | |
|---|---|---|
| Are you familiar with any local programs or resources available to support pregnant women in managing anemia? | ||
| Prenatal care clinics | 47 | 19% |
| Community health centers | 37 | 15% |
| Government health programs | 14 | 6% |
| I don’t know of any | 152 | 61% |
Table 10: Knowledge about preventive and control measures of anemia in pregnancy.
Hypothesis I: There is no significant difference in the prevalence of anemia among pregnant women in Nwaorieubi Comprehensive Health Center, Mbaitoli LGA, Imo state.
The result of the chi-square test of independence as shown below revealed that since the p-value (0.002 and <.001) is less than the alpha (0.05), we reject the null hypothesis and conclude that there is significant relationship between anemia and its prevalence. It is worth nothing that there was no significant relationship between anemia and age group. Although, in several studies, there’s always been a significant relationship.
| Variable | Frequency (%) Anemia | X2 | p | |
|---|---|---|---|---|
| No | Yes | |||
| Age | ||||
| 15-22 | 16(41) | 23(59) | 0.837 | 0.841 |
| 23-30 | 33(36.7) | 57(63.3) | ||
| 31-39 | 43(41.7) | 60(58.3) | ||
| 40-49 | 6(33.3) | 12(66.7) | ||
| Financial status | ||||
| No income | 19(23.8) | 61(76.2) | 11.991 | 0.002 |
| Low income | 58(47.5) | 64(52.5) | ||
| High income | 21(43.8) | 27(56.2) | ||
| Gravida(trimester) | ||||
| First trimester | 19(28.4) | 48 | 15.046 | <.001 |
| Second trimester | 29(31.5) | 63(68.5) | ||
| Third trimester | 50(55) | 41(45) |
Hypothesis II: There are no association between factors associated with anemia and anemia in pregnancy among women in Nwaorieubi Comprehensive Health Center, Mbaitoli LGA, Imo state.
• Model Summary
| Model | R | R Square | Adjusted R Square | Std. Error of the Estimate |
|---|---|---|---|---|
| 0.94 | 0.882 | 0.879 | 0.17045 |
The model summary shows the R (correlation coefficient) value and the R Square values with other statistics. The R value shows that there is a very strong positive relationship between the dependent variable (Anaemia) and the independent variables (Insufficient intake of vitamins and minerals, Lack of financial resources, Limited availability of ANC, Lack/underutilization of prenatal care, Lack of awareness, Cultural or social barrier, Certain genetic condition and Multiple pregnancy). The R Square values shows that about 88.2% of the variation in Anaemia is accounted for by the factors. This implies that the model is adequate for predicting Anaemia. We shall reject the null hypothesis is the p-value is less than the alpha (0.05), otherwise, we will not.
• ANOVA
| Model | Sum of Squares | df | Mean Square | F | P-Value |
|---|---|---|---|---|---|
| Regression | 52.6 | 8 | 6.573 | 226.243 | 0 |
| Residual | 7 | 241 | 0.029 | ||
| Total | 59.6 | 249 |
Since the p-value (0.000) is less than the alpha (0.05), we reject the null hypothesis and conclude that there is a significant relationship between Anaemia and the factors.
This implies that the factors significantly contributed to Anaemia. However, the Table will show the factors that are making significant contributions to Anaemi Coefficient.
| Model | Unstandardized Coefficients | Standardized Coefficients | T | P-Value | 95.0% Confidence Interval for B | |||
|---|---|---|---|---|---|---|---|---|
| B | Std. Error | Beta | Lower Bound | Upper Bound | ||||
| (Constant) | 0.748 | 0.066 | 11.252 | 0 | 0.617 | 0.879 | ||
| Insufficient intake of vitamins and minerals | -0.534 | 0.039 | -0.459 | -13.671 | 0 | -0.611 | -0.457 | |
| Lack of financial resources | -0.066 | 0.067 | -0.024 | -0.982 | 0.027 | -0.197 | 0.066 | |
| Limited availability of ANC | 0.055 | 0.029 | 0.056 | 1.905 | 0.058 | -0.002 | 0.111 | |
| Lack/underutilization of prenatal care | -0.426 | 0.038 | -0.429 | -11.278 | 0 | -0.501 | -0.352 | |
| Lack of awareness | 0.001 | 0.035 | 0.001 | 0.031 | 0.975 | -0.069 | 0.071 | |
| Cultural or social barrier | 0.307 | 0.039 | 0.278 | 7.955 | 0 | 0.231 | 0.383 | |
| Certain genetic condition | -0.596 | 0.045 | -0.373 | -13.308 | 0 | -0.685 | -0.508 | |
| Multiple pregnancy | 0.722 | 0.056 | 0.303 | 12.863 | 0 | 0.611 | 0.832 |
Hypothesis III: There is no significant between the knowledge and prevention and control of anemia amongst pregnant women attending ANC in Nwaorieubi Comprehensive Health Center, Mbaitoli LGA, Imo state.
The chi-square results shown below, indicated that since the p values (0.002, <.001) are less than alpha(0.005) we reject the null hypothesis and conclude that there is significant between consuming iron rich food; Folic acid and iron supplement; and having knowledge on programs that helps pregnant women with anemia. It should be noted that in this study, variables such as Received adequate ANC, Received information about anemia, had adequate financial resources and recommended time to start taking Iron supplement, was not statistically significant.
| Variable | Frequency(%) Anemia | X2 | P | |
|---|---|---|---|---|
| No | Yes | |||
| Received Adequate ANC | ||||
| Yes | 38(37.3) | 64(62.8) | 0.274 | 0.601 |
| No | 60(40.5) | 88(59.5%) | ||
| Received information about anemia | ||||
| Yes | 46(43) | 61(57) | 1.128 | 0.288 |
| No | 52(36.4) | 91(63.6) | ||
| Had adequate financial resources | ||||
| Yes | 32(32.7) | 66(67.3) | 2.899 | 0.089 |
| No | 66(43.4) | 86(56.6) | ||
| consume iron rich food | ||||
| Not at all | 27(40.3) | 40(59.7) | 15.003 | 0.002 |
| Rarely | 19(29.2) | 46(70.8) | ||
| Occasionally | 15(27.8) | 39(72.2) | ||
| Yes, regularly | 37(57.8) | 27(42.2) | ||
| Took iron and folic acid supplement | ||||
| Not at all | 32(56.1) | 25(43.9) | 40.418 | <.001 |
| Rarely | 14(28.5) | 35(71.4) | ||
| Occasionally | 6(9.8) | 55(90.2) | ||
| Yes, regularly | 46(55.4) | 37(44.6) | ||
| Recommended time to start taking Iron supplements | ||||
| Early in pregnancy | 38(40) | 57(60) | 1.861 | 0.394 |
| later in pregnancy | 36(35) | 67(65) | ||
| Anytime during pregnancy | 24(46.2) | 28(53.8%) | ||
| Which local program that supports anemic pregnant women do u know | ||||
| Prenatal care clinics | 22(46.8) | 25(53.2) | 16.591 | <.001 |
| Community health centers | 23(62.2) | 14(37.8) | ||
| Government health program | 1(7.1) | 13(92.9) | ||
| I don’t know any | 52(34.2) | 100(65.8) |
Discussion
The socio-demographic characteristics provided in these findings offer valuable insights into the contextual framework of the pregnant women under investigation. These factors play a pivotal role in shaping the overarching landscape within which maternal health and well-being unfold [9]. The age distribution demonstrates diversity, with the majority (41%) falling within the 31-39 age bracket. The study participants share a common Christian religious affiliation (100%), creating a cohesive spiritual backdrop. Marital status reveals that all participants are married (100%), implying a consistent marital environment during pregnancy. Educational diversity emerges, with 75% having completed secondary education and 25% holding higher qualifications. Remarkably, primary education is absent, suggesting potential differences in health literacy [10]. Occupational variety encompasses civil servants (10%), students (12%), unemployed individuals (51%), and self- employed individuals (27%), highlighting a spectrum of socio- economic contexts. Financial status disparities are evident, with 49% classified as low-income and 32% reporting no income. These discrepancies can influence healthcare access and overall well-being. Trimester distribution is balanced, affording the exploration of anemia-related factors across pregnancy stages [11]. Pregnancy frequency reveals 41% experiencing their first pregnancy, 34% in their second, and 24% with three or more pregnancies. This distribution enriches our understanding of participants’ pregnancy experiences [12]. These socio-demographic attributes encompass age, religious affiliation, marital status, education, occupation, financial status, pregnancy trimester distribution, and pregnancy count. These facets provide the vital framework to comprehend subsequent analyses regarding knowledge, health indicators, and factors contributing to anemia during pregnancy.
Anemia during pregnancy is a well-recognized concern due to its potential impacts on maternal and fetal health. To better understand women’s knowledge and experiences regarding anemia in pregnancy, a comprehensive survey was conducted, analyzing participants’ familiarity with anemia, its occurrence during pregnancy, and the prevalence of associated symptoms [10]. The survey results indicated that the majority of participants (91%) were aware of anemia in general. This high level of general awareness suggests that anemia is a concept familiar to the sampled population. Similarly, 91% of respondents reported having heard about anemia occurring during pregnancy, highlighting that participants had a reasonable understanding of the specific context of anemia within the prenatal period [13]. Regarding participants’ understanding of anemia’s severity levels, the results revealed varying levels of comprehension. A significant proportion of respondents reported having a “very low” (48%) or “low” (29%) understanding of anemia. This distribution suggests that there is a substantial portion of the population that may not possess a comprehensive grasp of anemia’s implications, especially in the context of pregnancy. Conversely, a smaller but notable number of participants reported having a “moderate” (14%), “high” (7%), or even a “very high” (2%) level of understanding [14]. These findings underscore the heterogeneity in participants’ awareness levels and suggest the potential for targeted educational initiatives to address these disparities [15]. The survey further investigated the prevalence of symptoms associated with anemia during pregnancy. Fatigue, a common symptom attributed to reduced oxygen-carrying capacity of the blood, was reported by 81% of participants. Additionally, symptoms such as pale skin (76%), dizziness (71%), rapid heartbeat (52%), shortness of breath (56%), headache (62%), and swelling of the hands and feet (52%) were also reported by varying proportions of respondents. These reported symptoms align with established manifestations of anemia and highlight the potential impact on participants’ quality of life during pregnancy [16]. Indeed, the survey provides valuable insights into women’s knowledge and experiences regarding anemia during pregnancy. While the majority of participants demonstrated awareness of anemia and its occurrence during pregnancy, the varying levels of understanding and the prevalence of associated symptoms suggest opportunities for enhanced education and awareness campaigns. Addressing these gaps in knowledge could ultimately lead to improved maternal care and healthier pregnancy outcomes.
The findings of the study provide valuable insights into the multifaceted nature of anemia during pregnancy. Anemia, characterized by insufficient red blood cell count and hemoglobin levels, can have serious implications for both maternal health and fetal development. The study investigated several key factors contributing to anemia in pregnancy and highlighted their respective percentages among the participants. One notable finding is the prevalence of insufficient intake of vitamins and minerals among pregnant women. This factor was identified in 44% of the participants. Inadequate nutrition, particularly the lack of essential nutrients like iron, folic acid, and vitamin B12, can hamper the body’s ability to produce sufficient red blood cells, leading to anemia [16]. Financial constraints emerged as a significant barrier, with 66% of participants reporting limited financial resources. This finding underscores the intricate link between socioeconomic status and anemia risk. Financial limitations can restrict access to a varied and nutrient-rich diet, making it challenging for pregnant women to meet their increased nutritional needs during this critical period [17]. Limited access to healthcare facilities was reported by 57% of participants. This points to a concerning issue of healthcare disparities, where certain pregnant women face challenges in accessing timely medical care, including regular check-ups and early detection of anemia. Inadequate healthcare infrastructure can hinder proper anemia management and exacerbate its effects on maternal and fetal health. The study also shed light on the significance of prenatal care utilization. Approximately 60% of pregnant women did not fully utilize prenatal care services. These finding highlights missed opportunities for early detection, monitoring, and intervention in managing anemia. Prenatal care visits are crucial for tracking maternal health indicators, including hemoglobin levels, and addressing anemia- related concerns promptly. Lack of awareness emerged as a substantial contributor, with 64% of participants lacking awareness about anemia during pregnancy. This suggests a need for comprehensive health education programs that not only inform pregnant women about anemia but also emphasize its importance, its risk factors, and the available interventions.
Cultural and social barriers were identified in 34% of participants. Sociocultural factors play a pivotal role in shaping dietary habits and healthcare-seeking behaviors. Certain cultural practices and beliefs might influence dietary choices, impacting the intake of necessary nutrients for preventing anemia [18]. Genetic conditions were reported in 46% of participants. Certain genetic factors can affect the body’s ability to produce and maintain healthy red blood cells, predisposing pregnant women to anemia. This finding underscores the complex interplay between genetic predisposition and environmental factors in anemia development. Lastly, the study highlighted the impact of multiple pregnancies on anemia risk. Approximately 31% of participants carrying twins or more were at a heightened risk of anemia. This is attributed to the increased demands of multiple fetuses, leading to the depletion of maternal iron stores.
All this is in line with previous study by Oyedeji A, et al. [19] which pointed out that biological factors such as Iron stores plays an important role in curbing anaemia in pregnancy. In conclusion, the study’s findings collectively emphasize the need for a comprehensive approach to address anemia during pregnancy. Strategies should include improving nutritional education, enhancing healthcare accessibility, raising awareness about anemia, and tailoring interventions to specific cultural contexts. By addressing these factors, healthcare providers and policymakers can work towards reducing the prevalence and consequences of anemia in pregnant women, ultimately promoting better maternal and fetal outcomes. The study investigated the understanding of anemia diagnosis during pregnancy among participants. A total of 250 participants were involved in the study. The participants were asked whether they were aware of the methods for diagnosing anemia during pregnancy. Out of the total participants, 135 (54%) indicated that they were aware of the diagnostic methods, while 115 (46%) stated that they were not aware [20]. For those participants who responded positively to being aware of anemia diagnosis methods, they were further queried about the specific methods they believed were used for diagnosing anemia during pregnancy. The responses were categorized into three options: blood test, urine test, and physical examination. Among the participants who claimed awareness, 55 (41%) mentioned blood tests as a method for diagnosing anemia during pregnancy. This suggests that a substantial portion of respondents recognized blood tests as a diagnostic approach. Furthermore, 70 (52%) participants indicated urine tests as a means of diagnosing anemia during pregnancy. This response highlights that a majority of participants associated urine tests with anemia diagnosis, possibly indicating a prevalent misconception. A smaller subset of participants, specifically 10 (7%), mentioned physical examination as a method for diagnosing anemia during pregnancy. This finding underscores that only a minority of respondents linked physical examination with anemia diagnosis, indicating a potential lack of awareness regarding this aspect.
The study uncovered that 54% of the participants were aware of how anemia can be diagnosed during pregnancy. Among those aware, a considerable proportion attributed anemia diagnosis to urine tests (52%) and blood tests (41%), while a minority associated it with physical examination (7%). These findings suggest varying levels of awareness and misconceptions among participants concerning anemia diagnosis during pregnancy. The present study investigated the level of awareness regarding potential complications associated with anemia during pregnancy for both the pregnant woman and the developing fetus. The study population was comprised of respondents who were asked to provide their perceptions on the matter. Of the participants, 88% (219) acknowledged the existence of possible complications stemming from anemia during pregnancy; while 12% (31) held the view that anemia would not lead to complications. Among those who recognized the potential for complications due to anemia, 16% (36) identified fatigue and weakness as one of the associated complications, while 84% (183) did not associate fatigue and weakness with anemia during pregnancy. Regarding the increased risk of infections as a consequence of anemia during pregnancy, 60% (131) of participants believed in this association, whereas 40% (88) did not perceive an elevated risk of infections. Concerning the likelihood of increased risk of preterm birth due to anemia, 72% (157) of participants concurred with this possibility, in contrast to 28% (62) who did not acknowledge anemia as a risk factor for preterm birth. It supported this claim that anemia results to preterm birth and intrauterine growth restriction. Moreover, 92% (201) of respondents believed in the heightened risk of maternal mortality associated with anemia during pregnancy, while only 8% (18) did not view maternal mortality as a potential consequence. When considering the potential consequences of anemia during pregnancy for the developing fetus, 68% (169) of participants believed it could lead to low birth weight, whereas 32% (81) did not perceive this association. In terms of premature birth as a potential outcome of anemia during pregnancy, 53% (132) of participants endorsed this view, while 47% (118) did not connect anemia to premature birth. Kalaivani., added that anemia during pregnancy affects fetal development and prognosis, thereby causing growth retardation, prematurity and low birth weight.
Similarly, 53% (133) of respondents recognized developmental delays as a potential consequence of anemia during pregnancy, while 47% (117) did not associate developmental delays with anemia. Olujimi et al., 2014 supported this claim by saying that the chances of fetal growth restriction and low birth weight, which is a sign of developmental delays, are tripled when the pregnant woman is anemic. Furthermore, 62% (155) of participants believed that anemia could increase the risk of stillbirth, in contrast to 38% (95) who did not consider stillbirth to be linked to anemia. Finally, 72% (180) of participants perceived an elevated risk of infant mortality due to anemia during pregnancy, while 28% (69) did not attribute anemia to an increased risk of infant mortality. The research aimed to assess the level of knowledge concerning the prevention of anemia during pregnancy, encompassing various aspects including prenatal care, information dissemination, dietary practices, supplement intake, awareness of supplementation timing, financial resources, and familiarity with available support programs. Among the participants, 47% (102) reported receiving adequate prenatal care during their pregnancy, while the remaining 53% (148) indicated otherwise. In terms of information dissemination, 45% (107) of respondents received information about anemia during their antenatal care visits, whereas 55% (143) did not receive such information. Regarding dietary practices, 41% (64) of participants consumed iron-rich foods regularly, while 20% (54) did so occasionally, 12% (65) did so rarely, and 27% (67) did not consume such foods at all during pregnancy. In relation to supplement intake, 39% (57) took iron and folic acid supplements regularly, 16% (49) did so occasionally, 12% (61) did so rarely, and 33% (83) did not take these supplements at all. When asked about the recommended time to start taking iron supplements, 38% (95) identified the early pregnancy period (first trimester) as the appropriate time, 41% (103) indicated the later pregnancy stage (third trimester), and 21% (52) believed that iron supplementation could begin at any time during pregnancy. Financial resources for purchasing nutritious food were found to be adequate for 44% (98) of respondents, while 56% (152) reported insufficient resources for this purpose.
In terms of awareness of local programs or resources supporting pregnant women in managing anemia, 19% (47) were familiar with prenatal care clinics, 15% (37) with community health centers, 6% (14) with government health programs, and 61% (152) indicated a lack of awareness regarding any such programs. These findings highlight disparities in knowledge and practices related to anemia prevention during pregnancy. While some respondents demonstrated adherence to recommended practices such as regular intake of iron-rich foods and supplements, others exhibited gaps in knowledge and access to resources. The prevalence of inadequate awareness underscores the need for targeted educational initiatives, improved access to prenatal care, and enhanced dissemination of information to promote optimal practices for preventing anemia during pregnancy [21]. The research delved into the challenges encountered by participants in accessing antenatal care (ANC) services during pregnancy. This exploration encompassed various dimensions including hindrances to ANC attendance, main challenges faced, factors influencing accessibility, satisfaction with service quality, and evaluations of ANC facility availability. The majority (93%) of participants reported facing challenges that hindered their attendance to ANC, indicating prevalent obstacles in accessing these crucial healthcare services. Concerning the primary challenges encountered in accessing ANC services, lack of transportation options emerged as a significant obstacle, with 79% of participants identifying this factor as a hindrance. Long waiting times at healthcare facilities were reported by 71% of respondents, signifying a potential area for improvement in service efficiency. Similarly, 45% of participants faced difficulties due to the limited availability of ANC centers in their locality. Financial constraints and affordability issues were a substantial barrier, affecting 97% of participants. This underscores the need to address economic barriers to ensure equitable access to ANC services. Cultural or social barriers were noted by 73% of respondents, implying that cultural sensitivities and social norms could impact ANC utilization. Additionally, language barriers were reported by 12% of participants, which highlights the importance of providing services in languages understandable to diverse populations. Fear of judgment or discrimination was indicated by 6% of participants, suggesting that negative perceptions associated with seeking ANC may deter some individuals. Moreover, the attitude of health workers influenced ANC access for 76% of respondents. This indicates that provider behavior and patient-provider interactions are integral factors affecting service utilization. Participants’ evaluations of ANC facility availability revealed that 59% considered such facilities as not accessible in their areas. Only 27% found them to be very accessible, while 18% regarded them as moderately accessible. Satisfaction levels with the overall quality of received ANC services varied: 10% were very satisfied, 21% were satisfied, 41% expressed a neutral sentiment, 23% were dissatisfied, and 5% were very dissatisfied. Hence, the findings illuminate the multifaceted challenges participants encounter in accessing ANC services. These challenges span transportation, waiting times, service availability, financial constraints, cultural and social factors, language barriers, fear of judgment, and health worker attitudes. Addressing these challenges is paramount to ensuring equitable access to high-quality ANC services and promoting positive maternal and fetal health outcomes.
Globally, the prevalence of anaemia during pregnancy has been reported to range from 41.8% to 60.0%, with higher rates observed in developing countries and Africa specifically. In Nigeria, the national prevalence of anaemia in pregnancy is 55.1 % [6]. However, in this study conducted at Comprehensive Health Care Centers in Nwaorieubi Mbaitoli LGA in lmo State, the overall prevalence of anaemia among pregnant women was found to be 61%. According to the World Health Organization’s classification, this indicates a severe public health problem in this population. The prevalence of anaemia in this study is higher than the national prevalence globally which lies within 36.5% (WHO, 2019) also higher than the rates reported in other African countries such as United Republic of Tanzania and Zimbabwe. In sub-saharan Africa, the incidence of anemia during pregnancy can be as high as 57.1% [20]. The high prevalence of anaemia in this study can be attributed to the low socioeconomic status of the women, as most participants had a low monthly income Low socioeconomic status is known to affect nutritional status and health-seeking behavior, as women in this group may face financial constraints and have limited access to quality healthcare services. Overall, these findings highlight the need for targeted interventions to address anaemia among pregnant women in this population, with a focus on improving socioeconomic conditions, promoting early and regular antenatal care attendance, and implementing effective nutritional interventions. The association between iron and folic acid supplementation and anaemia showed that pregnant women who did not take these supplements were at a significantly higher risk of developing anaemia compared to those who took them. This finding is consistent with previous studies conducted in Ethiopia, Uganda, Vietnam, India, and other countries, which have also indicated that inadequate intake and absorption of essential nutrients, especially iron, folic acid, and vitamin B12, contributes significantly to anemia during pregnancy [21]. The reason behind this association is that iron and folic acid supplementation help increase hemoglobin levels and prevent anaemia during pregnancy. Even if a woman had sufficient iron levels before pregnancy, the increased demands of the growing fetus, uterus, and placenta, as well as the increased red blood cell mass, require additional iron and folic acid during pregnancy. In developing countries, where nutritional deficiencies are common, dietary intake alone may not meet these increased requirements, making oral iron supplementation crucial. To address this, the World Health Organization (WHO) recommends daily oral iron and folic acid supplementation of 60 mg and 400 μg, respectively, throughout pregnancy as part of antenatal care programs. In this study, it was observed that most women didn’t take iron rich food and supplements as instructed by the healthcare provider seriously. This may be because of lack of information on the consequences of anemia.
The influence of lack of information while attending the ANC with occurrences of anemia with prevalence of 73.4% anemic women did not receive adequate information concerning the consequence of anemia compared to 43.9% of anemic women. This habit of ignorance may contribute to the high prevalence of anemia observed in this study.
Furthermore, the study revealed poor awareness among pregnant women regarding the consequences of anaemia during pregnancy. Only a small percentage of participants were aware of these consequences. Improving awareness and education about the importance of iron and folic acid supplementation during pregnancy could help address these barriers and reduce the prevalence of anaemia [22]. The association between lack of financial resources and anaemia revealed that unemployed participants had a higher proportion of anaemia which is consistent with findings from studies conducted in Pakistan and Brazil. This association can be attributed to several factors related to the employment status of the women. In many low-income settings, women often need to work outside the home due to low family income, which can result in increased physical and mental stress. Commonly in Igboland unemployed women(without government works) goes to farm, to clear bushes, plant crops and still come home to cook for their family. Pregnant women who are unemployed may have limited time for rest and may face challenges in attending antenatal care (ANC) appointments regularly. The demanding nature of their jobs and lack of flexibility may make it difficult for them to prioritize their own health and attend ANC visits as frequently as needed. Furthermore, employed women in these settings are often considered underemployed, meaning they have unstable or low-paying jobs that provide limited financial resources. This can impact their ability to afford nutritious food and access other resources necessary for maintaining good health during pregnancy.
Conclusion
It is worth noting that anemia is a health problem in Imo state and Nigeria in general. According to this research, anemia prevalence in Imo state is 61.0%. In Nigeria as of 2019, the prevalence rate is 51.0%. In this study it was observed that economic factor; Low or No income, lack of awareness about anemia in pregnancy, were the contributing factors to high prevalence of anemia in Imo state. The economic status impeded participants from purchasing iron and vitamin rich supplements prescribed by the healthcare provider. Also, geographical proximity discouraged women who had little economic support from actively engaging with the ANC process. Hence, preconception care; good antenatal care should be made available with well trained staff that will be more informative on health problems such as anemia, iron deficiency and other hematological disease. In addition, combination of nutritional supplementation and food fortification program, as well as efforts with alleviation of family poverty may translate into optimal improvement in the Hb levels of the mothers. By addressing these factors, and implementing comprehensive intervention, the burden of anemia during pregnancy can be reduced, ultimately improving the health outcomes of pregnant women and their infants.
References
-
Adama SO, Akoja FT, Fawole O, Nwonu EI, Musa J, et al. (2020) Anaemia among Pregnant Women in Kogi State, Nigeria: The Role of Dietary Diversity and Multivitamin Supplementation. Annals of African Medicine 19(2): 112-117.
-
WHO (2020) Anaemia. World Health Organization.
-
Pena-Rosas JP, De-Regil LM, Dowswell T, Viteri FE (2015) Daily Oral Iron Supplementation during Pregnancy. Cochrane Database Syst Rev 2015(7): CD004736.
-
Pena-Rosas JP, De-Regil LM, Malave HG, Flores-Urrutia MC (2017) Intermittent Oral Iron Supplementation during Pregnancy. Cochrane Database Syst Rev 2017(11).
-
Steer P, Alam MA, Wadsworth J, Welch A (2018) Relation between Maternal Haemoglobin Concentration and Birth Weight in Different Ethnic Groups. BMJ 300(6727): 1697-1700.
-
World Health Organization (WHO) (2020) The Global Prevalence of Anaemia in 2011. World Health Organization, Geneva.
-
Adegbola O, Okunade K, Olowookere AE, Dairo MD, Aimakhu CO (2018) Prevalence and Determinants of Anemia in the First and Third Trimesters of Pregnancy in a Semi-Urban Community in Nigeria. Annals of African Medicine 17(1): 25-30.
-
Adejumo OI, Oso AA, Adejumo WL (2020) Prevalence and Determinants of Anemia among Pregnant Women Attending a Secondary Healthcare Facility in Southwestern Nigeria. Journal of Health, Population and Nutrition 39(1): 1-8.
-
Obi SN, Onah HE, Ezugwu FO (2020) Anemia in Pregnancy: A Public Health Problem in Enugu, Nigeria. Journal of Obstetrics and Gynaecology Research 46(3): 358-365.
-
Odjimogho SE, Adekanle DA, Ademakinwa OJ (2017) Prevalence and Determinants of Anaemia among Pregnant Women in a Rural Community of Ogun State, Southwest Nigeria. The Pan African Medical Journal 28(1): 1-7.
-
Bodnar LM, Scanlon KS, Freedman DS, Siega-Riz AM (2019) Sociodemographic and Cultural Factors Impacting the Amount, Frequency, and Delivery Method of Pregnant Women’s Consumption of Prenatal Vitamins in the United States. The Journal of Maternal-Fetal & Neonatal Medicine 32(3): 475-483.
-
Brabin B, Hakimi M, Pelletier D (2001) An Analysis of Anemia and Pregnancy-Related Maternal Mortality. Journal of Nutrition 131(2): 604S-615S.
-
Owa OT, Osifo UC, Anah MU (2017) Iron Status of Infants Born to Anemic Mothers in Benin City, Nigeria. Journal of Applied Hematology 8(3): 99-105.
-
Adewara EO, Okesina AB, Olowookere SA, Jimoh AA (2017) Prevalence and Risk Factors for Anaemia in Pregnancy in Ilorin, Nigeria. European Journal of Obstetrics & Gynecology and Reproductive Biology 219: 65-70.
-
Ezugwu EC, Iyoke CA, Ezugwu FO (2017) Association between Social Support and Antenatal Care Services in Pregnant Women in Enugu, Nigeria. Obstetrics and Gynecology International 2017.
-
Balogun OO, Dagunduro AT, Mohammed MM (2017) Determinants of Antenatal Care Utilization among Pregnant Women in Nigeria. African Health Sciences 17(1): 27-36.
-
Kalaivani K (2009) Prevalence & Consequences of Anaemia in Pregnancy. Indian J Med Res 130(5): 627- 633.
-
Mokuolu OA, Yusuf OB, Oyedeji OA, Orogade AA (2017) Risk Factors for Anaemia in Pregnancy in Nigeria. Journal of Obstetrics and Gynaecology 37(7): 889-894.
-
Oyedeji A, Oyedeji G, Adegun P (2018) Assessment of Factors Influencing Anemia among Pregnant Women attending Antenatal Care in Ile-Ife, Osun State, Nigeria. American Journal of Clinical Nutrition and Metabolism 1(2): 5-12.
-
Ibeh CC, Esin RA, Eke AC (2017) Pregnant Women’s Perception of Antenatal Care Services at the University of Nigeria Teaching Hospital, Enugu. African Journal of Reproductive Health 21(3): 70-79.
-
Ikeanyi EM, Onyeonoro UU, Iwu CD, Uzoigwe UE, Chukwuma EC, et al. (2021) Use of Herbal Medicine among Pregnant Women attending a Tertiary Hospital in Southeastern Nigeria: A Cross-Sectional Study. Journal of Complementary and Integrative Medicine 18(1).
-
Ugwu EO, Olibe AO, Obi SN, Ugwu AO (2018) Determinants of Anemia in Pregnancy among Pregnant Women attending Antenatal Clinic at Federal Teaching Hospital, Abakaliki, Southeast Nigeria. Medicine 97(17).
- Psychogenic Erectile Dysfunction in Late Adulthood: A Case Report on Clinical Intervention and Intimacy Restoration
- Clinical Trials on COVID-19 in 2025: A New Chapter in Global Health Research
- Innovations and Challenges in Contemporary Medical Clinical Trials: An Editorial Perspective
- Innovations and Challenges in Contemporary Medical Clinical Trials: A Critical Perspective
- Reimagining Clinical Trials: The Power of Continuous Feedback from Medical Reports
- Factors Influencing Brain Drain: Perspectives from a Medical School in Turkey